
Download Lectures on Biostatistics (1971). Corrected and searchable version of Google books edition
Download review of Lectures on Biostatistics (THES, 1973).
evidence
This piece is almost identical with today’s Spectator Health article.
This week there has been enormously wide coverage in the press for one of the worst papers on acupuncture that I’ve come across. As so often, the paper showed the opposite of what its title and press release, claimed. For another stunning example of this sleight of hand, try Acupuncturists show that acupuncture doesn’t work, but conclude the opposite: journal fails, published in the British Journal of General Practice).
Presumably the wide coverage was a result of the hyped-up press release issued by the journal, BMJ Acupuncture in Medicine. That is not the British Medical Journal of course, but it is, bafflingly, published by the BMJ Press group, and if you subscribe to press releases from the real BMJ. you also get them from Acupuncture in Medicine. The BMJ group should not be mixing up press releases about real medicine with press releases about quackery. There seems to be something about quackery that’s clickbait for the mainstream media.
As so often, the press release was shockingly misleading: It said
Acupuncture may alleviate babies’ excessive crying Needling twice weekly for 2 weeks reduced crying time significantly
This is totally untrue. Here’s why.
|
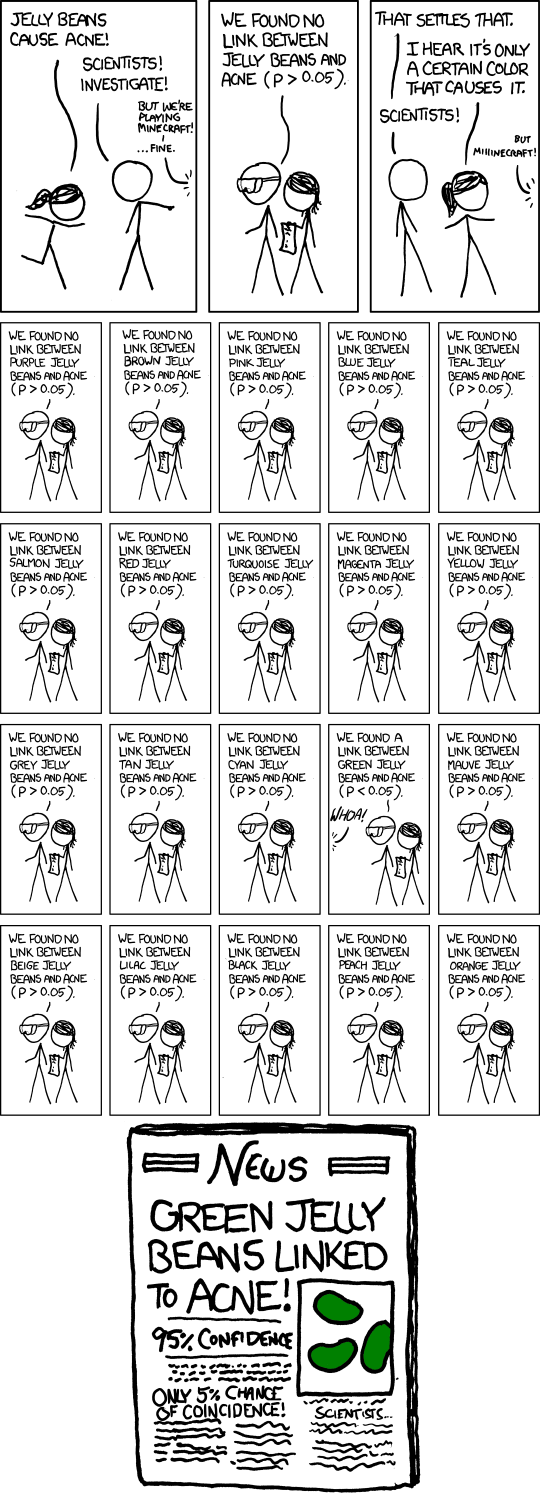
Luckily the Science Media Centre was on the case quickly: read their assessment. The paper made the most elementary of all statistical mistakes. It failed to make allowance for the jelly bean problem. The paper lists 24 different tests of statistical significance and focusses attention on three that happen to give a P value (just) less than 0.05, and so were declared to be "statistically significant". If you do enough tests, some are bound to come out “statistically significant” by chance. They are false postives, and the conclusions are as meaningless as “green jelly beans cause acne” in the cartoon. This is called P-hacking and it’s a well known cause of problems. It was evidently beyond the wit of the referees to notice this naive mistake. It’s very doubtful whether there is anything happening but random variability. And that’s before you even get to the problem of the weakness of the evidence provided by P values close to 0.05. There’s at least a 30% chance of such values being false positives, even if it were not for the jelly bean problem, and a lot more than 30% if the hypothesis being tested is implausible. I leave it to the reader to assess the plausibility of the hypothesis that a good way to stop a baby crying is to stick needles into the poor baby. If you want to know more about P values try Youtube or here, or here. |
|
One of the people asked for an opinion on the paper was George Lewith, the well-known apologist for all things quackish. He described the work as being a "good sized fastidious well conducted study ….. The outcome is clear". Thus showing an ignorance of statistics that would shame an undergraduate.
On the Today Programme, I was interviewed by the formidable John Humphrys, along with the mandatory member of the flat-earth society whom the BBC seems to feel obliged to invite along for "balance". In this case it was professional acupuncturist, Mike Cummings, who is an associate editor of the journal in which the paper appeared. Perhaps he’d read the Science media centre’s assessment before he came on, because he said, quite rightly, that
"in technical terms the study is negative" "the primary outcome did not turn out to be statistically significant"
to which Humphrys retorted, reasonably enough, “So it doesn’t work”. Cummings’ response to this was a lot of bluster about how unfair it was for NICE to expect a treatment to perform better than placebo. It was fascinating to hear Cummings admit that the press release by his own journal was simply wrong.
Listen to the interview here
Another obvious flaw of the study is that the nature of the control group. It is not stated very clearly but it seems that the baby was left alone with the acupuncturist for 10 minutes. A far better control would have been to have the baby cuddled by its mother, or by a nurse. That’s what was used by Olafsdottir et al (2001) in a study that showed cuddling worked just as well as another form of quackery, chiropractic, to stop babies crying.
Manufactured doubt is a potent weapon of the alternative medicine industry. It’s the same tactic as was used by the tobacco industry. You scrape together a few lousy papers like this one and use them to pretend that there’s a controversy. For years the tobacco industry used this tactic to try to persuade people that cigarettes didn’t give you cancer, and that nicotine wasn’t addictive. The main stream media obligingly invite the representatives of the industry who convey to the reader/listener that there is a controversy, when there isn’t.
Acupuncture is no longer controversial. It just doesn’t work -see Acupuncture is a theatrical placebo: the end of a myth. Try to imagine a pill that had been subjected to well over 3000 trials without anyone producing convincing evidence for a clinically useful effect. It would have been abandoned years ago. But by manufacturing doubt, the acupuncture industry has managed to keep its product in the news. Every paper on the subject ends with the words "more research is needed". No it isn’t.
Acupuncture is pre-scientific idea that was moribund everywhere, even in China, until it was revived by Mao Zedong as part of the appalling Great Proletarian Revolution. Now it is big business in China, and 100 percent of the clinical trials that come from China are positive.
if you believe them, you’ll truly believe anything.
Follow-up
29 January 2017
Soon after the Today programme in which we both appeared, the acupuncturist, Mike Cummings, posted his reaction to the programme. I thought it worth posting the original version in full. Its petulance and abusiveness are quite remarkable.
I thank Cummings for giving publicity to the video of our appearance, and for referring to my Wikipedia page. I leave it to the reader to judge my competence, and his, in the statistics of clinical trials. And it’s odd to be described as a "professional blogger" when the 400+ posts on dcscience.net don’t make a penny -in fact they cost me money. In contrast, he is the salaried medical director of the British Medical Acupuncture Society.
It’s very clear that he has no understanding of the error of the transposed conditional, nor even the mulltiple comparison problem (and neither, it seems, does he know the meaning of the word ‘protagonist’).
I ignored his piece, but several friends complained to the BMJ for allowing such abusive material on their blog site. As a result a few changes were made. The “baying mob” is still there, but the Wikipedia link has gone. I thought that readers might be interested to read the original unexpurgated version. It shows, better than I ever could, the weakness of the arguments of the alternative medicine community. To quote Upton Sinclair:
“It is difficult to get a man to understand something, when his salary depends upon his not understanding it.”
It also shows that the BBC still hasn’t learned the lessons in Steve Jones’ excellent “Review of impartiality and accuracy of the BBC’s coverage of science“. Every time I appear in such a programme, they feel obliged to invite a member of the flat earth society to propagate their make-believe.
Acupuncture for infantile colic – misdirection in the media or over-reaction from a sceptic blogger?26 Jan, 17 | by Dr Mike Cummings So there has been a big response to this paper press released by BMJ on behalf of the journal Acupuncture in Medicine. The response has been influenced by the usual characters – retired professors who are professional bloggers and vocal critics of anything in the realm of complementary medicine. They thrive on oiling up and flexing their EBM muscles for a baying mob of fellow sceptics (see my ‘stereotypical mental image’ here). Their target in this instant is a relatively small trial on acupuncture for infantile colic.[1] Deserving of being press released by virtue of being the largest to date in the field, but by no means because it gave a definitive answer to the question of the efficacy of acupuncture in the condition. We need to wait for an SR where the data from the 4 trials to date can be combined. So what about the research itself? I have already said that the trial was not definitive, but it was not a bad trial. It suffered from under-recruiting, which meant that it was underpowered in terms of the statistical analysis. But it was prospectively registered, had ethical approval and the protocol was published. Primary and secondary outcomes were clearly defined, and the only change from the published protocol was to combine the two acupuncture groups in an attempt to improve the statistical power because of under recruitment. The fact that this decision was made after the trial had begun means that the results would have to be considered speculative. For this reason the editors of Acupuncture in Medicine insisted on alteration of the language in which the conclusions were framed to reflect this level of uncertainty. DC has focussed on multiple statistical testing and p values. These are important considerations, and we could have insisted on more clarity in the paper. P values are a guide and the 0.05 level commonly adopted must be interpreted appropriately in the circumstances. In this paper there are no definitive conclusions, so the p values recorded are there to guide future hypothesis generation and trial design. There were over 50 p values reported in this paper, so by chance alone you must expect some to be below 0.05. If one is to claim statistical significance of an outcome at the 0.05 level, ie a 1:20 likelihood of the event happening by chance alone, you can only perform the test once. If you perform the test twice you must reduce the p value to 0.025 if you want to claim statistical significance of one or other of the tests. So now we must come to the predefined outcomes. They were clearly stated, and the results of these are the only ones relevant to the conclusions of the paper. The primary outcome was the relative reduction in total crying time (TC) at 2 weeks. There were two significance tests at this point for relative TC. For a statistically significant result, the p values would need to be less than or equal to 0.025 – neither was this low, hence my comment on the Radio 4 Today programme that this was technically a negative trial (more correctly ‘not a positive trial’ – it failed to disprove the null hypothesis ie that the samples were drawn from the same population and the acupuncture intervention did not change the population treated). Finally to the secondary outcome – this was the number of infants in each group who continued to fulfil the criteria for colic at the end of each intervention week. There were four tests of significance so we need to divide 0.05 by 4 to maintain the 1:20 chance of a random event ie only draw conclusions regarding statistical significance if any of the tests resulted in a p value at or below 0.0125. Two of the 4 tests were below this figure, so we say that the result is unlikely to have been chance alone in this case. With hindsight it might have been good to include this explanation in the paper itself, but as editors we must constantly balance how much we push authors to adjust their papers, and in this case the editor focussed on reducing the conclusions to being speculative rather than definitive. A significant result in a secondary outcome leads to a speculative conclusion that acupuncture ‘may’ be an effective treatment option… but further research will be needed etc… Now a final word on the 3000 plus acupuncture trials that DC loves to mention. His point is that there is no consistent evidence for acupuncture after over 3000 RCTs, so it clearly doesn’t work. He first quoted this figure in an editorial after discussing the largest, most statistically reliable meta-analysis to date – the Vickers et al IPDM.[2] DC admits that there is a small effect of acupuncture over sham, but follows the standard EBM mantra that it is too small to be clinically meaningful without ever considering the possibility that sham (gentle acupuncture plus context of acupuncture) can have clinically relevant effects when compared with conventional treatments. Perhaps now the best example of this is a network meta-analysis (NMA) using individual patient data (IPD), which clearly demonstrates benefits of sham acupuncture over usual care (a variety of best standard or usual care) in terms of health-related quality of life (HRQoL).[3] |
30 January 2017
I got an email from the BMJ asking me to take part in a BMJ Head-to-Head debate about acupuncture. I did one of these before, in 2007, but it generated more heat than light (the only good thing to come out of it was the joke about leprechauns). So here is my polite refusal.
|
Hello Thanks for the invitation, Perhaps you should read the piece that I wrote after the Today programme Why don’t you do these Head to Heads about genuine controversies? To do them about homeopathy or acupuncture is to fall for the “manufactured doubt” stratagem that was used so effectively by the tobacco industry to promote smoking. It’s the favourite tool of snake oil salesman too, and th BMJ should see that and not fall for their tricks. Such pieces night be good clickbait, but they are bad medicine and bad ethics. All the best David |
A constant theme of this blog is that the NHS should not pay for useless treatments. By and large, NICE does a good job of preventing that. But NICE has not been allowed by the Department of Health to look at quackery.
I have the impression that privatisation of many NHS services will lead to an increase in the provision of myth-based therapies. That is part of the "bait and switch" tactic that quacks use in the hope of gaining respectability. A prime example is the "College of Medicine", financed by Capita and replete with quacks, as one would expect since it is the reincarnation of the Prince’s Foundation for Integrated Health.
One such treatment is acupuncture. Having very recently reviewed the evidence, we concluded that "Acupuncture is a theatrical placebo: the end of a myth". Any effects it may have are too small to be useful to patients. That’s the background for an interesting case study.
A colleague got a very painful frozen shoulder. His GP referred him to the Camden & Islington NHS Trust physiotherapy service. That service is now provided by a private company, Connect Physical Health.
That proved to be a big mistake. The first two appointments were not too bad, though they resulted in little improvement. But at the third appointment he was offered acupuncture. He hesitated, but agreed, in desperation to try it. It did no good. At the next appointment the condition was worse. After some very painful manipulation, the physiotherapist offered acupuncture again. This time he refused on the grounds that "I hadn’t noticed any effect the first time, because there is no evidence that it works and that I was concerned by her standards of hygiene". The physiotherapist then became "quite rude" and said that she would put down that the patient had refused treatment.
The lack of response was hardly surprising. NHS Evidence says
"There is no clinical evidence to show that other treatments, such as transcutaneous electrical nerve stimulation (TENS), Shiatsu massage or acupuncture are effective in treating frozen shoulder."
In fact it now seems beyond reasonable doubt that acupuncture is no more than a theatrical placebo.
According to Connect’s own web site “Our services are evidence-based”. That is evidently untrue in this case, so I asked them for the evidence that acupuncture was effective.
I’d noticed that in other places, Connect Physical Health also offers the obviously fraudulent craniosacral therapy (for example, here) and discredited chiropractic quackery. So I asked them about the evidence for their effectiveness too.
This is what they said.
|
Many thanks for your comments via our web site. In response, we thought you might like to access the sources for some of the evidence which underpins our MSK services: Integrating Evidence-Based Acupuncture into Physiotherapy for the Benefit of the Patient – you can obtain the information you require from www.aacp.org.uk The General Chiropractic Council www.gcc-uk.org/page.cfm We have also attached a copy of the NICE Guidelines. |
So, no Cochrane reviews, no NHS Evidence. Instead I was referred to the very quack organisations that promote the treatments in question, the Acupuncture Association of Chartered Physiotherapists, and the totally discredited General Chiropractic Council.
The NICE guidelines that they sent were nothing to do with frozen shoulder. They were the guidelines for low back pain which caused such a furore when they were first issued (and which, in any case, don’t recommend chiropractic explicitly).
When I pointed out these deficiencies I got this.
|
Your email below has been forwarded to me. I am sorry if you feel that that that information we pointed you towards to enable you to make your own investigations into the evidence base for the services provided by Connect Physical Health and your hospital did not meet with your expectations. ‘ ‘ ‘ Please understand that our NHS services in Camden were commissioned by the Primary Care Trust. The fully integrated MSK service model included provision for acupuncture and other manual therapy provided by our experienced Chartered Physiotherapists. If you have any problems with the evidence base for the use of acupuncture or manual therapy within the service, which has been commissioned on behalf of the GPs in Camden Borough, then I would politely recommend that you direct your observations to the clinical commissioning authorities and other professional bodies who do spend time evidencing best practice and representing the academic arguments. I am sure they will be pleased to pick up discussions with you about the relative merits of the interventions being procured by the NHS. Yours sincerely, Mark Mark Philpott BSc BSc MSc MMACP MCSP
Head of Operations, Community MSK Services Connect Physical Health 35 Apex Business Village Cramlington Northumberland NE23 7BF |
So, "don’t blame us, blame the PCT". A second letter asked why they were shirking the little matter of evidence.
|
In response to your last email, I would like to say that Connect does not wish to be drawn into a debate over two therapeutic options (acupuncture and craniosacral therapy) that are widely practiced [sic] within and outside the NHS by very respectable practitioners. You will be as aware, as Connect is, that there are lots of treatments that don’t have a huge evidence base that are practiced in mainstream medicine. Connect has seen many carefully selected patients helped by acupuncture and manual therapy (craniosacral therapy / chiropractic) over many years. Lack of evidence doesn’t mean they don’t work, just that benefit is not proven. Furthermore, nowhere on our website do we state that ALL treatments / services / modalities that Connect offer are ‘Evidence Based’. We do however offer many services that are evidence based, where the evidence exists. We aim to offer ‘choice’ to patients, from a range of services that are safe and delivered by suitably trained professionals and practitioners in line with Codes of Practice and Guidelines from the relevant governing bodies. Connect’s service provision in Camden is meticulously assessed and of a high standard and we are proud of the services provided. |
This response is so wrong, on so many levels, that I gave up on Mr Philpott at this point. At least he admitted implicitly that all of their treatments are not evidence-based. In that case their web site needs to change that claim.
If, by "governing bodies" he means jokes like the GCC or the CNHC then I suppose the behaviour of their employees is not surprising. Mr Philpott is evidently not aware that "craniosacral therapy" has been censured by the Advertising Standards Authority. Well he is now, but evidently doesn’t seem to give a damn.
