
Download Lectures on Biostatistics (1971). Corrected and searchable version of Google books edition
Download review of Lectures on Biostatistics (THES, 1973).
advertisements
| “the report is more hypothesis-generating for future research than a rigorous scientific study. Find us some money and we will do a proper job. You can quote me for that.” Professor David Smith (Oxford). Scientific adviser for Food for the Brain. |
For a quick synopsis, look at Holfordmyths.org.
Patrick Holford and Drew Fobbester are joint researchers and authors of the Food for the Brain Child Survey , September 2007 (pdf). Holfordwatch has made a very thorough study of this report, in eight parts (so far). They conclude
“HolfordWatch can not share the optimism for these claimed benefits and finds that there is insufficient data to support them in a robust manner.”
There are many detailed questions, but the basic problem with the report is very simple. The fact that is (a) self-selected and (b) not randomised make it just another naive observational study. The stunningly obvious confounder in this case is, as so often, the socio-economic background of the kids. That was not even assessed, never mind any attempt being made to allow for it.
This isn’t just pedantry because what matters is causality. It is worth very little to know that eating vegetables is correlated with high SAT score if the correlation is a result of having well-off parents. If that were the reason, then forcing kids with poor parents to eat vegetables would make no difference to their SAT score because their parents would still be poor. The only conclusion of the study seems to be that we should eat more fruit and vegetables, something that we are already lectured about in every waking moment.
Many questions about the report have not yet been answered by its authors. But the report has a panel of scientific advisors, some of whom at least seem to be very respectable (though not ‘orthomolecular medicine‘, which is a cult founded on the batty late-life beliefs of the once great Linus Pauling that Vitamin C is a magic bullet).
Furthermore they are thanked thus
![]()
As it happens, David Smith is an old friend, so I wrote to him, and also to Philip Cowen, with some detailed questions. I didn’t get detailed answers, but the responses were none the less interesting. Cowen said
“I did see the report and quite agree with your conclusions that it an observational study and therefore not informative about causality.”
“The advice about diet seems reasonable although, as you point out, probably somewhat redundant.”
But still more interesting, David Smith told me (my emphasis)
“the survey was the largest of its kind and was done on minimal funding; hence several matters could not be dealt with and so the report is more hypothesis-generating for future research than a rigorous scientific study. Find us some money and we will do a proper job. You can quote me for that, if you wish.”
I’d grateful to David for his permission to quote this comment, It seems that Holford’s top scientific advisor agrees that it is not a rigorous study, and even agrees that the “proper job” is still to be done.
But it does seem a shame that that was not made clear in the report itself.
A merry christmas to one and all (or, depending on your mood, possibly bah humbug).
After the last post (and the next one), here’s something a bit lighter.
Last week I was in Brighton at the British Pharmacological Society Winter meeting in the Hilton Metropole (the less said about that hotel the better). The science was fun, but on Wednesday, I had a break to walk the length of Brighton Pier.
Here are few pictures.
Tarot consultant to GSK and Astra Zeneca

Just look at the notice in the stairs.

GSK and Astra Zeneca? Funny, Richard Sykes never mentioned the Tarot approach to drug discovery. Does it work as well as high-throughput screening?
The helter-skelter on Brighton pier
| For me that means only one thing: one of the best films ever made, Richard Attenborough’s Oh! What a Lovely War (1969). “The ever popular war game with songs battles & a few jokes”. All the lyrics can be found here. It isn’t easy to get, but Amazon now has a DVD.The film is based on Joan Littlewood’s 1963 musical of the same name. The First World War is run from the end of Brighton Pier.The picture shows the helter skelter, on December 19th 2007. |
 |
Most of the words in the film were quotations of what was actually said at the time. Chilling.
| Near the start. Negotiations fail: President Poincare (Ian Holm), Sir Edward Grey (Ralph Richardson) and Count Leopold Von Berchtold (John Gielgud). Hubris prevails on the beach and Field Marshal Sir Douglas Haig (John Mills) starts recruiting from a fairground booth. Click the picture to play clip [wmv file, 52 Mb] |
 |
| More hubris from Haig as the score is kept on the cricket scoreboard on the end of Brighton pier. First day: losses 60,000 men, ground gained, nil. Haig says “I feel that every step I take is guided by the divine will” (so no change then, just like Bush and Blair). Click the picture to play clip [wmv file, 26 Mb] |
 |
| The final scene. Iconic, beautiful, tear-jerking, sweeping shot of the South Downs. Click the picture to play clip [wmv file, 28 Mb]. And be very angry. |
 |
A Brighton shop window
A striking display, not least after recent events in Sudan.

The press releases (STOP PRESS)
Uhuh, here we go again.
All over the media we see headlines like “Honey ‘beats cough medicine’ “.
Take for example, the Daily Telegraph, where Ben Farmer writes “Honey is better at treating children’s coughs than an ingredient used in many over-the-counter medicines, according to new research”.
That is NOT what the research found This is what the research paper itself says (DM refers to the standard ‘cough suppressant’ dextromethorphan, which is already known to be ineffective).
| “honey was significantly superior to no treatment for cough frequency’ DM was not better than no treatment for any outcome. Comparison of honey with DM revealed no significant differences.” |
See it? No detectable difference between honey and standard cough medicine.
Everyone in the media misinterpreted what the paper said, but at least one blogger is already on to it, with Today’s “duh” study is a honey”.
At first sight, the results seem contradictory, No difference between honey and DM, No difference between DM and ‘no treatment’. So how can honey be better than ‘no treatment’?
The study was by Ian M. Paul, MD, MSc; Jessica Beiler, MPH; Amyee McMonagle, RN; Michele L. Shaffer, PhD; Laura Duda, MD; Cheston M. Berlin Jr, MD, published in Archives of Pediatrics & Adolescent Medicine 2007, 161, 1140 – 1146.
What was done
The design of this trial was pretty good apart from one thing Three things were compared (a) buckwheat honey, (b) a standard ‘cough suppressant’, dextromethorphan in a honey-flavoured syrup that was designed to be similar to the honey (DM for short), and (c) no treatment whatsoever.
The median age of the children who completed the study was 5.2 years (range, 2.2 – 16.9 years). They all had coughs attributed to upper respiratory tract infection. Thirty-five patients received honey, 33 received DM, and 37 received no treatment.The good thing is that the treatments were allocated randomly to the children, and that the person doing the assessment didn’t know which treatment each child had received. The children didn’t know whether they were getting honey or DM either, but they DID know when they got ‘no treatment’. The trial was carried out over two days. On day one nobody got a treatment, but they filled in a survey that asked, for example, “How frequent was your child’s coughing last night”. The parent had to tick one of seven boxes, from ‘not at all’ (score zero) to ‘extremely’ (score 6). They were then given the treatment allocated to them in a brown paper bag, so the person who gave it didn’t know which it was. The patients then went home and on the next day the same survey was completed by the same parent, over the telephone.
What happened?
First look at the raw data. Here is Figure 2 from the original paper.