Next I wrote to the PCT and it took several mails to find out who was responsible for the service. Three mails produced no response so I sent a Freedom of Information Act request. In the end I got some
"Connect PHC provide the Community musculoskeletal service for Camden. The specification for the service specifically asks for the provision of evidence based management and treatments see paragraph on Governance page 14 of attached.. Patients are treated with acupuncture as per the NICE Guidelines (May 2009) for the management of low back pain … . .. Chiropractors are not employed in the service and craniosacral therapy is not provided as part of the service either."
Another letter, pointing out that they were using acupuncture for things other than low back pain got no more information. They did send a copy of the contract with Connect. It makes no mention whatsoever of alternative treatments. It should have done, so part of the responsibility for the failure must lie with the PCT.
The contract does, however, say (page 18)
The service to be led by a lead clinician/manager who can effectively demonstrate ongoing and evidence-based development of clinical guidelines, policies and protocols for effective working practices within the service
In my opinion, Connect Physical Health are in breach of contract
Another example of Connect ignoring evidence
The Connect Physical Health web site has an article about osteoarthritis of the knee
Physiotherapy can be extremely beneficial to help to reduce the symptoms of OA. Treatments such as mobilizations, rehab exercises, acupuncture and taping can help to reduce pain, increase range of movement, increase muscle strength and aid return to functional activities and sports.
There is little enough evidence that physiotherapy does any of these things, but at least it is free of mystical mumbo-jumbo. Although at one time the claim for acupuncture was thought to have some truth, the 2010 Cochrane review concludes otherwise
Sham-controlled trials show statistically significant benefits; however, these benefits are small, do not meet our pre-defined thresholds for clinical relevance, and are probably due at least partially to placebo effects from incomplete blinding.
This conclusion is much the same as has been reached for acupuncture treatments of almost everything. Two major meta-analyses come to similar conclusions. Madsen Gøtzsche & Hróbjartsson (2009) and Vickers et al (2012) both conclude that if there is an effect at all (dubious) then it is too small to be noticeable to the patient. (Be warned that in the case of Vickers et al. you need to read the paper itself because of the spin placed on the results in the abstract.). These papers are discussed in detail in our recent paper.
Why is Connect Physical Health not aware of this?
Their head of operations told me (see above) that
"Connect does not wish to be drawn into a debate [about acupuncture and craniosacral therapy]".
That outlook was confirmed when I left a comment on their osteoarthritis post. This is what it looked like almost a month later.
Guess what? The comment has never appeared..
The attitude of Connect Physical Health to evidence is simply to ignore it if it gets in the way of making money, and to censor any criticism.
What have Camden NHS done about it?
The patient and I both complained to Camden NHS in August 2012. At first, they simply forwarded the complaints to Connect Physical Health with the unsatisfactory results shown above. It took until May 2013 to get any sort of reasonable response. That seems a very long time. In fact by the time the response arrived the PCT had been renamed a Clinical Commissioning Group (CCG) because of the vast top-down reorganisation inposed by Lansley’s Health and Social Care Act.
On 8 May 2013, this response was sent to the patient, Here is part of it.
|
I have received your email of complaint from the NHSNCL complaints department regarding your care. You raise some very clear concerns and I will attempt to address these in order. 1) The fact that you felt pressurised into having acupuncture is a concern as everybody should be given a choice. As part of the informed consent relating to acupuncture you should have been told about the treatment, it’s [sic] benefits and risks and then you sign to confirm you are happy to proceed. I understand that this was the case in your situation but I have reinforced that the consent is important and must be adhered to by the provider Connect Physical Health. There are clear standards of clinical practice that all Chartered Physiotherapists must follow which I will discuss further with the Connect Camden team Manager Nick Downing. I do disagree with you around acupuncture; there is no conclusive evidence for acupuncture in frozen shoulder but I have referenced a systematic review which concludes the studies were too small to draw any conclusions although shoulder function was significantly improved at 4 weeks (Green S et al. Acupuncture for shoulder pain. Cochrane Database Syst Rev 2005; 18: CD005319). There is a growing body of evidence supporting the use of acupuncture and until such time as there is specific evidence against it I don’t think we would be absolutely against the practice of this modality alongside other treatments. .Best wishes Strategy and Planning Directorate |
This response raises more questions than it answers.
For example, what is "informed consent" worth if the therapist is his/herself misinformed about the treatment? It is the eternal dilemma of alternative medicine that it is no use referring to well-trained practitioners, when their training has inculcated myths and untruths.
There is not a "growing body of evidence supporting the use of acupuncture". Precisely the opposite is true.
And the statement "until such time as there is specific evidence against it I don’t think we would be absolutely against the practice of this modality alongside" betrays a basic misunderstanding of the scientific process.
So I sent the writer of this letter a reprint of our paper, "Acupuncture is a theatrical placebo: the end of a myth" (the blog version alone has had over 12,000 page views). A few days later we had an amiable lunch together and we had a constructive discussion about the problems of deciding what should be commissioned and what shouldn’t.
It seems to me to be clear that CCGs should take better advice before boasting that they commission evidence-based treatments.
Postscript
Stories like this are worrying to the majority of physiotherapists who don’t go in for mystical mumbo-jumbo of acupuncture. One of the best is Neil O’Connell who blogs at BodyInMind. He tweeted
Physio fail, sigh RT@david_colquhoun: Yet more #acupuncture. Sold to the NHS by private contractor @ConnectPHC http://t.co/HylkwMCVTh
— Neil O'Connell (@NeilOConnell) June 10, 2013
It isn’t clear how many physiotherapists embrace nonsense, but the Acupuncture Association of Chartered Physiotherapists has around 6000 members, compared with 47,000 chartered physiotherapists (AACP), so it’s a smallish minority. The AACP claims that it is “Integrating Evidence-Based Acupuncture into Physiotherapy”. Like most politicians, the term “evidence-based” is thrown around with gay abandon. Clearly they don’t understand evidence.
Follow-up
12 June 2013
The Advertising Standards Authority has, one again, upheld complaints against the UCLH Trust, for making false claims in its advertising. This time, appropriately, it’s about acupuncture. Just about everything in their advertising leaflets was held to be unjustifiable. They’ve been in trouble before about false claims for homeopathy, hypnosis and craniosacral "therapy".
Of course all of these embarrassments come from one very small corner of the UCLH Trust, the Royal London Hospital for Integrated Medicine (previously known as the Royal London Homeopathic Hospital).
Why is it tolerated in an otherwise excellent NHS Trust? Well, the patron is the Queen herself (not Charles, aka the Quacktitioner Royal), She seems to exert more power behind the scenes than is desirable in In a constitutional monarchy
29 June 2013
I wrote to Dr Gill Gaskin about the latest ASA judgement against RLHIM. She is the person at the UCLH Trust who has responsibility for the quack hospital. She previously refused to do anything about the craniosacral nonsense that is promoted there. This time the ASA seems to have stung them into action at long last. I was told
|
In response to your question about proposed action: All written information for patients relating to the services offered by the Royal London Hospital for Integrated Medicine are being withdrawn for review in the light of the ASA’s rulings (and the patient leaflets have already been withdrawn). It will be reviewed and modified where necessary item by item, and only reintroduced after sign-off through the Queen Square divisional clinical governance processes and the Trust’s patient information leaflet team. With best wishes Gill Gaskin Dr Gill Gaskin |
It remains to be seen whether the re-written information is accurate or not.
The rules for advertising
The Advertising Standards Authority gives advice for advertisers about what’s permitted and what isn’t.
Acupuncture The CAP advice
Craniosacral therapy The CAP advice
Homeopathy The CAP advice and 2013 update
Chiropractic The CAP advice.
This article has been re-posted on The Winnower, so it now has a digital object identifier: DOI: 10.15200/winn.142935.50603
The latest news: eating red meat doesn’t do any harm. But why isn’t that said clearly? Alarmism makes better news, not only for journalists but for authors and university PR people too.
I’ve already written twice about red meat.
In May 2009 Diet and health. What can you believe: or does bacon kill you? based on the WCRF report (2007).
In March 2012 How big is the risk from eating red meat now? An update.
In the first of these I argued that the evidence produced by the World Cancer Research Fund (WCRF) for a causal relationship was very thin indeed. An update by WCRF in 2010 showed a slightly smaller risk, and weakened yet further the evidence for causality, though that wasn’t reflected in their press announcement.
The 2012 update added observations from two very large cohort studies. The result was that the estimates of risk were less than half as big as in 2009. The relative risk of dying from colorectal cancer was 1.21 (95% Confidence interval 1.04–1.42) with 50 g of red or processed meat per day, whereas in the new study the relative risk for cancer was only 1.10 (1.06-1.14) for a larger ‘dose’, 85 g of red meat. Again this good news was ignored and dire warnings were issued.
This reduction in size of the effect as samples get bigger is exactly what’s expected for spurious correlations, as described by Ioannidis and others. And it seems to have come true. The estimate of the harm done by red meat has vanished entirely in the latest study.
The EPIC study
This is the European Prospective Investigation into Cancer and Nutrition, another prospective cohort study, so it isn’t randomised [read the original paper]. And it was big, 448,568 people from ten different European countries. These people were followed for a median time of 12.7 years, and during follow-up 26,344 of them died.
The thing that was different about this paper was that red meat was found to pose no detectable risk, as judged by all-cause mortality. But this wasn’t even mentioned in the headline conclusions.
Conclusions: The results of our analysis support a moderate positive association between processed meat consumption and mortality, in particular due to cardiovascular diseases, but also to cancer.
To find the result you have to dig into Table 3.
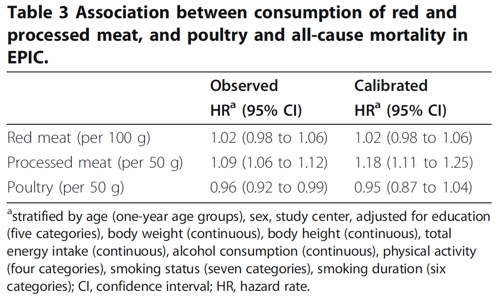
So, by both methods of calculation, the relative risk from eating red meat is negligible (except possibly in the top group, eating more than 160 g (7 oz) per day).
There is still an association between intake of processed meat and all-cause mortality, as in previous studies, though the association of processed meat with all-cause mortality, 1.09, or 1.18 depending on assumptions, is, if anything, smaller than was observed in the 2012 study, in which the relative risk was 1.20 (Table 2).
Assumptions, confounders and corrections.
The lowest meat eaters had only 13% of current smokers, but for the biggest red meat eaters it was 40%, for males. The alcohol consumption was 8.2 g/day for the lowest meat eaters but 23.4 g/day for the highest-meat group (the correlations were a bit smaller for women and also for processed meat eaters).
These two observations necessitate huge corrections to remove the (much bigger) effects of smoking and drinking if we want find the association for meat-eating alone. The main method for doing the correction is to fit the Cox proportional hazards model. This model assumes that there are straight-line relationships between the logarithm of the risk and the amount of each of the risk factors, e.g smoking, drinking, meat-eating and other risk factors. It may also include interactions that are designed to detect whether, for example, the effect of smoking on risk is or isn’t the same for people who drink different amounts.
Usually the straight-line assumption isn’t tested, and the results will depend on which risk factors (and which interactions between them) are included in the calculations. Different assumptions will give different answers. It simply isn’t known how accurate the corrections are when trying to eliminate the big effect of smoking in order to isolate the small effect of meat-eating. And that is before we get to other sorts of correction. For example, the relative risk from processed meat in Table 3, above, was 9% or 18% (1.09, or 1.18) depending on the outcome of a calculation that was intended to increase the accuracy of food intake records ("calibration").
The Conclusions of the new study don’t even mention the new result with red meat. All they mention is the risk from processed meat.
In this population, reduction of processed meat consumption to less than 20 g/day would prevent more than 3% of all deaths. As processed meat consumption is a modifiable risk factor, health promotion activities should include specific advice on lowering processed meat consumption.
Well, you would save that number of lives if, and only if, the processed meat was the cause of death. Too many epidemiologists, the authors pay lip service to the problem of causality in the introduction, but then go on to assume it in the conclusions. In fact the problem of causality isn’t even metnioned anywhere in either the 2012 study, or the new 2013 EPIC trial.
So is the risk of processed meat still real? Of course I can’t answer that. All that can be said is that it’s quite small, and as sample sizes get bigger, estimates of the risk are getting smaller. It wouldn’t be surprising if the risk from processed meat were eventually found not to exist, just as has happened for red (unprocessed) meat
The Japanese study
Last year there was another cohort study, with 51,683 Japanese. The results were even more (non-) dramatic [Nagao et al, 2012] than in the EPIC trial. This is how they summarise the results for the relative risks (with 95% confidence intervals).
"…for the highest versus lowest quintiles of meat consumption (77.6 versus 10.4 g/day) among men were 0.66 (0.45 — 0.97) for ischemic heart disease, 1.10 (0.84 — 1.43) for stroke and 1.00 (0.84 — 1.20) for total cardiovascular disease. The corresponding HRs (59.9 versus 7.5 g/day) among women were 1.22 (0.81 — 1.83), 0.91 (0.70 — 1.19) and 1.07 (0.90 — 1.28). The associations were similar when the consumptions of red meat, poultry, processed meat and liver were examined separately.
CONCLUSION: Moderate meat consumption, up to about 100 g/day, was not associated with increased mortality from ischemic heart disease, stroke or total cardiovascular disease among either gender."
In this study, the more meat (red or processed) you eat, the lower your risk of ischaemic heart disease (with the possible exception of overweight women). The risk of dying from any cardiovascular disease was unrelated to the amount of meat eaten (relative risk 1.0) whether processed meat or not.
Of course it’s possible that things which risky for Japanese people differ from those that are risky for Europeans. It’s also possible that even processed meat isn’t bad for you.
The carnitine study
The latest meat study to hit the headlines didn’t actually look at the effects of meat at all, though you wouldn’t guess that from the pictures of sausages in the headlines (not just in newspapers, but also in NHS Choices). The paper [reprint] was about carnitine, a substance that occurs particularly in beef, with lower amounts in pork and bacon, and in many other foods. The paper showed that bacteria in the gut can convert carnitine to a potentially toxic substance, trimethylamine oxide (TMAO). That harms blood vessels (at least in mice). But to show an effect in human subjects they were given an amount of carnitine equivalent to over 1 lb of steak, hardly normal, even in the USA.
The summary of the paper says it is an attempt to explain "the well-established link between high levels of red meat consumption and CVD [cardiovascular disease] risk". As we have just seen, it seems likely that this risk is far from being “well-established”. There is little or no such risk to explain.
It would be useful to have a diagnostic marker for heart disease, but this paper doesn’t show that carnitine or TMAO) is useful for that. It might also be noted that the authors have a maze of financial interests.
Competing financial interests Z.W. and B.S.L. are named as co-inventors on pending patents held by the Cleveland Clinic relating to cardiovascular diagnostics and have the right to receive royalty payments for inventions or discoveries related to cardiovascular diagnostics from Liposciences. W.H.W.T. received research grant support from Abbott Laboratories and served as a consultant for Medtronic and St. Jude Medical. S.L.H. and J.D.S. are named as co-inventors on pending and issued patents held by the Cleveland Clinic relating to cardiovascular diagnostics and therapeutics patents. S.L.H. has been paid as a consultant or speaker by the following companies: Cleveland Heart Lab., Esperion, Liposciences, Merck & Co. and Pfizer. He has received research funds from Abbott, Cleveland Heart Lab., Esperion and Liposciences and has the right to receive royalty payments for inventions or discoveries related to cardiovascular diagnostics from Abbott Laboratories, Cleveland Heart Lab., Frantz Biomarkers, Liposciences and Siemens.
The practical significance of this work was summed up the dietitian par excellence, Catherine Collins, on the BBC’s Inside Health programme.
Listen to Catherine Collins on carnitine.
She points out that the paper didn’t mean that we should change what we already think is a sensible diet.
At most, it suggests that it’s not a good idea to eat 1 lb steaks very day.
And the paper does suggest that it’s not sensible to take the carnitine supplements that are pushed by every gym. According to NIH
"twenty years of research finds no consistent evidence that carnitine supplements can improve exercise or physical performance in healthy subjects".
Carnitine supplements are a scam. And they could be dangerous.
Follow-up
Another blog on this topic, one from Cancer Research UK also fails to discuss the problem of causality. Neither does it go into the nature (and fallibility) of the corrections for counfounders like smoking and alcohol,. Nevertheless that, and an earlier post on Food and cancer: why media reports are often misleading, are a good deal more realistic than most newspaper reports.
The Scottish Universities Medical Journal asked me to write about the regulation of alternative medicine. It’s an interesting topic and not easy to follow because of the veritable maze of more than twenty overlapping regulators and quangos which fail utterly to protect the public against health fraud. In fact they mostly promote health fraud. The paper is now published, and here is a version with embedded links (and some small updates).
We are witnessing an increasing commercialisation of medicine. It’s really taken off since the passage of the Health and Social Security Bill into law. Not only does that mean having NHS hospitals run by private companies, but it means that “any qualified provider” can bid for just about any service. The problem lies, of course, in what you consider “qualified” to mean. Any qualified homeopath or herbalist will, no doubt, be eligible. University College London Hospital advertised for a spiritual healer. The "person specification" specified a "quallfication", but only HR people think that a paper qualification means that spiritual healing is anything but a delusion.
The vocabulary of bait and switch
First, a bit of vocabulary. Alternative medicine is a term that is used for medical treatments that don’t work (or at least haven’t been shown to work). If they worked, they’d be called “medicine”. The anti-malarial, artemesinin, came originally from a Chinese herb, but once it had been purified and properly tested, it was no longer alternative. But the word alternative is not favoured by quacks. They prefer their nostrums to be described as “complementary” –it sounds more respectable. So CAM (complementary and alternative medicine became the politically-correct euphemism. Now it has gone a stage further, and the euphemism in vogue with quacks at the moment is “integrated” or “integrative” medicine. That means, very often, integrating things that don’t work with things that do. But it sounds fashionable. In reality it is designed to confuse politicians who ask for, say, integrated services for old people.
Put another way, the salespeople of quackery have become rather good at bait and switch. The wikepedia definition is as good as any.
Bait-and-switch is a form of fraud, most commonly used in retail sales but also applicable to other contexts. First, customers are “baited” by advertising for a product or service at a low price; second, the customers discover that the advertised good is not available and are “switched” to a costlier product.
As applied to the alternative medicine industry, the bait is usually in the form of some nice touchy-feely stuff which barely mentions the mystical nonsense. But when you’ve bought into it you get the whole panoply of nonsense. Steven Novella has written eloquently about the use of bait and switch in the USA to sell chiropractic, acupuncture, homeopathy and herbal medicine: "The bait is that CAM offers legitimate alternatives, the switch is that it primarily promotes treatments that don’t work or are at best untested and highly implausible.".
The "College of Medicine" provides a near-perfect example of bait and switch. It is the direct successor of the Prince of Wales’ Foundation for Integrated Health. The Prince’s Foundation was a consistent purveyor of dangerous medical myths. When it collapsed in 2010 because of a financial scandal, a company was formed called "The College for Integrated Health". A slide show, not meant for public consumption, said "The College represents a new strategy to take forward the vision of HRH Prince Charles". But it seems that too many people have now tumbled to the idea that "integrated", in this context, means barmpottery. Within less than a month, the new institution was renamed "The College of Medicine". That might be a deceptive name, but it’s a much better bait. That’s why I described the College as a fraud and delusion.
Not only did the directors, all of them quacks, devise a respectable sounding name, but they also succeeded in recruiting some respectable-sounding people to act as figureheads for the new organisation. The president of the College is Professor Sir Graham Catto, emeritus professor of medicine at the University of Aberdeen. Names like his make the bait sound even more plausible. He claims not to believe that homeopathy works, but seems quite happy to have a homeopathic pharmacist, Christine Glover, on the governing council of his college. At least half of the governing Council can safely be classified as quacks.
So the bait is clear. What about the switch? The first thing to notice is that the whole outfit is skewed towards private medicine: see The College of Medicine is in the pocket of Crapita Capita. The founder, and presumably the main provider of funds (they won’t say how much) is the huge outsourcing company, Capita. This is company known in Private Eye as Crapita. Their inefficiency is legendary. They are the folks who messed up the NHS computer system and the courts computer system. After swallowing large amounts of taxpayers’ money, they failed to deliver anything that worked. Their latest failure is the court translation service.. The president (Catto), the vice president (Harry Brunjes) and the CEO (Mark Ratnarajah) are all employees of Capita.
The second thing to notice is that their conferences and courses are a bizarre mixture of real medicine and pure quackery. Their 2012 conference had some very good speakers, but then it had a "herbal workshop" with Simon Mills (see a video) and David Peters (the man who tolerates dowsing as a way to diagnose which herb to give you). The other speaker was Dick Middleton, who represents the huge herbal company, Schwabe (I debated with him on BBC Breakfast), In fact the College’s Faculty of Self-care appears to resemble a marketing device for Schwabe.
Why regulation isn’t working, and can’t work
There are various levels of regulation. The "highest" level is the statutory regulation of osteopathy and chiropractic. The General Chiropractic Council (GCC) has exactly the same legal status as the General Medical Council (GMC). This ludicrous state of affairs arose because nobody in John Major’s government had enough scientific knowledge to realise that chiropractic, and some parts of osteopathy, are pure quackery,
The problem is that organisations like the GCC function more to promote chiropractic than to regulate them. This became very obvious when the British Chiropractic Association (BCA) decided to sue Simon Singh for defamation, after he described some of their treatments as “bogus”, “without a jot of evidence”.
In order to support Singh, several bloggers assessed the "plethora of evidence" which the BCA said could be used to justify their claims. When, 15 months later, the BCA produced its "plethora" it was shown within 24 hours that the evidence was pathetic. The demolition was summarised by lawyer, David Allen Green, in The BCA’s Worst Day.
In the wake of this, over 600 complaints were made to the GCC about unjustified claims made by chiropractors, thanks in large part to heroic work by two people, Simon Perry and Allan Henness. Simon Perry’s Fishbarrel (browser plugin) allows complaints to be made quickly and easily -try it). The majority of these complaints were rejected by the GCC, apparently on the grounds that chiropractors could not be blamed because the false claims had been endorsed by the GCC itself.
My own complaint was based on phone calls to two chiropractors, I was told such nonsense as "colic is down to, er um, faulty movement patterns in the spine". But my complaint never reached the Conduct and Competence committee because it had been judged by a preliminary investigating committee that there was no case to answer. The impression one got from this (very costly) exercise was that the GCC was there to protect chiropractors, not to protect the public.
The outcome was a disaster for chiropractors, wno emerged totally discredited. It was also a disaster for the GCC which was forced to admit that it hadn’t properly advised chiropractors about what they could and couldn’t claim. The recantation culminated in the GCC declaring, in August 2010, that the mythical "subluxation" is a "historical concept " "It is not supported by any clinical research evidence that would allow claims to be made that it is the cause of disease.". Subluxation was a product of the fevered imagination of the founder of the chiropractic cult, D.D. Palmer. It referred to an imaginary spinal lesion that he claimed to be the cause of most diseases. .Since ‘subluxation’ is the only thing that’s distinguished chiropractic from any other sort of manipulation, the admission by the GCC that it does not exist, after a century of pretending that it does, is quite an admission.
The President of the BCA himself admitted in November 2011
“The BCA sued Simon Singh personally for libel. In doing so, the BCA began one of the darkest periods in its history; one that was ultimately to cost it financially,”
As a result of all this, the deficiencies of chiropractic, and the deficiencies of its regulator were revealed, and advertisements for chiropractic are somewhat less misleading. But this change for the better was brought about entirely by the unpaid efforts of bloggers and a few journalists, and not at all by the official regulator, the GCC. which was part of the problem. not the solution. And it was certainly not helped by the organisation that is meant to regulate the GCC, the Council for Health Regulatory Excellence (CHRE) which did nothing whatsoever to stop the farce.
At the other end of the regulatory spectrum, voluntary self-regulation, is an even worse farce than the GCC. They all have grand sounding "Codes of Practice" which, in practice, the ignore totally.
The Society of Homeopaths is just a joke. When homeopaths were caught out recommending sugar pills for prevention of malaria, they did nothing (arguably such homicidal advice deserves a jail sentence).
The Complementary and Natural Healthcare Council (CNHC) is widely know in the blogosphere as Ofquack. I know about them from the inside, having been a member of their Conduct and Competence Committee, It was set up with the help of a £900,000 grant from the Department of Health to the Prince of Wales, to oversee voluntary self-regulation. It fails utterly to do anything useful.. The CNHC code of practice, paragraph 15 , states
“Any advertising you undertake in relation to your professional activities must be accurate. Advertisements must not be misleading, false, unfair or exaggerated”.
When Simon Perry made a complaint to the CNHC about claims being made by a CNHC-registered reflexologist, the Investigating Committee upheld all 15 complaints. But it then went on to say that there was no case to answer because the unjustified claims were what the person had been taught, and were made in good faith.
This is precisely the ludicrous situation which will occur again and again if reflexologists (and many other alternative therapies) are “accredited”. The CNHC said, correctly, that the reflexologist had been taught things that were not true, but then did nothing whatsoever about it apart from toning down the advertisements a bit. They still register reflexologists who make outrageously false claims.
Once again we see that no sensible regulation is possible for subjects that are pure make-believe.
The first two examples deal (or rather, fail to deal) with regulation of outright quackery. But there are dozens of other quangos that sound a lot more respectable.
European Food Standards Agency (EFSA). One of the common scams is to have have your favourite quack treatment classified as a food not as a medicine. The laws about what you can claim have been a lot laxer for foods. But the EFSA has done a pretty good job in stopping unjustified claims for health benefits from foods. Dozens of claims made by makers of probiotics have been banned. The food industry, needless to say, objects very strongly to be being forced to tell the truth. In my view, the ESFA has not gone far enough. They recently issued a directive about claims that could legally be made. Some of these betray the previously high standards of the EFSA. For example you are allowed to say that "Vitamin C contributes to the reduction of tiredness and fatigue" (as long as the product contains above a specified amount of Vitamin C. I’m not aware of any trials that show vitamin C has the slightest effect on tiredness or fatigue, Although these laws do not come into effect until December 2012, they have already been invoked by the ASA has a reason not to uphold a complaint about a multivitamin pill which claimed that it “Includes 8 nutrients that can contribute to the reduction in tiredness and fatigue”
The Advertising Standards Authority (ASA). This is almost the only organisation that has done a good job on false health claims. Their Guidance on Health Therapies & Evidence says
"Whether you use the words ‘treatment’, ‘treat’ or ‘cure’, all are likely to be seen by members of the public as claims to alleviate effectively a condition or symptom. We would advise that they are not used"
"Before and after’ studies with little or no control, studies without human subjects, self-assessment studies and anecdotal evidence are unlikely to be considered acceptable"
"Before and after’ studies with little or no control, studies without human subjects, self-assessment studies and anecdotal evidence are unlikely to be considered acceptable"
They are spot on.
The ASA’s Guidance for Advertisers of Homeopathic Services is wonderful.
"In the simplest terms, you should avoid using efficacy claims, whether implied or direct,"
"To date, the ASA has have not seen persuasive evidence to support claims that homeopathy can treat, cure or relieve specific conditions or symptoms."
That seems to condemn the (mis)labelling allowed by the MHRA as breaking the rules.. Sadly, though, the ASA has no powers to enforce its decisions and only too often they are ignored. The Nightingale collaboration has produced an excellent letter that you can hand to any pharmacist who breaks the rules
The ASA has also judged against claims made by "Craniosacral therapists" (that’s the lunatic fringe of osteopathy). They will presumably uphold complaints about similar claims made (I’m ashamed to say) by UCLH Hospitals.
The private examination company Edexcel sets exams in antiscientific subjects, so miseducating children. The teaching of quackery to 16 year-olds has been approved by a maze of quangos, none of which will take responsibility, or justify their actions. So far I’ve located no fewer than eight of them. The Office of the Qualifications and Examinations Regulator (OfQual), Edexcel, the Qualifications and Curriculum Authority (QCA), Skills for Health, Skills for Care, National Occupational Standards (NOS), private exam company VTCT and the schools inspectorate, Ofsted.. Asking any of these people why they approve of examinations in imaginary subjects meets with blank incomprehension. They fail totally to protect tha public from utter nonsense.
The Department of Education has failed to do anything about the miseducation of children in quackery. In fact it has encouraged it by, for the first time, giving taxpayers’ money to a Steiner (Waldorf) school (at Frome, in Somerset). Steiner schools are run by a secretive and cult-like body of people (read about it). They teach about reincarnation, karma, gnomes, and all manner of nonsense, sometimes with unpleasant racial overtones. The teachers are trained in Steiner’s Anthroposophy, so if your child gets ill at school they’ll probably get homeopathic sugar pills. They might well get measles or mumps too, since Steiner people don’t believe in vaccination.
Incredibly, the University of Aberdeen came perilously close to appointing a chair in anthroposophical medicine. This disaster was aborted by bloggers, and a last minute intervention from journalists. Neither the university’s regulatory mechanisms. nor any others, seemed to realise that a chair in mystical barmpottery was a bad idea.
Trading Standards offices and the Office of Fair Trading.
It is the statutory duty of Trading Standards to enforce the Consumer Protection Regulations (2008) This European legislation is pretty good. it caused a lawyer to write " Has The UK Quietly Outlawed “Alternative” Medicine?". Unfortunately Trading Standards people have consistently refused to enforce these laws. The whole organisation is a mess. Its local office arrangement fails totally to deal with the age of the internet. The situation is so bad that a group of us decided to put them to the test. The results were published in the Medico-Legal Journal, Rose et al., 2012. "Spurious Claims for Health-care Products: An Experimental Approach to Evaluating Current UK Legislation and its Implementation". They concluded "EU directive 2005/29/EC is
largely ineffective in preventing misleading health claims for consumer products in
the UK"
Skills for Health is an enormous quango which produces HR style "competences" for everything under the son. They are mostly quite useless. But those concerned with alternative medicine are not just useless. They are positively harmful. Totally barmy. There are competences and National Occupational Standards for every lunatic made-up therapy under the sun. When I phoned them to discover who’d written them, I learned that the had been drafted by the Prince of Wales’ Foundation for Magic Medicine. And when I joked by asking if they had a competence for talking to trees, I was told, perfectly seriously, “You’d have to talk to LANTRA, the land-based organisation for that.”
That was in January 2008. A lot of correspondence with the head of Skills for Health got nowhere at all. She understood nothing and it hasn’t improved a jot.
This organisation costs a lot of taxpayers’ money and it should have been consigned to the "bonfire of the quangos" (but of course there was no such bonfire in reality). It is a disgrace.
The Quality Assurance Agency (QAA) is supposed to ensure the quality of university courses. In fact it endorses courses in nonsense alternative medicine and so does more harm than good. The worst recent failure of the QAA was in the case of the University of Wales: see Scandal of the University of Wales and the Quality Assurance Agency. The university was making money by validating thousands of external degrees in everything from fundamentalist theology to Chinese Medicine. These validations were revealed as utterly incompetent by bloggers, and later by BBC Wales journalist Ciaran Jenkins (now working for Channel 4).
The mainstream media eventually caught up with bloggers. In 2010, BBC1 TV (Wales) produced an excellent TV programme that exposed the enormous degree validation scam run by the University of Wales. The programme can be seen on YouTube (Part 1, and Part 2). The programme also exposed, incidentally, the uselessness of the Quality Assurance Agency (QAA) which did nothing until the scam was exposed by TV and blogs. Eventually the QAA sent nine people to Malaysia to investigate a dodgy college that had been revealed by the BBC. The trip cost £91,000. It could have been done for nothing if anyone at the QAA knew how to use Google.
The outcome was that the University of Wales stopped endorsing external courses, and it was soon shut down altogether (though bafflingly, its vice-chancellor, Marc Clement was promoted). The credit for this lies entirely with bloggers and the BBC. The QAA did nothing to help until the very last moment.
Throughout this saga Universities UK (UUK), has maintained its usual total passivity. They have done nothing whatsoever about their members who give BSc degrees in anti-scientific subjects. (UUK used to known as the Committee of Vice-Chancellors and Principals).
Council for Health Regulatory Excellence (CHRE), soon to become the PSAHSC,
Back now to the CHRE, the people who failed so signally to sort out the GCC. They are being reorganised. Their consultation document says
"The Health and Social Care Act 20122 confers a new function on the Professional Standards Authority for Health and Social Care (the renamed Council for Healthcare Regulatory Excellence). From November 2012 we will set standards for organisations that hold voluntary registers for people working in health and social care occupations and we will accredit the register if they meet those standards. It will then be known as an ‘Accredited Register’. "
They are trying to decide what the criteria should be for "accreditation" of a regulatory body. The list of those interested has some perfectly respectable organisations, like the British Psychological Society. It also contains a large number of crackpot organisations, like Crystal and Healing International, as well as joke regulators like the CNHC.
They already oversee the Health Professions Council (HPC) which is due to take over Herbal medicine and Traditional Chinese Medicine, with predictably disastrous consequences.
Two of the proposed criteria for "accreditation" appear to be directly contradictory.
Para 2.5 makes the whole accreditation pointless from the point of view of patients
2.5 It will not be an endorsement of the therapeutic validity or effectiveness of any particular discipline or treatment.
Since the only thing that matters to the patient is whether the therapy works (and is safe), accrediting of organisations that ignore this will merely give the appearance of official approval of crystal healing etc etc. This appears to contradict directly
A.7 The organisation can demonstrate that there either is a sound knowledge base underpinning the profession or it is developing one and makes that explicit to the public.
A "sound knowledge base", if it is to mean anything useful at all, means knowledge that the treatment is effective. If it doesn’t mean that, what does it mean?
It seems that the official mind has still not grasped the obvious fact that there can be no sensible regulation of subjects that are untrue nonsense. If it is nonsense, the only form of regulation that makes any sense is the law.
Please fill in the consultation. My completed return can be downloaded as an example, if you wish.
Medicines and Healthcare products Regulatory Agency (MHRA) should be a top level defender of truth. Its strapline is
"We enhance and safeguard the health of the public by ensuring that medicines and medical devices work and are acceptably safe."
The MHRA did something (they won’t tell me exactly what) about one of the most cruel scams that I’ve ever encountered, Esperanza Homeopathic Neuropeptide, peddled for multiple sclerosis, at an outrageous price ( £6,759 for 12 month’s supply). Needless to say there was not a jot of evidence that it worked (and it wasn’t actually homeopathic).
Astoundingly, Trading Standards officers refused to do anything about it.
The MHRA admit (when pushed really hard) that there is precious little evidence that any of the herbs work, and that homeopathy is nothing more than sugar pills. Their answer to that is to forget that bit about "ensuring that medicines … work"
Here’s the MHRA’s Traditional Herbal Registration Certificate for devils claw tablets.

The wording "based on traditional use only" has to be included because of European legislation. Shockingly, the MHRA have allowed them to relegate that to small print, with all the emphasis on the alleged indications. The pro-CAM agency NCCAM rates devil’s claw as "possibly effective" or "insufficient evidence" for all these indications, but that doesn’t matter because the MHRA requires no evidence whatsoever that the tablets do anything. They should, of course, added a statement to this effect to the label. They have failed in their duty to protect and inform the public by allowing this labelling.
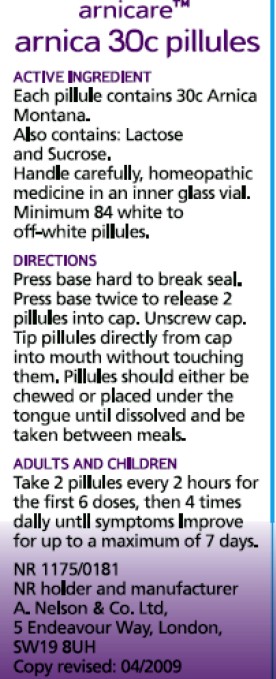
But it gets worse. Here is the MHRA’s homeopathic marketing authorisation for the homeopathic medicinal product Arnicare Arnica 30c pillules
It is nothing short of surreal.
|
|
Since the pills contain nothing at all, they don’t have the slightest effect on sprains, muscular aches or bruising. The wording on the label is exceedingly misleading.
If you "pregnant or breastfeeding" there is no need to waste you doctor’s time before swallowing a few sugar pills.
"Do not take a double dose to make up for a missed one". Since the pills contain nothing, it doesn’t matter a damn.
"If you overdose . . " it won’t have the slightest effect because there is nothing in them
And it gets worse. The MHRA-approved label specifies ACTIVE INGREDIENT. Each pillule contains 30c Arnica Montana
No, they contain no arnica whatsoever.
|
|
It truly boggles the mind that men with dark suits and lots of letters after their names have sat for hours only to produce dishonest and misleading labels like these.
When this mislabeling was first allowed, it was condemned by just about every scientific society, but the MHRA did nothing.
The Nightingale Collaboration.
This is an excellent organisation, set up by two very smart skeptics, Alan Henness and Maria MacLachlan. Visit their site regularly, sign up for their newsletter Help with their campaigns. Make a difference.
Conclusions
The regulation of alternative medicine in the UK is a farce. It is utterly ineffective in preventing deception of patients.
Such improvements as have occurred have resulted from the activity of bloggers, and sometime the mainstream media. All the official regulators have, to varying extents, made things worse.
The CHRE proposals promise to make matters still worse by offering "accreditation" to organisations that promote nonsensical quackery. None of the official regulators seem to be able to grasp the obvious fact that is impossible to have any sensible regulation of people who promote nonsensical untruths. One gets the impression that politicians are more concerned to protect the homeopathic (etc, etc) industry than they are to protect patients.
Deception by advocates of alternative medicine harms patients. There are adequate laws that make such deception illegal, but they are not being enforced. The CHRE and its successor should restrict themselves to real medicine. The money that they spend on pseudo-regulation of quacks should be transferred to the MHRA or a reformed Trading Standards organisation so they can afford to investigate and prosecute breaches of the law. That is the only form of regulation that makes sense.
Follow-up
The shocking case of the continuing sale of “homeopathic vaccines” for meningitis, rubella, pertussis etc was highlighted in an excellent TV programme by BBC South West. The failure of the MHRA and the GPC do take any effective action is a yet another illustration of the failure of regulators to do their job. I have to agree with Andy Lewis when he concludes
“Children will die. And the fault must lie with Professor Sir Kent Woods, chairman of the regulator.”
As promised in my last post about Edinburgh Napier University, I wrote to the vice-chancellor of the university, Professor Dame Joan K. Stringer DBE, BA (Hons) CertEd PhD CCMI FRSA FRSE, to invite her to respond.
|
7 February, 2011 Dear Professor Stringer, I should be grateful if you could let me know about your opinion of the degrees that you offer in Aromatherapy and Reflexology I have posted on my blog a bit of the material that was sent to me as result of recent FoI requests. See https://www.dcscience.net/?p=4049 I submit that degrees like this detract from the intellectual respectability of what is, not doubt, in other respects a good university, but since you are mentioned in the post, it’s only fair to give you the chance to defend yourself. In fact you’d be very welcome to do so publicly by commenting on the post. Best regards David Colquhoun |
Over a month later, I have received no response at all. This seems to me to be a bit discourteous.
There is nothing new in failing to get any answer to letters to vice-chancellors. The only VC who has ever thanked me for opening his eyes is Terence Kealey, of the University of Buckingham. All the rest have stayed silent. I can interpret this silence only as guilt. They know it’s nonsense, but dare not say so. Of course it isn’t infrequent for the course to close down after public exposure of the nonsense they teach. So perhaps the letters get read, even if they don’t elicit a reply.
Meanwhile the university sent me more materials that are used to teach their students. So here is another sample, largely from what’s taught to the unfortunate “reflexology” students.
Remember, these pre-scientific myths are not being taught as history or anthropology. They are taught as though they were true, to students who are then let loose on patients, so they can make money from anyone who is gullible enough to believe what they say.
There are no "excess body energies". It’s made-up nonsense.
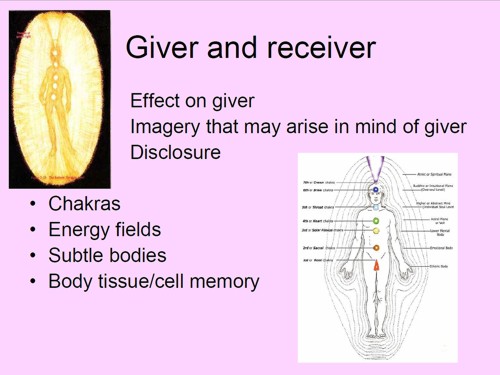
The diagram is pure imagination. It dates form a time before we knew anything about physiology, yet it is still being taught as though it meant something.
The admission that there is controversy is interesting. But it doesn’t seem to deter Napier’s teachers in the slightest.
How can anyone in the 21st century believe that the heart is "king of our emotional existence”?. That’s just preposterous pre-scientific myth,
You must be joking.
"Vibrational medicine" is a non-existent subject. Pure gobbledygook.
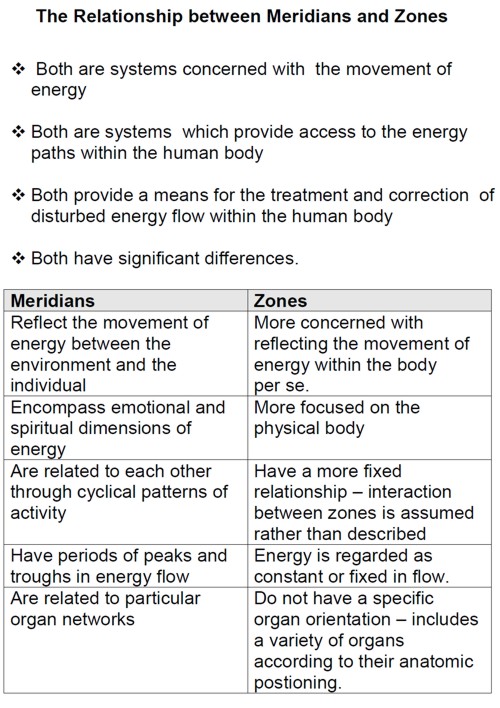
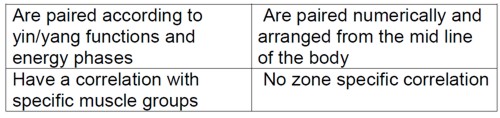
This is partly old, partly quite new. It is all preposterous made-up nonsense. There isn’t the slightest reason to think that "zones" or "meridians" exist. In fact there is good evidence from acupuncture studies to think that they don’t exist.
Now some slides from course CPT08102. The mention of the word ‘energy’ in the alternative world always rings alarm bells. Here’s why.
Well, it’s a good question. Pity about the answer.

Shouldn’t that read "as a practising reflexologist it is important than you have a MISunderstanding of the energy that surrounds us"?.

![]()
What logic? Have these people never heard of Hodgkin & Huxley (the answer, I imagine, is no)?
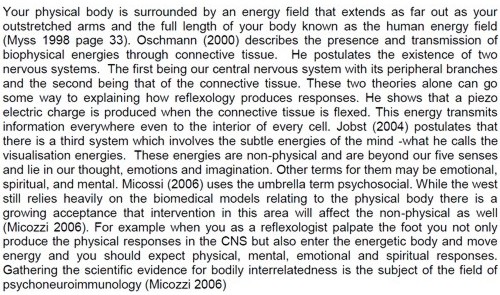
The mention of Kim Jobst immediately raises suspicions. He is a homeopath and endorser of the obviously fraudulent Q-link
pendant.
"when you as a reflexologist palpate the foot you not only produce the physical responses in the CNS but also enter the energetic body and move energy , , ". Well, no you don’t. This is purely made-up nonsense. The words sound "sciencey" but the meaning of the words is utterly obscure.
Yes we do live in an interconnected world. And sadly, that interconnectedness is used to spread myth and misinformation, usually with the aim of making money.
I guess Edinburgh Napier University makes money by teaching ancient myths as though they were true. In so doing they destroy their academic reputation.
Here you are tested to see how much nonsense you have memorised successfully. If only they had sent ‘model answers’.
Remember, these pre-scientific myths are not being taught as history or anthropology. They are taught as though they were true, to students who are then let loose on patients, so they can make money from anyone who is gullible enough to believe what they say.
A 2009 systematic review of randomised controlled trials concludes that “The best evidence available to date does not demonstrate convincingly that reflexology is an effective treatment for any medical condition.”. So forget it.
How about it Professor Stringer? Isn’t it time to clean up your university?
Follow-up
It seems very reasonable to suggest that taxpayers have an interest in knowing what is taught in universities. The recent Pittilo report suggested that degrees should be mandatory in Acupuncture, Herbal Medicine and Traditional Chinese Medicine. So it seems natural to ask to see what is actually taught in these degrees, so one can judge whether it protects the public or endangers them.
Since universities in the UK receive a great deal of public money, it’s easy. Just request the material under the Freedom of Information Act.
Well, uh, it isn’t as simple as that.
Every single application that I have made has been refused. After three years of trying, the Information Commissioner eventually supported my appeal to see teaching materials from the Homeopathy "BSc" at the University of Central Lancashire. He ruled that every single objection (apart from one trivial one) offered by the universities was invalid. In particular, it was ruled that univerities were not "commercial" organisations for the purposes of the Act.
So problem solved? Not a bit of it. I still haven’t seen any of the materials from the original request because the University of Central Lancashire appealed against the decision and the case of University of Central Lancashire v Information Commissioner is due to be heard on November 3rd, 4th and 5th in Manchester. I’m joined (as lawyers say) as a witness. Watch this space.
UCLan is not the exception. It is the rule. I have sought under the Freedom of Information Act, teaching materials from UClan (homeopathy), University of Salford (homeopathy, reflexology and nutritional therapy), University of Westminster (homeopathy, reflexology and nutritional therapy), University of West of England, University of Plymouth and University of East London, University of Wales (chiropractic and nutritional therapy), Robert Gordon University Aberdeen (homeopathy), Napier University Edinburgh (herbalism).
In every single case, the request for teaching materials has been refused. And that includes the last three, which were submitted after the decision of the Information Commissioner. They will send things like course validation documents, but these are utterly uninformative box-ticking documents. They say nothing whatsoever about what is actually taught.
The fact that I have been able to discover quite a lot about what’s being taught owes nothing whatsoever to the Freedom of Information Act. It is due entirely to the many honest individuals who have sent me teaching materials, often anonymously. We should be grateful to them. Their principles are rather more impressive than those of their principals.
Since this started about three years ago, two of the universities, UCLan and Salford, have shut down entry to all of their CAM courses. And Westminster has shut two of them, with more rumoured to be closing soon. They are to be congratulated for that, but is far from being the end of the matter. The Department of Health, and some of the Royal Colleges, have yet to catch up with the universities, The Pittolo report, which recommends making degrees compulsory, is being considered by the Department of Health. The consultation ends on November 2nd: if you haven’t yet responded, please do so now (see how here, and here).
A common excuse: the university does not possess teaching materials (yes, really)
Several of the universities claim that they cannot send teaching materials, because they have no access to them. This happens when the university has accredited a course that is run by another, privately run, institution. The place that does the actual teaching, being private, is exempt from the Freedom of Information Act.
The ludicrous corollary of this excuse is that the university has accredited the course without checking on what is taught, and in some cases without even having seen a timetable.
The University of Wales
In fact the University of Wales doesn’t run courses at all. Like the (near moribund) University of London, it acts as a degree-awarding authority for a lot of Welsh Universities. It also validates a lot of courses in non-university institutions, 34 or so of them in the UK, and others scattered round the world.
Many of them are theological colleges. It does seem a bit odd that St Petersburg Christian University, Russia, and International Baptist Theological Seminary, Prague, should be accredited by the University of Wales.
They also validate the International Academy of Osteopathy, Ghent (Belgium), Osteopathie Schule Deutschland, the Istituto Superiore Di Osteopatia, Milan, the Instituto Superior De Medicinas Tradicionales, Barcelona, the Skandinaviska Osteopathögskolan (SKOS) Gothenburg, Sweden and the College D’Etudes Osteopathiques, Canada.
The 34 UK institutions include the Scottish School of Herbal Medicine, the Northern College of Acupuncture and the Mctimoney College of Chiropractic.
The case of the Nutritional Therapy course has been described already in Another worthless validation: the University of Wales and nutritional therapy. It emerged that the course was run by a grade 1 new-age fantasist. It is worth recapitulating the follow up.
What does the University of Wales say? So far, nothing. Last week I sent brief and polite emails to Professor Palastanga and to
Professor Clement to try to discover whether it is true that the validation process had indeed missed the fact that the course organiser’s writings had been described as “preposterous, made-up, pseudoscientific nonsense” in the Guardian.
So far I have had no reply from the vice-chancellor, but on 26 October I did get an answer from Prof Palastanga.
As regards the two people you asked questions about – J.Young – I personally am not familiar with her book and nobody on the validation panel raised any concerns about it. As for P.Holford similarly there were no concerns expressed about him or his work. In both cases we would have considered their CV’s as presented in the documentation as part of the teaching team. In my experience of conducting degree validations at over 16 UK Universities this is the normal practice of a validation panel.
I have to say this reply confirms my worst fears. Validation committees such as this one simply don’t do their duty. They don’t show the curiosity that is needed to discover the facts about the things that they are meant to be judging. How could they not have looked at the book by the very person that they are validating? After all that has been written about Patrick Holford, it is simply mind-boggling that the committee seems to have been quite unaware of any of it.It is yet another example of the harm done to science by an unthinking, box-ticking approach.
Incidentally, Professor Nigel Palastanga has now been made Pro Vice-Chancellor (Quality) at the University of Wales and publishes bulletins on quality control. Well well.
The McTimoney College of Chiropractic was the subject of my next Freedom of Information request to the University of Wales. The reasons for that are, I guess, obvious. They sent me hundreds of pages of validation documents, Student Handbooks (approx 50 pages), BSc (Hons) Chiropractic Course Document. And so on. Reams of it. The documents mostly are in the range of 40 to 100 pages. Tons of paper, but none of it tells you anyhing whatsover of interest about what’s being taught. They are a testament to the ability of universities to produce endless vacuous prose with
very litlle content.
They did give me enough information to ask for a sample of the teaching materials on particular topics. But I gor blank refusal, on the grounds that they didn’t possess them. Only McTimoney had them. Their (unusually helpful) Freedom of Information officer replied thus.
“The University is entirely clear about the content of the course but the day to day timetabling of teaching sessions is a matter for the institution rather than the University and we do not require or possess timetable information. The Act does not oblige us to request the information but there is no reason you should not approach McTimoney directly on this.”
So the university doesn’t know the timetable. It doesn’t know what is taught in lectures, but it is " entirely clear about the content of the course".
This response can be described only as truly pathetic.
Either this is a laughably crude form of obstruction of my request, or perhaps, even more frighteningly, the university really believes that its endless box-ticking documents actually provide some useful control of quality. Perhaps the latter interpretation is more charitable. After all, the QAA, CHRE, UUK and every HR department share similar delusions about what constitutes quality.
Perhaps it is just yet another consequence of having science run largely by people who have never done it and don’t understand it.
Validation is a business. The University of Wales validates no fewer than 11,675 courses altogether. Many of these are perfectly ordinary courses in universities in Wales, but they validate 594 courses at non-Welsh accredited institutions, an activity that earned them £5,440,765 in the financial year 2007/8. There’s nothing wrong with that if they did the job properly. In the two cases I’ve looked at, they haven’t done the job properly. They have ticked boxes but they have not looked at what’s being taught or who is teaching it.
The University of Kingston
The University of Kingston offers a “BSc (Hons)” in acupuncture. In view of the fact that the Pittilo group has recommended degrees in acupuncture, there is enormous public interest in what is taught in such degrees, so I asked.
They sent the usual boring validation documents and a couple of sample exam papers . The questions were very clinical, and quite beyond the training of acupuncturists. The validation was done by a panel of three, Dr Larry Roberts (Chair, Director of Academic Development, Kingston University), Mr Roger Hill (Accreditation Officer, British Acupuncture Accreditation Board) and Ms Celia Tudor-Evans (Acupuncturist, College of Traditional Acupuncture, Leamington Spa). So nobody with any scientific expertise, and not a word of criticism.
|
Further to your recent request for information I am writing to advise that the University does not hold the following requested information: (1) Lecture handouts/notes and powerpoint presentations for the following sessions, mentioned in Template 3rd year weekend and weekday course v26Aug2009_LRE1.pdf (a) Skills 17: Representational systems + Colour & Sound ex. Tongue feedback 11 (b) Mental Disease + Epilepsy Pulse feedback 21 (c) 18 Auricular Acupuncture (d) Intro. to Guasha + practice Cupping, moxa practice Tongue feedback 14 (2) I cannot see where the students are taught about research methods and statistics. I would like to see Lecture handouts/notes and PowerPoint presentations for teaching in this area, but the ‘timetables’ that you sent don’t make clear when or if it is taught. The BSc Acupuncture is delivered by a partner college, the College of Integrated Chinese Medicine (CICM), with Kingston University providing validation only. As such, the University does not hold copies of the teaching materials used on this course. In order to obtain copies of the teaching materials required you may wish to contact the College of Integrated Chinese Medicine directly. This completes the University’s response to your information request. |
So again we see that Kingston has validated the course but has not seen a timetable, far less what is taught. My reply was thus
|
Yes I am exceedingly unhappy about it. The university attaches its name to the course so it must obviously be able to get the material simply by asking for it (I’m surprised that the university should endorse a course without knowing what is taught on it, but that’s another matter). I request formally that you obtain this material. If necessary please read this as a formal appeal. |
I await with interest. In every single case so far, the internal review has merely confirmed the initial refusal. It means a bit of a delay before the case goes to the Information Commisssioner’s Office.
Napier University Edinburgh
Napier University runs a "BSc (Hons) Herbal medicine". (brochure here). Since herbal medicine is a subject of the Pittilo recommendations, there is enormous public interest in what they teach. So I asked, under the Freedom of Information (Scotland) Act (2002). They sent quite quickly validation and accreditation documents, some examination papers, timetables and lecture lists.
The validation was the usual vacuous box-ticking stuff though it did reveal that the course “made extensive use of techniques such as tongue and pulse diagnosis”, which are well known phoney diagnosis methods, about as much use as a pendulum (as used at Westminster University).
As at Kingston University, the exam papers they chose to send were mostly "pretend doctor" stuff. One of them was
Discuss the herbal practitioner’s role in the management of IHD [ischaemic heart disease)
How one would like to see what the students said, and, even more one would like to see the model answer. Amateurs who try to treat potentially serious conditions are a danger to the public.
So then we got to the interesting bit, the request for actual teaching materials.
|
I have looked at the material that you sent and I’d now like to make the following supplementary request (A) Lecture notes/handouts and powerpoint slides for the following small smaple of lectures HRB09102 Materia Medica 4 Materia Medica 3 HRB08103 Clinical Medicine and Diagnosis 4 (HRB09104) HRB09100 Materia Medica & Herbal Practice BSc Herbal Medicine : Materia Medica HRB07102 Lastly, I can see nowhere in the timetable, lectures that deal with Research methods, clinical trial design and statistics. |
No prizes for guessing the result Total refusal to send any of them. To make matters worse, the main grounds for refusal were the very "commercial interests" which, after careful legal examination, the Information Commissioner (for England and Wales) had decided were invalid. They say too that "The public interest in withholding the information is greater than the public interest in its release".. It is hard to see how the public interest is served by concealing from the people who pay for the degrees what is taught on degrees that Pittilo wants to make compulsory. [Download the whole response]
The matter is now under internal appeal (read the appeal) and eventually we shall find out whether the Scottish Information Commissioner backs the judgement.
Robert Gordon University Aberdeen
This case has particular interest because the Vice-Chancellor of Robert Gordon University is Professor Michael Pittilo, chair of the highly contentious steering group that recommended degress in CAM. Robert Gordon University (RGU) does not teach herbal medicine or acupuncture. But they do run An Introduction to Homeopathy. All the degrees in homeopathy have closed. It is perhaps the daftest and most discredited of all the popular forms of Magic Medicine. But Professor Pittilo thinks it is an appropriate subject to teach in his university.
So again I asked for information under the Freedom of Information (Scotland) Act 2002. They sent me quite quckly a list of the powerpoint presentations used on the courses [download it]. I asked for a small sample of the powerpoints. And again the university did not possess them!
|
I should like to see only the following three powerpoint presentations in the first instance, please.
Please can you let me know also who produced the powerpoints. (1) Evidence for homeopathy I note that you will have to request them but since they are being offered as part of a course offered by RGU, so RGU is responsible for their quality, I presume that this should cause no problem. |
The request was refused on much the same grounds as used by Napier University. As usual, the internal review just confirmed the initial proposal (but dropped the obviously ludicrous public interest defence). The internal review said
“it is mainly the quality of our courses (including course material) and teaching which has given us the position of "the best modern university in Scotland"
I am bound to ask, if the university is so proud of its course material, why is it expending so much time and money to prevent anyone from seeing a small sample of it?
My appeal has been sent to the Scottish Information Commissioner [download the appeal].
What are vice-chancellors thinking about?
I find it very difficult to imagine what is going through the heads of vice-chancellors who run courses in mumbo-jumbo. Most of them don’t believe a word of it (though Michael Pittilo might be an exception) yet they foist it on their students. How do they sleep at night?
Recently the excellent Joe Collier wrote a nice BMJ blog which applauded the lack of respect for authority in today’s students, Joe Collier says good riddance to old-fashioned respect. I couldn’t resist leaving a comment.
|
I couldn’t agree more. There is nothing quite so unnerving as being addressed as “Sir”. It is an advantage of age that you realise what second-rate people come to occupy very grand positions. Still odder since, if occasionally they are removed for incompetence, they usually move to an even grander position. I guess that when I was an undergraduate, I found vice-chancellors somewhat imposing. That is, by and large, not a view that survives closer acquaintance. |
Should teaching materials be open to the public?
There is only one university in the world that has, as a matter of policy, made all of its teaching material open to the public, that is the Massachusetts Institute of Technology (MIT). I can recommend strongly course 18.06, a wonderful set of lectures on Linear Algebra by Gilbert Strang. (It is also a wonderful demonstration of why blackboards may be better than Powerpoint for subjects like this). Now they are on YouTube too.
A lot of other places have made small moves in the same direction, as discussed recently in Times Higher Education, Get it Out in the Open.
Now the OU is working with other British universities to help them develop and share open course materials. In June, at the celebrations for the 40th anniversary of the OU, Gordon Brown announced funding to establish the Support Centre for Open Resources in Education at the OU, as part of a £7.8 million grant designed to enhance the university’s national role.
The funding follows a separate grant of £5.7 million from the Higher Education Funding Council for England for universities across the sector to make thousands of hours of free learning materials available.
Much material is available on the web, when individual teachers choose to place it there, but at the same time there is a move in the other direction. In particular, the widespread adoption of Moodle has resulted in a big decrease in openness. Usually you have to be registered on a course to see the material. Even other people in the university can’t see it. I think that is a deplorable development (so, presumably, does HEFCE).
Conclusion
I was told by the Univerity of Kingston that
“The course is one which the University has validated and continues to be subject to the University’s quality assurance procedures, such as internal subject reviews, annual monitoring and external examining”
The only conclusion to be drawn from this is that “quality arrurance procedures” work about as well in universities as they did in the case of baby Peter. No doubt they were introduced with worthy aims. But in practice they occupy vast amounts of time for armies of bureaucrats, and because the brain does not need to be engaged they end up endorsing utter nonsenes. The system is broken.
Resistance is futile. You can see a lot of the stuff here
It is hard to keep secrets in the internet age. Thanks to many wonderful people who have sent me material. you can see plenty of what is taught, despite the desperate attempts of vice-chancellors to conceal it. Try these links.
What is actually taught
Chinese medicine -acupuncture gobbledygook revealed
https://www.dcscience.net/?p=1950
Consultation opens on the Pittilo report: help top stop the Department of Health making a fool of itself
https://www.dcscience.net/?p=2007
Why degrees in Chinese medicine are a danger to patients
https://www.dcscience.net/?p=2043
More make-believe from the University of Westminster. This time its Naturopathy
https://www.dcscience.net/?p=1812
The last BSc (Hons) Homeopathy closes! But look at what they still teach at Westminster University.
https://www.dcscience.net/?p=1329
The opposite of science
https://www.dcscience.net/?p=1191
Bad medicine. Barts sinks further into the endarkenment.
https://www.dcscience.net/?p=1143
A letter to the Times, and progress at Westminster
https://www.dcscience.net/?p=984
Nutritional Fairy Tales from Thames Valley University
https://www.dcscience.net/?p=260
Westminster University BSc: amethysts emit high yin energy
https://www.dcscience.net/?p=227
References for Pittilo report consultation
A very bad report: gamma minus for the vice-chancellor
https://www.dcscience.net/?p=235
The Times (blame subeditor for the horrid title)
http://www.timesonline.co.uk/tol/comment/columnists/guest_contributors/article4628938.ece
Some follow up on the Times piece
https://www.dcscience.net/?p=251
The Health Professions Council breaks its own rules: the result is nonsense
https://www.dcscience.net/?p=1284
One month to stop the Department of Health endorsing quackery. The Pittilo questionnaire,
https://www.dcscience.net/?p=2310
An excellent submission to the consultation on statutory regulation of alternative medicine (Pittilo report)
https://www.dcscience.net/?p=2329
Follow-up
Two weeks left to stop the Department of Health making a fool of itself. Email your response to tne Pittilo consultation to this email address HRDListening@dh.gsi.gov.uk
I’ve had permission to post a submission that has been sent to the Pittilo consultation. The whole document can be downloaded here. I have removed the name of the author. It is written by the person who has made some excellent contributions to this blog under the pseudonym "Allo V Psycho".
The document is a model of clarity, and it ends with constructive suggestions for forms of regulation that will, unlike the Pittilo proposals, really protect patients
Here is the summary. The full document explains each point in detail.
|
Executive Summary
Instead, safe regulation of alternative practitioners should be through:
|
The first two recommendations for effective regulation are much the same as mine, but the the third one is interesting. The problem with the Cancer Act (1939), and with the Unfair Trading regulations, is that they are applied very erratically. They are the responsibility of local Trading Standards offices, who have, as a rule, neither the expertise nor the time to enforce them effectively. A Health Advertising Standards Authority could perhaps take over the role of enforcing existing laws. But it should be an authority with teeth. It should have the ability to prosecute. The existing Advertising Standards Authority produces, on the whole, excellent judgements but it is quite ineffective because it can do very little.
A letter from an acupuncturist
I had a remarkable letter recently from someone who actually practises acupuncture. Here are some extracts.
|
“I very much enjoy reading your Improbable Science blog. It’s great to see good old-fashioned logic being applied incisively to the murk and spin that passes for government “thinking” these days.” “It’s interesting that the British Acupuncture Council are in favour of statutory regulation. The reason is, as you have pointed out, that this will confer a respectability on them, and will be used as a lever to try to get NHS funding for acupuncture. Indeed, the BAcC’s mission statement includes a line “To contribute to the development of healthcare policy both now and in the future”, which is a huge joke when they clearly haven’t got the remotest idea about the issues involved.” “Before anything is decided on statutory regulation, the British Acupuncture Council is trying to get a Royal Charter. If this is achieved, it will be seen as a significant boost to their respectability and, by implication, the validity of state-funded acupuncture. The argument will be that if Physios and O.T.s are Chartered and safe to work in the NHS, then why should Chartered Acupuncturists be treated differently? A postal vote of 2,700 BAcC members is under-way now and they are being urged to vote “yes”. The fact that the Privy Council are even considering it, is surprising when the BAcC does not even meet the requirement that the institution should have a minimum of 5000 members (http://www.privy-council.org.uk/output/Page45.asp). Chartered status is seen as a significant stepping-stone in strengthening their negotiating hand in the run-up to statutory regulation.” “Whatever the efficacy of acupuncture, I would hate to see scarce NHS resources spent on well-meaning, but frequently gormless acupuncturists when there’s no money for the increasing costs of medical technology or proven life-saving pharmaceuticals.” “The fact that universities are handing out a science degree in acupuncture is a testament to how devalued tertiary education has become since my day. An acupuncture degree cannot be called “scientific” in any normal sense of the term. The truth is that most acupuncturists have a poor understanding of the form of TCM taught in P.R.China, and hang on to a confused grasp of oriental concepts mixed in with a bit of New Age philosophy and trendy nutritional/life-coach advice that you see trotted out by journalists in the women’s weeklies. This casual eclectic approach is accompanied by a complete lack of intellectual rigour. My view is that acupuncturists might help people who have not been helped by NHS interventions, but, in my experience, it has very little to do with the application of a proven set of clinical principles (alternative or otherwise). Some patients experience remission of symptoms and I’m sure that is, in part, bound up with the psychosomatic effects of good listening, and non-judgemental kindness. In that respect, the woolly-minded thinking of most traditional acupuncturists doesn’t really matter, they’re relatively harmless and well-meaning, a bit like hair-dressers. But just because you trust your hairdresser, it doesn’t mean hairdressers deserve the Privy Council’s Royal Charter or that they need to be regulated by the government because their clients are somehow supposedly “vulnerable”.” |
Earlier postings on the Pittilo recommendations
A very bad report: gamma minus for the vice-chancellor https://www.dcscience.net/?p=235
Article in The Times (blame subeditor for the horrid title)
http://www.timesonline.co.uk/tol/comment/columnists/guest_contributors/article4628938.ece
Some follow up on The Times piece
https://www.dcscience.net/?p=251
The Health Professions Council breaks its own rules: the result is nonsense
https://www.dcscience.net/?p=1284
Chinese medicine -acupuncture gobbledygook revealed
https://www.dcscience.net/?p=1950
Consultation opens on the Pittilo report: help top stop the Department of Health making a fool of itself https://www.dcscience.net/?p=2007
Why degrees in Chinese medicine are a danger to patients https://www.dcscience.net/?p=2043
One month to stop the Department of Health endorsing quackery. The Pittilo questionnaire, https://www.dcscience.net/?p=2310
Follow-up
This post has been translated into Belorussian..
Chinese medicine and herbal medicine are in the news at the moment. There is a real risk that the government could endorse them by accepting the Pittilo report.
In my view traditional Chinese medicine endangers people. The proposed ‘regulation’ would do nothing to protect the public. Quite on the contrary, it would add to the dangers, by giving an official stamp of approval while doing nothing for safety.
The government’s idea of improving safety is to make sure that practitioners are ‘properly trained’. But it is the qualifications that cause the danger in the first place. The courses teach ideas that are plain wrong and often really dangerous.
Why have government (and some universities) not noticed this? That’s easy to see. Governments, quangos and university validation committees simply don’t look. They tick boxes but never ask what actually goes on. Here’s some examples of what goes on for them to think about. They show clearly the sort of dangerous rubbish that is taught on some of these ‘degrees’.
These particular slides are from the University of Westminster, but similar courses exist in only too many other places. Watch this space for more details on courses at Edinburgh Napier University, Middlesex University and the University of East London
Just a lot of old myths. Sheer gobbledygook,
SO much for a couple of centuries of physiology,
It gets worse.
Plain wrong.
Curious indeed. The fantasy gobbledygook gets worse.
Now it is getting utterly silly. Teaching students that the brain is made of marrow is not just absurd, but desperately dangerous for anyone unlucky (or stupid) enough to go to such a person when they are ill.
Here’s another herbal lecture., and this time the topic is serious. Cancer.
Herbal approaches for patients with cancer.
I’ve removed the name of the teacher to spare her the acute embarrassment of having these dangerous fantasies revealed. The fact that she probably believes them is not a sufficient excuse for endangering the public. There is certainly no excuse for the university allowing this stuff to be taught as part of a BSc (Hons).
First get them scared with some bad statistics.
No fuss there about distinguishing incidence, age-standardisation and death rates. And no reference. Perhaps a reference to the simple explanation of statistics at Cancer Research UK might help? Perhaps this slide would have been better (from CDC). Seems there is some mistake in slide 2.
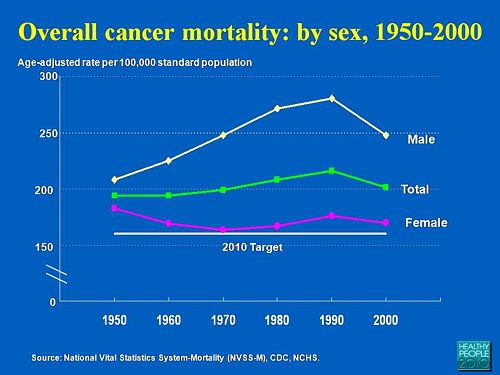
Straight on to a truly disgraceful statement in slide 3
The is outrageous and very possibly illegal under the Cancer Act (1939). It certainly poses a huge danger to patients. It is a direct incentive to make illegal, and untrue claims by using weasel words in an attempt to stay just on the right side of the law. But that, of course, is standard practice in alternative medicine,
Slide 11 is mostly meaningless. “Strengthen vitality” sounds good but means nothing. And “enhancing the immune system” is what alternative medicine folks always say when they can think of nothing else. Its meaning is ill-defined and there is no reason to think that any herbs do it.
The idea of a ‘tonic’ was actually quite common in real medicine in the 1950s. The term slowly vanished as it was realised that it was a figment of the imagination. In the fantasy world of alternative medicine, it lives on.
Detoxification, a marketing term not a medical one, has been extensively debunked quite recently. The use of the word by The Prince of Wales’ company, Duchy Originals recently fell foul of the Advertising Standards Authority, and his herbal ‘remedies’ were zapped by the MHRA (Medicines and Health Regulatory Authority).
And of course the antioxidant myth is a long-disproved hypothesis that has become a mere marketing term.
“Inhibits the recurrence of cancer”! That sounds terrific. But if it is so good why is it not even mentioned in the two main resources for information about herbs?
In the UK we have the National Library for Health Complementary and Alternative Medicine Specialist Library (NeLCAM), now a part of NHS Evidence. It was launched in 2006. The clinical lead was none other than Peter Fisher, clinical director of the Royal London Homeopathic Hospital, and the Queen’s homeopathic physician. The library was developed with the School of Integrated Health at the University of Westminster (where this particular slide was shown to undergraduates). Nobody could accuse these people of being hostile to magic medicine,
It seems odd, then, that NeLCAM does not seem to thnk to think that Centella asiatica, is even worth mentioning.
In the USA we have the National Center for Alternative and Complementary Medicine (NCCAM), an organisation that is so friendly to alternative medicine that it has spent a billion dollars on research in the area, though it has produced not a single good treatment for that vast expenditure. But NCCAM too does not even mention Centella asiatica in its herb list. It does get a mention in Cochrane reviews but only as a cosmetic cream and as an unproven treatment for poor venous circulation in the legs.
What on earth is a “lymph remedy”. Just another marketing term?
“especially valuable in the treatment of breast, throat and uterus cancer.“
That is a very dramatic claim. It as as though the hapless students were being tutored in doublespeak. What is meant by “especially valuable in the treatment of”? Clearly a desperate patient would interpret those words as meaning that there was at least a chance of a cure. That would be a wicked deception because there isn’t the slightest reason to think it works. Once again there this wondrous cure is not even mentioned in either NELCAM or NCCAM. Phytolacca is mentioned, as Pokeweed, in Wikipedia but no claims are mentioned even there. And it isn’t mentioned in Cochrane reviews either. The dramatic claims are utterly unfounded.
Ah the mistletoe story, again.
NHS Evidence (NeLCAM) lists three completed assessments. One concludes that more research is needed. Another concludes that “Rigorous trials of mistletoe extracts fail to demonstrate efficacy of this therapy”, and the third says “The evidence from RCTs to support the view that the application of mistletoe extracts has impact on survival or leads to an improved ability to fight cancer or to withstand anticancer treatments is weak”.
NCCAM says of mistletoe
- More than 30 human studies using mistletoe to treat cancer have been done since the early 1960s, but major weaknesses in many of these have raised doubts about their findings (see Question 6).
- Very few bad side effects have been reported from the use of mistletoe extract, though mistletoe plants and berries are poisonous to humans (see Question 7).
- The U.S. Food and Drug Administration (FDA) has not approved mistletoe as a treatment for cancer or any other medical condition (see Question 8).
- The FDA does not allow injectable mistletoe to be imported, sold, or used except for clinical research (see Question 8).
Cochrane reviews lists several reviews of mistletoe with similar conclusions. For example “The evidence from RCTs to support the view that the application of mistletoe extracts has impact on survival or leads to an improved ability to fight cancer or to withstand anticancer treatments is weak”.
Anthroposophy is one of the highest grades of fantasy you can find. A post on that topic is in the works.
“Indicated for cancers . . . colon/rectal, uterine, breast, lung“. A cure for lung cancer? That, of course, depends on how you interpret the weasel words “indicated for”. Even Wikipedia makes no mention of any claims that Thuja benefits cancer. NHS Evidence (NeLCAM) doesn’t mention Thuja for any indication. Neither does NCCAM. Nor Cochrane reviews. That is not the impression the hapless students of this BSc lecture were given. In my view suggestions that you can cure lung cancer with this tree are just plain wicked.
Pure snake oil, and not even spelled correctly, Harry Hoxsey’s treatment centres in the USA were closed by court order in the 1950s.
At least this time it is stated that there is no hard evidence to support this brand of snake oil.
More unfounded claims when it says “treated successfully many cancer patients”. No references and no data to support the claim. It is utterly unfounded and claims to the contrary endanger the public.
Gerson therapy is one of the most notorious and unpleasant of the quack cancer treatments. The Gerson Institute is on San Diego, but their clinics are in Mexico and Hungary. It is illegal in the USA. According to the American Cancer Society you get “a strict low-salt, low-fat, vegetarian diet and drinking juice from about twenty pounds of fresh fruits and vegetables each day. One glass of juice is consumed each hour, thirteen times a day. In addition, patients are given several coffee enemas each day. Various supplements, such as potassium, vitamin B12, pancreatic enzymes, thyroid hormone, and liver extracts, are used to stimulate organ function, particularly of the liver and thyroid.”. At one time you also got several glasses of raw calf liver every day but after infections killed several people] carrot juice was given instead.
Cancer Research UK says “there is no evidence to show that Gerson therapy works as a cure for cancer”, and “The Gerson diet can cause some very serious side effects.” Nobody (except perhaps the Price of Wales) has any belief in this unpleasant, toxic and expensive folk-lore.
Again patients are endangered by teaching this sort of stuff.
And finally, the usual swipe at vaccines. It’s nothing to do with herbalism. but just about every alternative medicine advocate seems to subscribe to the anti-vaccination lobby.. It is almost as though they have an active preference for things that are known to be wrong. They seem to believe that medicine and science are part of an enormous conspiracy to kill everyone.
Perhaps this dangerous propaganda might have been ameliorated if the students had been shown this slide (from a talk by Melinda Wharton).
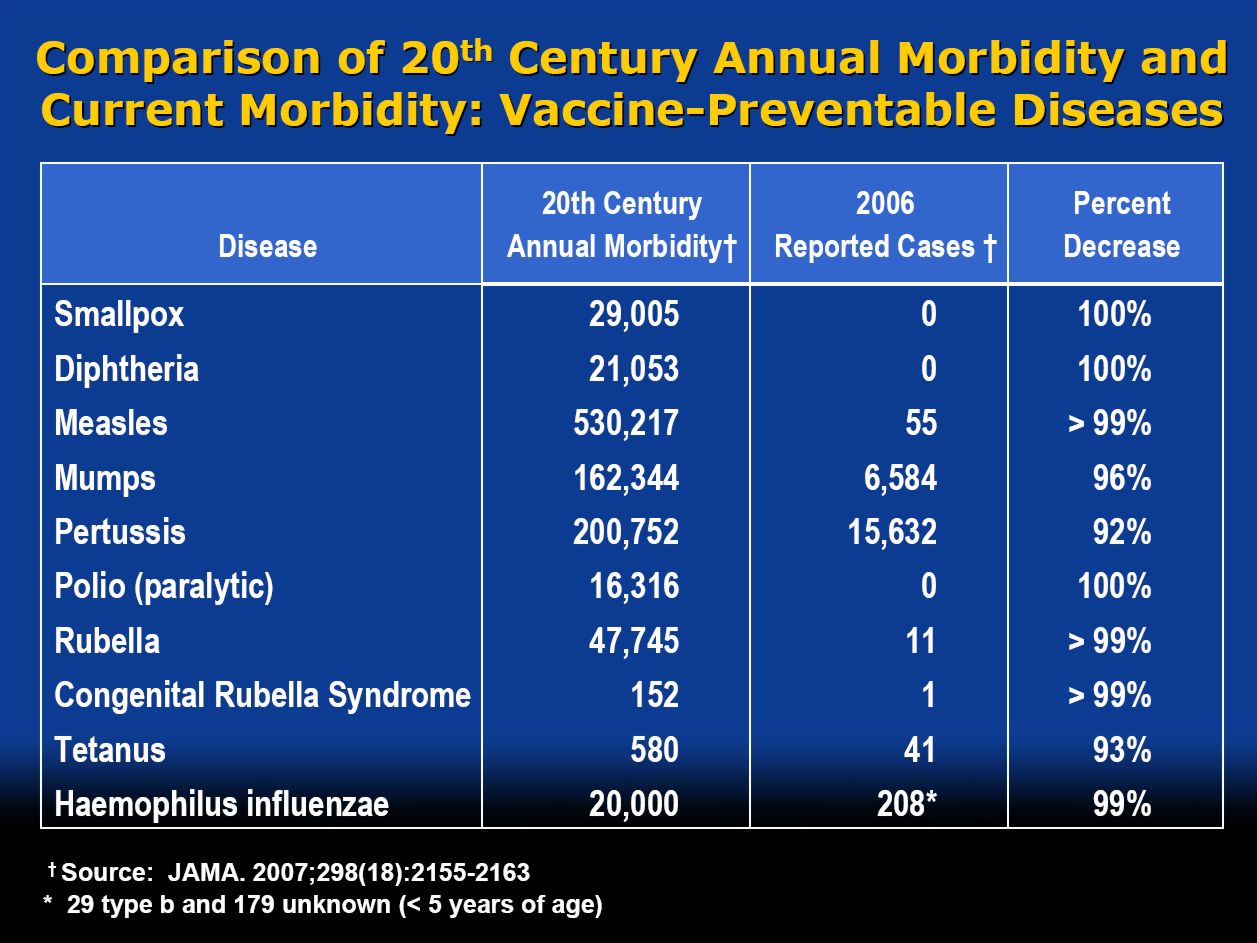
Click to enlarge
Left to people like this, we would still have smallpox, diphtheria. tetanus and rabies, Take a look at Vaccine-preventable diseases.
This is the sort of ‘education’ which the Pittilo report wants to make compulsory.
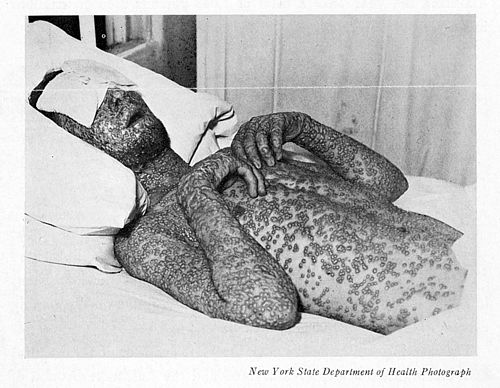
Smallpox in Baltimore, USA, 1939. This man was not vaccinated.
Conclusion
This selection of slides shows that much of the stuff taught in degrees in herbal medicine poses a real danger to public safety and to public health.
Pittilo’s idea that imposing this sort of miseducation will help safety is obviously and dangerously wrong. The Department of Health must reject the Pittilo recommendations on those grounds.
Follow-up
The much-delayed public consultation on the Pittilo report has just opened.
It is very important that as many people as possible respond to it. It’s easy to say that the consultation is sham. It will be if it is left only to acupuncturists and Chinese medicine people to respond to it. Please write to them before the closing date, November 2nd 2009. The way to send your evidence is here.
There is a questionnaire that you can complete, with the usual leading questions. Best do it anyway, but I’d suggest also sending written evidence as attachment too. I just got from DoH the email address where you can send it. They said
| if you have material you wish to send which you can’t easily “shoehorn” into the questionnaire, please send it to the following mailbox:
HRDListening@dh.gsi.gov.uk |
Here are three documents that I propose to submit in response to the consultation.I ‘d welcome criticisms that might make it more convincing. Use any parts of them you want in your own response.
- Submission to the Department of Health, for the consultation on the Pittilo report [download pdf].
- What is taught in degrees in herbal and traditional Chinese medicine? [download pdf]
- $2.5B Spent, No Alternative Med Cures [download pdf]
|
I’ve written quite a lot about the Pittilo report already, in particular A very bad report: gamma minus for the vice-chancellor, and in The Times (see also the blog version).
Intriguingly, these posts are at number 2 in a Google search for “Michael Pittilo”. |
 |
Briefly, the back story is this.
It is now over a year since the Report to Ministers from “The Department of Health Steering Group on the Statutory Regulation of Practitioners of Acupuncture, Herbal Medicine, Traditional Chinese Medicine and Other Traditional Medicine Systems Practised in the UK” [download the report].
The chair of the steering group was Professor R. Michael Pittilo, Principal and Vice-Chancellor of The Robert Gordon University, Aberdeen. The reason thet the report is so disastrously bad in its assessment of evidence is that it was written entirely by people with vested interests.
The committee consisted of five acupuncturists, five herbalists and five representatives of traditional Chinese medicine (plus eleven observers). There was not a single scientist or statistician to help in the assessment of evidence. And it shows: The assessment of the evidence in the report was execrable. Every one of the committee members would have found themselves out of work if they had come to any conclusion other than that their treatment works, Disgracefully, these interests were not declared in the report, though they are not hard to find. The university of which the chair is vice-chancellor runs a course in homeopathy, the most discredited of the popular forms of alternative medicine. That tells you all you need to know about the critical faculties of Michael Pittilo.
The two main recommendations of this Pittilo report are that
- Practitioners of Acupuncture, Herbal Medicine, Traditional Chinese Medicine should be subject to statutory regulation by the Health Professions Council
- Entry to the register normally be through a Bachelor degree with Honours
Let’s consider the virtue of these two recommendations.
Regulation by the Health Professions Council (HPC) breaks their own rules
For a start, this should be ruled out by the HPC’s own rules, which require “Practise based on evidence of efficacy” as a condition for registration. Since there is practically no “evidence of efficacy”, it follows that the HPC can’t regulate acupuncture, herbal and Chinese medicine as Pittilo recommends. Or so you’d think. But the official mind seems to have an infinite capacity for doublespeak. The HPC published a report on 11 September 2008, Regulation of Medical Herbalists, Acupuncturists and Traditional Chinese Medicine Practitioners.
The report says
1. Medical herbalists, acupuncturists and traditional Chinese medicine practitioners should be statutorily regulated in the public interest and for public safety reasons.
2. The Health Professions Council is appropriate as the regulator for these professions.
3. The accepted evidence of efficacy overall for these professions is limited, but regulation should proceed because it is in the public interest.
In other words, the HPC simply decided to ignore its own rules, Its excuse for doing so is that regulation would protect “public safety” . But it simply would not do that. It is ell known that some Chinese herbs are adulterated with dangerous substances, but laws against that already exist. Trading Standards are much more likely to take appropriate action than the HPC. The Medicines and Health Regulatory Authority (MHRA) already deals with the licensing of herbal medicines. and, despite the fact that it recently betrayed its trust by allowing them to be labelled in a misleading way, they are the people to do it, not the HPC.
The Pittilo report (page 11) says
In future, it is hoped that more Government funding can be allocated to research into traditional/herbal medicines and acupuncture and that grants will become available to encourage practitioners to undertake postgraduate research work.
So they are asking for more government money.
In March 2007, the Chinese Government pledged to spend over $130 million over the next five years on research into the effectiveness of traditional Chinese medicine. It is to be hoped that this money will be targeted effectively to evaluate TCM.
It seems to have escaped the notice of Pittilo that roughly 100 percent of trials of Chinese medicine done in China come out positive. Elsewhere, very few come out positive,(see Vickers et al., 1998, Controlled Clinical Trials, 19, 159-166: download reprint) The Department of Health would be unwise to rely on Chinese research. Remember that modern acupuncture was not so much a product of ancient wisdom, but rather it stems from nationalist propaganda by Mao Tse-Tung, who needed a cheap way to keep the peasants quiet, though he was too sensible to use it himself.
The HPC report (page 5) cites these with the words
” . . . a lack of evidence of efficacy should not prevent regulation but that the professions should be encouraged and funded to strengthen the evidence base.”
This sentence seems to assume that the outcomes of research will be to strengthen the evidence base. Thus far, precisely the opposite has been the case. The Pittilo group has apparently not noticed that the US National Institutes of Health has already spent a billion dollars on research in alternative medicine and failed to come up with a single effective treatment. There are better ways to spend money on health. See, for example $2.5B Spent, No Alternative Med Cures found. .An enornous amount of research has already been done and the outcomes have produced no good treatments,
The proposed regulation would endanger the public, not protect it.
The excuse given by the HPC for breaking its own rules is that it should do so to protect the public.
Likewise Ann Keen, Health Minister, said:
“Patient safety is paramount, whether people are accessing orthodox health service treatments or using alternative treatments”
So first we need to identify what dangers are posed by acupuncture, herbal medicine and traditional Chinese medicine.
- Acupuncture is fairly safe. Its biggest danger lies in the unjustified claims that are routinely made for what can be achieved by being impaled by needles. This poses a danger that people may use acupuncture in place of treatments that work
- Herbal medicines are unstandardised, so even the very few that may work are dangerous to patients because the dose of active principle is unknown and varies from one batch to another. Taking a herbal medicine is a bit like swallowing a random number of tablets, False health claims pose a danger to patients too, when they cause patients to avoid treatments that work.
- Traditional Chinese Medicine is probably the most dangerous. Like the other two, the medicines are unstandardised so the dose is never known. False health claims abound. And in addition to these dangers, many cases have been found of Chinese medicines being adulterated with poisonous substances or with conventional drugs.
The form of regulation proposed by Pittilo would do little or nothing to protect the public from any of these dangers.
The proposals accept the herbal and Chinese medicine as traditionally practised. Nothing would be done about one of the major dangers, the lack of standardisation. That is a problem that was solved by pharmacologists in the 1930s, when international standards were set for the biological activity of things like tincture of digitalis, and assays were devised so that different batches could be adjusted to the same potency. Now, 80 years later, it is being proposed by Pittilo that we should return to the standards of safety that existed at the beginning of the last century. That is a threat to public safety., but the proposed regulation would do nothing whatsoever to protect the public from this dangerous practice. On the contrary, it would give official government sanction to it.
The other major danger is that patients are deceived by false health claims. This is dangerous (as well as dishonest) because it can cause patients to avoid treatments that work better, The internet abounds with claims that herbs can cure anything from diabetes to cancer. Many are doubtless illegal, but regulators like the HPC have traditionally ignored such claims: they are left to Trading Standards, Advertising Standards and the Medicines and Health Regulatory Authority (MHRA) to deal with. The MHRA already also has responsibility for monitoring side effects. The HPC would not do this.
The analogy with chiropractic and the GCC
The foolishness of allowing statutory regulation for unproven treatments has recently been illustrated quite dramatically by the case of chiropractic. Chiropractors have had statutory regulation by the General Chiropractic Council, which was established by the Chiropractors Act of 1994. The British Chiropractic Association (BCA) recently decided to sue the science writer, Simon Singh, for defamation when he cast doubt on some of the claims made by chiropractors, in particular their claims to be able to cure colic and asthma in children. That led to close examination of the claims. In fact there is no reason to think that spinal manipulation works for asthma, or that it works for colic. In fact there is quite good evidence that the claims are false. The result was that about 600 well-justified complaints have been lodged with the GCC (enough to bankrupt the GCC if the complaints are dealt with properly).
The point of this story is that the statutory regulator had nothing whatsoever to prevent these false health claims being made. Two of the complaints concern practices run by the chair of the GCC. Worse, the GCC actually endorsed such claims. The statutory regulator saw its duty to defend chiropractic (apart from a handful of cases of sexual misdemeanours), not to protect the patient from false health claims. The respectability conferred by statutory regulation made false health claims easier and endangered the public. It would be a disaster if the same mistake were made again.
On 11th December 2008 I got a letter form the HPC which said
in our opinion a lack of evidence of efficacy would not impede our ability to set standards or deal with complaints we receive. The vast majority of cases we consider are related to conduct.
But perhaps that is because they haven’t tried “regulating” quacks before. Now that the public is far more conscious about health fraud than it used to be, one can predict confidently that the HPC would be similarly overwhelmed by a deluge of complaints about the unjustified health claims made by acupuncturists, herbal medicine and traditional Chinese medicine practitioners. There is no shortage of them to complain about.
The education problem
The Pittilo report recommends that the entry level for registration should be a bachelors degree with honours. At first sight it seems reasonable to ask that practitioners should be ‘properly qualified’, but when one looks at what is actually taught on these degrees it becomes clear that they endanger, rather than protect, the public,
There are two very big problems with this recommendation.
Firstly, you can’t have a bachelors degree with honours until after you have decided whether or not there is anything useful to teach. If and when any of the subjects under consideration and shown to work to a useful extent, then it would be quite reasonable to establish degrees in them. Even the report does not pretend seriously that that stage has been reached. The proposal to set up degrees in subjects, at least some of which are quite likely to have no more than placebo value, is self-evidently nonsense,
The time for degrees, and the time for government endorsement by statutory regulation, is after the therapies have been shown to work, not before.
The absurdity of thinking that the public will be protected because a practitioner has a degree in, say, acupuncture, is shown with startling clarity by a recently revealed examination paper in acupuncture’
You can download the entire exam paper. Here are a few highlights from it.
So students, in 2009, are being taught the crudest form of vitalism.
Teaching of traditional Chinese medicine is just as bad. Here are two slides from a course run by the University of Westminster.
The first ‘explains’ the mysterious and entirly mythical “Qi”.
So “Qi” means breath, air, vapour, gas, energy, vitalism. This is meaningless nonsense.
The second slide shows the real dangers posed by the way Chinese medicine is taught, The symptoms listed at the top could easily be a clue to serious illness, yat students are taught to treat them with ginger. Degrees like this endanger the public.
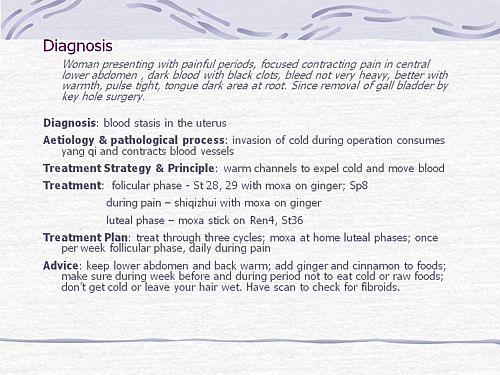
There are more mind-boggling slides from lectures on Chinese medicine and cancer: they show that what students are being taught is terrifyingly dangerous to patients.
It is entirely unacceptable that students are being taught these ancient myths as though they were true, and being encouraged to treat sick people on their basis. The effect of the Pittilo recommendations would be to force new generations of students to have this sort of thing forced on them. In fact the course for which this exam was set has already closed its doors. That is the right thing to do.
Here’s another example. The course leader for “BSc (Hons) Herbal Medicine” at the Univsrsity of Central Lancashire is Graeme Tobyn BA. But Tobyn is not only a herbalist but also an astrologer. In an interview he said
“At the end I asked her if I could cast her horoscope. She threw up her hands and said, ‘I knew this would happen if I came to an alternative practitioner.”
“I think the ruler of the ascendant was applying to Uranus in the ninth house, which was very pertinent.”
This would be preposterous even in the life style section of a downmarket women’s magazine, The Pittilo report wants to make degrees run my people like this compulsory. Luckily the Univerity of Central Lancashire is much more sensible and the course is being closed.
The matter is, in any case, being taken out of the hands of the government by the fact that universities are closing degrees in complementary medicine, including courses in some of those under discussion here, The University of Salford and the University of Central Lancashire have recently announced the closure of all the degree programmes in complementary and alternative medicine. The largest provider of such degrees, the University of Westminster has already shut down two of them, and the rest are being assessed at the moment. It is likely that the rest will be closed in the future.
The revelation that Westminster had been teaching its first year students that “amethysts emit high yin energy” and that students had been taught to diagnose disease and choose treatments by means of a dowsing pendulum, showed very clearly the sort of utter nonsense that undergraduates were being forced to learn to get a ‘bachelors degree with honours’. It stretches credulity to its limits to imagine that the public is protected by degrees like this. Precisely the opposite is true. The universities have recognised this, and shut the degrees. One exception is Professor Pittilo’s own university which continues to run a course in homeopathy, the most discredited of all the popular types alternative medicine.
A simpler, more effective and cheaper way to protect the public
I must certainly agree with the minister that protection of the public is an important matter. Having established that the Pittllo recommendations are more likely to endanger the public than protect them, it is essential to suggest alternative proposals that would work better.
Luckily, that is easy, because mechanisms already exist for dealing with the dangers that were listed above. The matter of adulteration, which is serious in traditional Chinese medicine, is a matter that is already the responsibility of the Office of Trading Standards. The major problem of false claims being made for treatment is also the responsibility of the Office of Trading Standards, which has a statutory duty to enforce the Unfair Trading Consumer Protection Regulations of May 2008. These laws state, for example, that
“One of the 31 commercial practices which are in all circumstances considered unfair is “falsely claiming that a product is able to cure illnesses, dysfunction or malformations”
The monitoring of false claims, and of side effects of treatments, is also the responsibility of the Medicines and Health Regulatory Authority (MHRA).
Rather than setting up complicated, expensive and ineffective ‘regulation’ by the HPC, all that need to be done is to ensure that the MHRA and/or Trading Standards have the funds to enforce existing laws. At the moment, they are not being implemented effectively, so I’d recommend that responsibility for enforcing the law against false health claims be transferred entirely to the MHRA, which has much more expertise in such matters than Trading Standards This would be both cheaper and more effective than the present system in which the responsibility is divided between the two organisations in an unclear way.
This proposal would protect the public against unsafe and adulterated treatments, and it would protect the public against false and fraudulent claims. That is what matters. It would do so more effectively,
more cheaply and more honestly than the Pittilo recommendations. There would be no reduction in patient choice either, There is no proposal to ban acupuncture, herbal medicine or traditional Chinese medicine. All that is necessary is to ensure that they don’t endanger the public.
Since the root of the problem lies in the fact that the evidence for the effectiveness is very weak. the question of efficacy, and cost-benefit ratio, should be referred to NICE. This was recommended by the House of Lords Report (2000). It is recommended again by the Smallwood report (sponsored by the Prince of Wales Foundation). It is baffling that this has not been done already. It does not seem wise to spend large amounts of money on new research at the moment, in the light of the fact that the US National Institutes of Health has already spent over $1 billion on such research without finding a single useful treatment.
The results of all this research has been to show that hardly any alternative treatment are effective. That cannot be ignored.
Conclusion
Recent events show that the halcyon days for alternative medicine are over. When the Pittilo report first appeared, it was greeted with derision in the media. For example, in The Times Alice Miles wrote
“This week came the publication of the Report to Ministers from the Department of Health Steering Group on the Statutory Regulation of Practitioners of Acupuncture, Herbal Medicine, Traditional Chinese Medicine and Other Traditional Medicine Systems Practised in the UK. Otherwise known as twaddle.”
In the Independent, Dominic Lawson wrote
So now we will have degrees in quackery.
What, really, is the difference between acupuncture and psychic surgery?
People will no doubt continue to use it and that is their right and their responsibility. But if the government were to accept the recommendations of the Pittilo report it would be seen, quite rightly, as being anti-scientific and of posing a danger to the public.
Fortunately there is a better, and cheaper, way to protect the public.
Follow-up
Margaret McCartney’s blog in the Financial Times puts rhw view of a GP with her usual sense, humour and incisiveness.
“This report would, if implemented, create lots more nonsense exam papers funded by a lot more public money – and would produce practitioners without the absolutely crucial skill of how to assess evidence and reject or use it appropriately”
The Times has covered the story (with some interesting comments) Consultation on how to regulate complementary and alternative therapies
Times Higher Education UK-wide consultation on CAM regulation is launched Excellent response from Andy Lewis.
The Sun has by far the best coverage up to now, Jane Symons writes “Regulating quacks helps them prey on gullible patients“
On 17th June 2009, 15 months after Singh’s article was published, the British Chiropractic Association (BCA) has finally produced its evidence (though only after enormous pressure from bloggers [download as pdf]..
Jack of Kent has already made some comments from the legal point of view.
As expected, the list of references they give is truly pathetic, The list of 29 references has nine about infantile colic, four about asthma (two of which refer to osteopathy not chiropractic). three about the safety of chiropractic (a contentious matter but not the point here) and three about the safety of non-steroidal anti-inflammatory drugs (an important matter but utterly irrelevant here).
Let’s look at the papers about colic. Most are in obscure alternative medicine journals, not easily available, but the BCA’s own synopsis is sufficient for now.
-
Klougart N, Nilsson N and Jacobsen J (1989) Infantile Colic Treated by Chiropractors: A Prospective Study of 316 Cases, J Manip Physiol Ther,12:281-288. [ download thr reprint]. As evidence it is about as useless as the infamous Spence study so beloved of homeopaths. There was no control group at all. It simply follows 316 babies and found that most of them eventually got better. Well, they do, don’t they? It is a sign of the pathetic standard of research in chiropractic that anyone should think this paper worth mentioning at all.
-
Mercer, C. and Nook, B. in the Proceedings of the 5th Biennial Congress of the World Federation of Chiropractic (1999) (so no peer review, for what that is worth). “Resolution of symptoms [of infantile colic] in 93% of infants treated with spinal manipulation”.. This sounds as useless as Klougart et al. Why only 93% one wonders? Every parent knows that 100 percent of babies stop crying eventually.
-
Wiberg et al. J Manip Physiol Ther, 1999, 242 517 – 522. This one was randomised (but not blind) and showed that spinal manipulation was as effective as dimethicone for colic. [Download pdf]
I expect that all that means is that dimethicone doesn’t work either. -
Hayden & Mullinger (2006) Complementary Ther. clin. Prac. “This preliminary study suggested that cranial osteopathic treatment can benefit infants with colic”. So. (a) preliminary and (b) not chiropractic.
-
Hipperson AJ (2004) Clinical Chiropractic 11, 122 – 129. A report of two case studies, so essentially worthless as evidence The journal isn’t even listed in Pubmed.
-
Browning M. Miller, J. Clinical Chiropractic (2008) 11, 122—129 [download pdf] Comparison of the short-term effects of chiropractic spinal manipulation and occipito-sacral decompression in the treatment of infant colic: A single-blinded, randomised, comparison trial. This paper just compared two different chiropractic methods. It shows that both are equally effective, or equally plausibly, both are equally ineffective.
- Leach RA (2002) J Manip Physiol Ther, 25, 58 -62. Merely two case reports and they refer to usie of a mechanical device, not the usual chiropractic manipulation.
-
Miller J (2007) Clinical Chiropractic 10, 139—146 Cry babies: A framework for chiropractic care [download pdf]. No evidence at all here. It isn’t a research paper.
- Nilsson N. 1985 Eur J Chiropr 33, 264 – 255 Infantile colic and chiropractic. “Respondents to a questionnaire revealed that 91% of of infants improved after 2 – 3 manipulations”. Again, no controls. So, babies stop crying, eventually.
That seems to be the best they can do. What they don’t do is mention any of the papers that contradict their claims. They cite Sackett et al. (1996) as their criterion for what constitutes evidence, That paper says “Evidence based medicine is the conscientious, explicit, and judicious use of current best evidence”. That means all the evidence. So why, for example, is there no mention of Olafsdottir et al. (2001), “Randomised controlled trial of infantile colic treated with chiropractic spinal manipulation”. That is one of the few really good papers in the area. It compared chiropractic treatment of babies for colic with placebo treatment (the nurse just held the baby for 10 minutes (the time the chiropractor took). The conclusion was
Conclusion Chiropractic spinal manipulation is no more effective than placebo in the treatment of infantile colic. This study emphasises the need for placebo controlled and blinded studies when investigating alternative methods to treat unpredictable conditions such as infantile colic.
More on this dishonest selectivity can be found at Holfordwatch.
No doubt there will soon be more analyses of what passes, in the eyes of the BCA, for evidence, The nine papers they cite for colic are truly pathetic. Not a single one of them amounts to anything that would be recognised as evidence in the real world. And papers that do provide real evidence are not mentioned.
Follow-up
As always, the blogs provided a very fast response to a document that appeared only late last night. And, as always, these unpaid people, working in their spare time, have done a far better job than the suits at the BCA (or NICE).
Here are some of them.
“A Review of The BCA’s Evidence for Chiropractic”. Martin on The Lay Scientist.
“The BCA have no evidence that chiropractic can help with ear infections” on Gimpy’s blog.
“Examining the BCA’S ‘Plethora’ of Evidence”. Unity, at Ministry of Truth.
“British Chiropractic Association and The Plethora of Evidence for Paediatric Asthma”. On Evidence Matters
“BCA Statement Baffles Blogger”. James Cole on jdc325’s Weblog
“Careful, BCA, you might slip a disk. The British Chiropractic Association may need to hire a chiropractor to work on themselves: they’re shoveling so hard they’re likely to hurt their backs.” In the US magazine, Discover.
“British Chiropractic Association (BCA) demonstrate what evidence-based medicine isn’t” at Holfordwatch. This one shows nicely how the BCA fail to apply their own standard of evidence, based on Sackett et al. (1996).
“The BCA’s worst day”. “Today has not been a good day for the British Chiropractic Association”. Jack of Kent summarises the demolition, in 24 hours, of the BCA’s ‘evidence’
Laurie Taylor says it all.
Could this bit (dated 18 June) in Laurie Taylor’s saga of the University of Poppleton possibly have been inspired by the Singh affair?
|
Sweet smell of success Our campus burst into colour last week as members of the Department of Aromatherapy, led by Professor Gwendolyn Frisson, paraded round the former administrative block happily waving bunches of wild carrot, devil’s claw, cinnamon leaf and lime blossom. What sparked the herbal celebration was the news of a full retraction from the journalist on the Poppleton Evening News who had described the department in print as “a hotchpotch of untestable propositions and unproven medical interventions”. The journalist in question, Simeon Rainbow, explained in his published retraction that he’d had time to reflect on the department’s reaction to his original article and now fully recognised that there was no better way of deciding upon the scientific validity of practices such as aromatherapy than by threatening anyone who denied such validity with an enormously costly libel action. Professor Frisson said that she welcomed the retraction. She would now be able to return with renewed enthusiasm to her research on the beneficial effects of grated angelica root on patients with advanced encephalitis. |
On 23rd May 2009, the Financial Times magazine published a six-page cover story about pseudo-scientific degrees by Richard Tomkins. The online version has the text but doesn’t do justice to the prominence that it was given. The print version had a much better title too, The Retreat from Reason. This article, which was some time in gestation, appeared shortly afte the last degree in homeopathy in the UK closed its doors. So perhaps it should have been called The Return of Reason. What’s interesting is that it has become commonplace for the mainstream newspapers to print articles like this and to dump some of their whackier lifestyle articles.
The print version had a much better title too, The Retreat from Reason, with a two-page spread..
They published the entire ‘Patients’ Guide to Magic Medicine‘ as a sidebar on page 4.
To these has now been added, inspired by Jack of Kent,
Libel: A very expensive remedy, to be used only when you have no evidence. Appeals to alternative practitioners because truth is irrelevant
One part of the article that I particularly enjoyed is this.
George Lewith, professor of health research at the University of Southampton’s medical school, is also director of the Centre for Complementary and Integrated Medicine, a private practice with clinics in Southampton and London’s West End, so it is no surprise that he is ready to speak out in support of complementary therapies. In fact, Southampton University – a member of the elite Russell Group – does not offer degree courses in complementary medicine, but Lewith defends the idea of offering them in principle, on the basis that, done properly, they produce better-trained practitioners. “Without the new universities’ involvement we might be faced with the quackery we saw in the 1940s and 1950s, when these people were outside medicine and were practising in an alternative fringe culture,” he says.
Sorry George, you are still an “alternative fringe culture”. And universities are realising that, and shutting down courses all over the place.
A response in the Finacial Times
The FT published one response in its letter column, A bilious attack on complementary medicine.
“Sir, Like many journalists, Richard Tomkins has been over-impressed by the scientific credentials of Professors David Colquhoun and Edzard Ernst as they carry on their absurdly over-stated, arrogant and irresponsible campaign against complementary medicine (“The retreat of reason”, May 23)”
and then the trump card
“Absence of evidence is not evidence of absence”
That’s the line used by quacks again and again and again (see, for example, integrative baloney @ Yale). I guess they have never heard of type 1 and type 2 errors. But that is a bit technical for homeopaths, so put it more simply. There is a quite remarkable absence of evidence for tooth fairies. So they must exist. Get it?
The letter is from Allen Parrott of Yeovil. Could that be the Allen Parrott of the British Acupuncture Accreditation Board? If so he is “is an adult educationist who was Dean of Adult and Community Education at Yeovil College and a lecturer in the School of Education at Exeter University. As well as his work for the Board, he is currently working as an educational adviser for the Kent, Surrey and Sussex Deanery in the NHS.”. So no reason to worry about the standards of education in Yeovil, then.
In March 2007 I wrote a piece in Nature on Science degrees without the science. At that time there were five “BSc” degrees in homeopathy. A couple of weeks ago I checked the UCAS site for start in 2009, and found there was only one full “BSc (hons)” left and that was at Westminster University.
Today I checked again and NOW THERE ARE NONE.
A phone call to the University of Westminster tonight confirmed that they have suspended entry to their BSc (Hons) homeopathy degree.
They say that they have done so because of “poor recruitment”. It was a purely financial decision. Nothing to do with embarrasment. Gratifying though it is that recruits for the course are vanishing, that statement is actually pretty appalling It says that the University of Westminster doesn’t care whether it’s nonsense, but only about whether it makes money.
Nevertheless the first part of this post is not entirely outdated before it even appeared, because homeopathy will still be taught as part of Complementary Therapies. And Naturopathy and “Nutritional Therapy” are still there..
According to their ‘School of Integrated Health‘, “The University of Westminster has a vision of health care for the 21st Century”. Yes, but it is what most people would call a vision of health care in the 18th century.
The revelation that the University of Westminster teaches that Amethysts emit high Yin energy caused something of a scandal.
Since then I have acquired from several sources quite a lot more of their teaching material, despite the fact that the university has refused to comply with the Freedom of Information Act.
In view of the rather silly internal review conducted by Westminster’s Vice-Chancellor, Professor Geoffrey Petts, this seems like a good moment to make a bit more of it public,
I think that revelation of the material is justified because it is in the
public interest to know how the University if Westminster is spending taxpayers’ money. Another motive is to defend the reputation of the post-1992 universities. I have every sympathy with the ex-polytechnics in their efforts to convert themselves into universities. In many ways they have succeeded. That effort
is impeded by teaching mystical versions of medicine.
If the University of Westminster is being brought into disrepute, blame its vice-chancellor, not me.
Homeopathic spiders
Here are a few slides from a lecture on how good spider venom is for you. It is from Course 3CTH502 Homeopathic Materia Medica II. No need to worry though, because they are talking about homeopathic spider venom, so there is nothing but sugar in the pills. The involvement of spiders is pure imagination. No more than mystical gobbledygook.
You are in hurry, or play with your fingers? You need spider venom pills (that contain no spider venom).

You break furniture? Time goes too fast for you? Try the tarantula-free tarantula pills.
You are preoccupied with sex? You play with ropes? What you need is Mygale (which contains no Mygale)

Much more seriously, the same sugar pills are recommended for serious conditions, chorea, ‘dim sight’, gonorrhoea, syphilis and burning hot urine.
This isn’t just preposterous made-up stuff. It is dangerous.
There is a whole lot more fantasy stuff in the handouts for Homeopathy Materia Medica II (3CTH502). Here are a couple of examples.
Aurum metallicum (metallic gold) [Download the whole handout]
Affinities MIND, VASCULAR SYSTEM, Nerves, Heart, Bones, Glands, Liver, Kidneys, RIGHT SIDE, Left side.
Causations Emotions. Ailments from disappointed love and grief, offence or unusual responsibility, abuse of mercury or allopathic drugs.
Aurum belongs to the syphilitic miasm but has elements of sycosis (Aur-Mur).
Potassium salts are the subject of some fine fantasy, in “The Kali’s” [sic]. (there is much more serious stuff to worry about here than a few misplaced apostrophes.). [Download the whole handout]
“The radioactive element of potassium emits negative electrons from the atom nucleus and is thought to be significant in the sphere of cell processes especially in relation to functions relating to automatism and rhythmicity.”
“Kali people are very conscientious with strong principles. They have their rules and they stick to them, ‘a man of his word’.”
“Potassium acts in a parasympathetic way, tending towards depression”
“They [“Kali people=] are not melancholic like the Natrum’s but rather optimistic.”
Radioactive potassium is involved in automaticity? Total nonsense.
Where is the science?
Yes, it is true that the students get a bit of real science. There isn’t the slightest trace that I can find of any attempt to resolve the obvious fact that what they are taught in the science bits contradict directly what they are told in the other bits. Sounds like a recipe for stress to me.
They even get a bit of incredibly elementary statistics. But they can’t even get that right. This slide is from PPP – Res Quant data analysis.
“Involves parameters and/or distributions”. This has no useful meaning whatsoever, that I can detect.
“Tests hypotheses when population distributions are skewed”. Well yes, though nothing there about forms of non-Gaussian properties other than skew, nothing about normalising transformations, and nothing about the Central Limit theorem.
“Ranks data rather than the actual data itself”. This is plain wrong. Randomisation tests on the original data are generally the best (uniformly most powerful) sort of non-parametric test. It seems to have escaped the attention of the tutor that ranking is a short-cut approximation that allowed tables to be constructed, before we had computers.
The students are told about randomised controlled trials. But amazingly in the lecture PPP-RCTs, the little matter of blinding is barely mantioned. And the teacher’s ideas about randomisation are a bit odd too.
Sorry, but if you fiddle the randomisation, no amount of “careful scrutiny” will rescue you from bias.
An Introduction to Naturopathic Philosophy
Naturopathy is just about as barmy as homeopathy. You can see something about it at the University of Wales. How about this slide from Westminster’s An Introduction to Naturopathic Philosophy.
So if you get tuberculosis, it isn’t caused by Mycobacterium tuberculosis? And the symptoms are “constructive”? So you don;t need to do anything. It’s all for the best really.
This isn’t just nonsense. It’s dangerous nonsense.
Traditional Chinese Medicine
Ever wondered what the mysterious “Qi” is? Worry no more. All is explained on this slide.

It means breath, air, vapour, gas, energy, vitalism. Or perhaps prana? Is that quite clear now?

What can we make of this one? Anyone can see that the description is barely written in English and that vital information is missing (such as the age of the woman). And it’s nonsense to suggest that “invasion of cold” (during keyhole surgery!) would cause prolonged constriction of blood vessels (never mind that it would “consume yang qi”). Not being a clinician, I showed it to an oncologist friend. He said that it was impossible to tell from the description whether the problem was serious or not, but that any abdominal pain should be investigated properly. There isn’t anything here about referral for proper investigation. Just a lot of stuff about ginger and cinnamon. Anyone who was taught in this way could be a real danger to the public. It isn’t harmless nonsense It’s potentially harmful nonsense.
And finally, it’s DETOX
Surely everyone knows by now that ‘detox’ is no more than a marketing word? Well not at the University of Westminster. They have a long handout that tells you all the usual myths and a few new ones.
It is written by Jennifer Harper-Deacon, who describes herself modestly, thus.
Jennifer Harper-Deacon is a qualified and registered Naturopath and acupuncturist who holds a PhD in Natural Health and MSc in Complementary Therapies. She is a gifted healer and Reiki Master who runs her own clinic in Surrey where she believes in treating the ‘whole’ person by using a combination of Chinese medicine and naturopathic techniques that she has qualified in, including nutritional medicine, Chinese and Western herbalism, homoeopathy, applied kinesiology, reflexology, therapeutic massage, aromatherapy and flower remedies.
It seems that there is no limit on the number of (mutually incompatible) forms of nuttiness that she believes. Here are a few quotations from her handout for Westminster students.
“Detoxification is the single most powerful tool used by natural health professionals to prevent and reverse disease”
What? To “prevent and reverse” malaria? tuberculosis? Parkinson’s disease? AIDS? cancer?
“When you go on to a raw food only diet, especially fruit, the stored toxins are brought up from the deep organs such as the liver and kidneys, to the superficial systems of elimination.”;
Very odd. I always though that kidneys were a system of elimination.
“The over-use and mis-use of antibiotics has weakened the body’s ability to attack and destroy new strains of resistant bacteria, virulent viruses, which have led to our immune system becoming compromised.”
Certainly over-use and mis-use are problems. But I always thought it was the bacteria that became resistant.
“The beauty about detoxification therapy is that it addresses the very causative issues of health problems”
That is another dangerous and silly myth. Tuberculosis is not caused by mythical and un-named “toxins”. It is caused by Mycobacterium tuberculosis.
“Naturopathy follows the logic of cause and effect therefore believes that we simply need pure food and water, sunshine, air, adequate rest and sleep coupled with the right amount of exercise for health.”
Try telling that to someone with AIDS.
“Colon cleansing is one of the most important parts of any detoxification programme.”
The strange obsession with enemas in the alternative world is always baffling.
“Frankincense: holds the capacity to physically strengthen our defence system and can rebuild energy levels when our immune system is weak. Revered as a herb of protection, frankincense can also strengthen our spiritual defences when our Wei qi is low, making us more susceptible to negative energies. This calming oil has the ability to deepen the breath, helping us to let go of stale air and emotions, making it ideal oil to use inhale prior to meditating.”
This is so much hot air. There is a bit of evidence that frankincense might have some anti-inflammatory action and that’s it.
But this has to be my favourite.
“Remember when shopping to favour fruits and vegetables which are in season and locally grown (and ideally organic) as they are more vibrationally compatible with the body.”
Locally grown vegetables are “more vibrationally compatible with the body”? Pure mystical gobbledygook. Words fail me.
OK there’s a whole lot more, but that will do for now.
It’s good that Westminster is shutting down its Homeopathy BSc, but it seems they have a bit further to go.
The Health Professions Council (HPC) is yet another regulatory quango.
The HPC’s strapline is
|
At present the HPC regulates; Arts therapists, biomedical scientists, chiropodists/podiatrists, clinical scientists, dietitians, occupational therapists, operating department practitioners, orthoptists, paramedics, physiotherapists, prosthetists/orthotists, radiographers and speech & language therapists.
These are thirteen very respectable jobs. With the possible exception of art therapists, nobody would doubt for a moment that they are scientific jobs, based on evidence. Dietitians, for example, are the real experts on nutrition (in contrast to “nutritional therapists” and the like, who are part of the alternative industry). That is just as well because the ten criteria for registration with the HPC say that aspirant groups must have
“Practise based on evidence of efficacy”
But then came the Pittilo report, about which I wrote a commentary in the Times, and here, A very bad report: gamma minus for the vice-chancellor, and here.
Both the Pittilo report, the HPC, and indeed the Department of Health itself (watch this space), seem quite unable to grasp the obvious fact that you cannot come up with any sensible form of regulation until after you have decided whether the ‘therapy’ works or whether it is so much nonsense.
In no sense can “the public be protected” by setting educational standards for nonsense. But this obvioua fact seems to be beyond the intellectual grasp of the quangoid box-ticking mentality.
That report recommended that the HPC should regulate also Medical Herbalists, Acupuncturists and Traditional Chinese Medicine Practitioners. Even more absurdly, it recommended degrees in these subjects, just at the moment that those universities who run them are beginning to realise that they are anti-scientific subjects and closing down degrees in them.
How could these three branches of the alternative medicine industry possibly be eligible to register with the HPC when one of the criteria for registration is that there must be “practise based on evidence of efficacy”?
Impossible, I hear you say. But if you said that, I fear you may have underestimated the capacity of the official mind for pure double-speak.
The HPC published a report on 11 September 2008, Regulation of Medical Herbalists, Acupuncturists and Traditional Chinese Medicine Practitioners.
The report says
1. Medical herbalists, acupuncturists and traditional Chinese medicine practitioners should be statutorily regulated in the public interest and for public safety reasons.
2. The Health Professions Council is appropriate as the regulator for these professions.
3. The accepted evidence of efficacy overall for these professions is limited, but regulation should proceed because it is in the public interest.
But the last conclusion contradicts directly the requirement for “practise based on evidence of efficacy”. I was curious about how this contradiction
could be resolved so I sent a list of questions. The full letter is here.
The letter was addressed to the president of the HPC, Anna van der Gaag, but with the customary discourtesy of such organisations, it was not answered by her but by Michael Guthrie, Head of Policy and Standards He said
“Our Council considered the report at its meeting in July 2008 and decided that the regulation of these groups was necessary on the grounds of public protection. The Council decided to make a recommendation to the Secretary of State for Health that these groups be regulated.
http://www.hpc-uk.org/assets/documents/100023FEcouncil_20080911_enclosure07.pdf “.
This, of course, doesn’t answer any of my questions. It does not explain how the public is protected by insisting on formal qualifications, if the qualifications
happen to teach mythical nonsense. Later the reply got into deeper water.
“I would additionally add that the new professions criteria are more focused on the process and structures of regulation, rather than the underlying rationale for regulation – the protection of members of the public. The Council considered the group’s report in light of a scoring against the criteria. The criteria on efficacy was one that was scored part met. As you have outlined in your email (and as discussed in the report itself) the evidence of efficacy (at least to western standards) is limited overall, particularly in the areas of herbal medicines and traditional Chinese medicine. However, the evidence base is growing and there was a recognition in the report that the individualised approach to practice in these areas did not lend themselves to traditional RCT research designs.”
Yes, based on process and structures (without engaging the brain it seems). Rather reminiscent of the great scandal in UK Social Services. It is right in one respect though.
The evidence base is indeed growing, But it is almost all negative evidence. Does the HPC not realise that? And what about “at least by Western standards”? Surely the HPC is not suggesting that UK health policy should be determined by the standards of evidence of Chinese herbalists? Actually it is doing exactly that since its assessment of evidence was based on the Pittilo report in which the evidence was assessed (very badly) by herbalists.
One despairs too about the statement that
“there was a recognition in the report that the individualised approach to practice in these areas did not lend themselves to traditional RCT research designs”
Yes of course the Pittilo report said that, because it was written by herbalists! Had the HPC bothered to read Ben Goldacre’s column in the Guardian they would have realised that there is no barrier at all to doing proper tests. It isn’t rocket science, though it seems that it is beyond the comprehension of the HPC.
So I followed the link to try again to find out why the HPC had reached the decision to breach its own rules. Page 10 of the HPC Council report says
3. The occupation must practise based on evidence of efficacy This criterion covers how a profession practises. The Council recognizes the centrality of evidence-based practice to modern health care and will assess applicant occupations for evidence that demonstrates that:
- Their practice is subject to research into its effectiveness. Suitable evidence would include publication in journals that are accepted as
learned by the health sciences and/or social care communities- There is an established scientific and measurable basis for measuring outcomes of their practice. This is a minimum—the Council welcomes
evidence of there being a scientific basis for other aspects of practice and the body of knowledge of an applicant occupation- It subscribes to the ethos of evidence-based practice, including being open to changing treatment strategies when the evidence is in favour
of doing so.
So that sounds fine. Except that research is rarely published in “journals that are accepted as learned by the health sciences”. And of course most of the good evidence is negative anyway. Nobody with the slightest knowledge of the literature could possibly think that these criteria are satisfied by Medical Herbalists, Acupuncturists and Traditional Chinese Medicine Practitioners.
So what does the HPC make of the evidence? Appendix 2 tells us. It goes through the criteria for HPS registration.
“Defined body of knowledge: There is a defined body of knowledge, although approaches to practice can vary within each area.”
There is no mention that the “body of knowledge” is, in many cases, nonsensical gobbledygook and, astonishingly this criterion was deemed to be “met”!.
This shows once again the sheer silliness of trying to apply a list of criteria without first judging whether the subject is based in reality,
Evidence of efficacy. There is limited widely accepted evidence of efficacy, although this could be partly explained by the nature of the professions in offering bespoke treatments to individual patients. This criterion is scored part met overall.
Sadly we are not told who deemed this criterion to be “part met”. But it does say that “This scoring has been undertaken based on the information outlined in the [Pittilo] report”. Since the assessment of evidence in that report was execrably bad (having been made by people who would lose their jobs if
they said anything negative). it is no wonder that the judgement is overoptimistic!
Did the HPC not notice the quality of the evidence presented in the Pittilo report? Apparently not. That is sheer incompetence.
Nevertheless the criterion was not “met”, so they can’t join HPC, right? Not at all. The Council simply decided to ignore its own rules.
On page 5 of the Council’s report we see this.
The Steering Group [Pittilo] argues that a lack of evidence of efficacy should not prevent regulation but that the professions should be encouraged and funded to strengthen the evidence base (p.11, p. 32, p.34).
This question can be a controversial area and the evidence base of these professions was the focus of some press attention following the report’s publication. An often raised argument against regulation in such circumstances is that it would give credibility in the public’s eyes to treatments that are not proven to be safe or efficacious.
This second point is dead right, but it is ignored. The Council then goes on to say
In terms of the HPC’s existing processes, a lack of ‘accepted’ evidence of efficacy is not a barrier to producing standards of proficiency or making decisions about fitness to practise cases.
This strikes me as ludicrous, incompetent, and at heart, dishonest.
There will be no sense in policy in this area until the question of efficacy is referred to NICE. Why didn’t the HPC recommend that? Why has it not been done?
One possible reason is that I discovered recently that, although there are two scientific advisers in the Department of Health,. both of them claim that it is “not their role” to give scientific advice in this area. So the questions get referred instead to the Prince of Wales Foundation. That is no way to run a ship.
The fact of the matter is that the HPC, like so many other regulatory agencies, fails utterly to protect the public from fraudulent and incompetent practitioners. In fact it actually protects them, in the same way that the financial ‘regulators’ protected fraudulent bankers. They all seem to think that ticking boxes and passing exams is an effective process. Even if the exams require you to memorise that amethysts “emit high Yin energy so transmuting lower energies and clearing and aligning energy disturbance as all levels of being”.
Recently I wrote a piece for the National Health Executive (“the Independent Journal for Senior Health Service Managers”), with the title Medicines that contain no medicine and other follies
In the interests of what journalists call balance (but might better be called equal time for the Flat Earth Society), an article appeared straight after mine, Integrating Homeopathy into Primary Care. It was by Rachel Roberts “Research consultant for the Society of Homeopaths”.
This defence was so appalling that I sent them a response (after first doing a bit of checking on its author). To my surprise, they published the response in full [download pdf of printed version]. Their title was

As always, the first step is to Google the author, to find out a bit more. It seems that Rachel Roberts runs a business Integrated Homeopathic Training. (a financial interest that was not mentioned in her article). She will sell you flash cards (‘Matmedcards’) for £70 (+£9 p&p) for 120 cards (yes, seriously). The card for Conium maculatum is remarkable. It says on the reverse side
Yes, it says (my emphasis)
“The poison used to execute Socrates. No 1 remedy for scirrhous breast cancer. Esp after blow to the breast”
No doubt she would claim that the word “remedy” was a special weasel word of homeopaths that did not imply any therapeutic efficacy. But its use in this context seems to me to be cruel deception, even murderous. It also appears to breach the Cancer Act 1939, as well as the Unfair Trading laws.
I asked the Bristol Trading Standards Office, and got a reply remarkably quickly. It ended thus.
“. . . . the use of the card for “hemlock” as an example amounts to advice in connection with the treatment (of cancer)”. I will initially write to IHT and require that they remove this, and any other, reference to cancer treatment from their website.
When I checked again a couple of weeks later, the hemlock sample card had been been replaced by one about chamomile (it is described as the opium of homeopathy. Luckily the pills contain no opium (and no chamomile either) or that would be breaking another law. Bafflingly, it is not (yet) against the law to sell pills that contain no trace of the ingredient on the label, if they are labelled ‘homeopathic’.
Presumably the packs still contain a claim to cure cancer. And what is said in the privacy of the consulting room will never be known.
Political correctness is a curious thing. I felt slightly guilty when I reported this breach of the Cancer Act. It felt almost sneaky. The feeling didn’t last long though. We are talking about sick people here.
It isn’t hard to imagine a desperate woman suffering from cancer reading that Ms Roberts knows the “No 1 remedy for scirrhous breast cancer”. She might actually believe it. She might buy some hemlock pills that contain no hemlock (or anything else). She might die as a result. It is not a joke. It is, literally, deadly serious.
It is also deadly serious that the Department of Health and some NHS managers are so stifled by political correctness that they refer to homeopaths as “professionals” and pay them money.
Ms Roberts, in her article, is at pains to point out that
|
 |
Well it is already well known that the the Code of Ethics of the Society of Homeopaths is something of a joke. This is just one more example.
The Code of Ethics, para 72 says homeopaths have a legal obligation
“To avoid making claims (whether explicit or implied; orally or in writing) implying cure of any named disease.”
Like, perhaps, claiming to have the “No 1 remedy for scirrhous breast cancer”?
Obviously voluntary self-regulation isn’t worth the paper it’s written on.
You don’t need to go to her web site to find “claims . . . implying cure of any named disease”. In her article she says
“Conditions which responded well to homeopathy included childhood eczema and asthma, migraine, menopausal problems, inflammatory bowel disease, irritable bowel syndrome, arthritis, depression and chronic fatigue syndrome.”
No doubt they will say that the claim that asthma and migraine “responded well” to their sugar pills carries no suggestion that they can cure a named disease. And if you believe that, you’ll believe anything.
I have to say that I find Ms Robert’s article exceedingly puzzling. It comes with 29 references, so it looks, to use Goldacre’s word, ‘sciencey’. If you read the references, and more importantly, know about all the work that isn’t referred to, you see it is the very opposite of science. I see only two options.
Either it is deliberate deception designed to make money, or it shows, to a mind-boggling extent, an inability to understand what constitutes evidence.
The latter, more charitable, view is supported by the fact that Ms Roberts trots out, yet again, the infamous 2005 Spence paper, as though it constituted evidence for anything at all. In this paper 6544 patients at the Bristol Homeopathic Hospital were asked if the felt better after attending the out-patient department. Half of them reported that the felt ‘better’ or ‘much better’. Another 20% said they were ‘slightly better’ (but that is what you say to be nice to the doctor). The patients were not compared with any other group at all. What could be less surprising than that half of the relatively minor complaints that get referred for homeopathy get ‘better or much better’ on their own?
This sort of study can’t even tell you if homeopathic treatment has a placebo effect, never mind that it has a real effect of its own. It is a sign of the desperation of homeopaths that they keep citing this work.
Whatever the reason, the conclusion is clear. Never seek advice from someone who has a financial interest in the outcome. Ms Roberts makes her living from homeopathy. If she were to come to the same conclusion as the rest of the world, that it is a placebo and a fraud, her income would vanish. It is asking too much of anyone to do that.
| This is the mistake made time and time again by the Department of Health and by the NHS. The Pittilo report does the same thing The execrably bad assessment of evidence in that report is, one suspects, not unrelated to the fact that it was done entirely by people who would lose their jobs if they were to come to any conclusion other than their treatments work. |  |
At present , the regulation of alternative medicine is chaotic because the government and the dozen or so different quangos involved are trying to regulate while avoiding the single most important question – do the treatments work?
They should now grasp that nettle and refer the question to NICE.
Follow-up
BSc courses in homeopathy are closing. Is it a victory for campaigners, or just the end of the Blair/Bush era?
The Guardian carries a nice article by Anthea Lipsett, The Opposite of Science (or download pdf of print version).
Dr Peter Davies, dean of Westminster’s school of integrated health, says
“he welcomes the debate but it isn’t as open as he would like.”
Well you can say that again. The University of Westminster has refused to send me anything much, and has used flimsy excuses to avoid complying with the Freedom of Information Act. Nevertheless a great deal has leaked out. Not just amethysts emit hig Yin energy, but a whole lot more (watch this space). Given what is already in the public, arena, how can they possibly say things like this?
“Those teaching the courses insist they are academically rigorous and scientific.”
There’s another remark from an unlikely source that I can agree with too. George Lewith, of Southampton University and Upper Harley Street, is quoted as saying
“The quality of degrees is an open joke . . . ”
Whatever next? [Note: Lewith told me later that he was quoted out of context by the Guardian, so it seems that after all he is happy with the courses. So sadly I have to withdraw the credit that I was giving him].
The article emphasises nicely the view that universities that run BSc degrees in things that are fundamentally the opposite of science are deceiving young people and corrupting science itself.
Professor Petts of Westminster seems to think that the problem can be solved by putting more science into the courses The rest of the world realises that as soon as you apply science to homeopathy or naturopathy, the whole subject vanishes in a puff of smoke, I fear that Professor Petts will have to do better,
“He [DC] believes the climate is starting to change after the Bush/Blair era where people believed in things because they wished they were true. “This has been going on for a generation and it’s about time for a swing in the other direction,” he suggests.”
Well, one can always hope.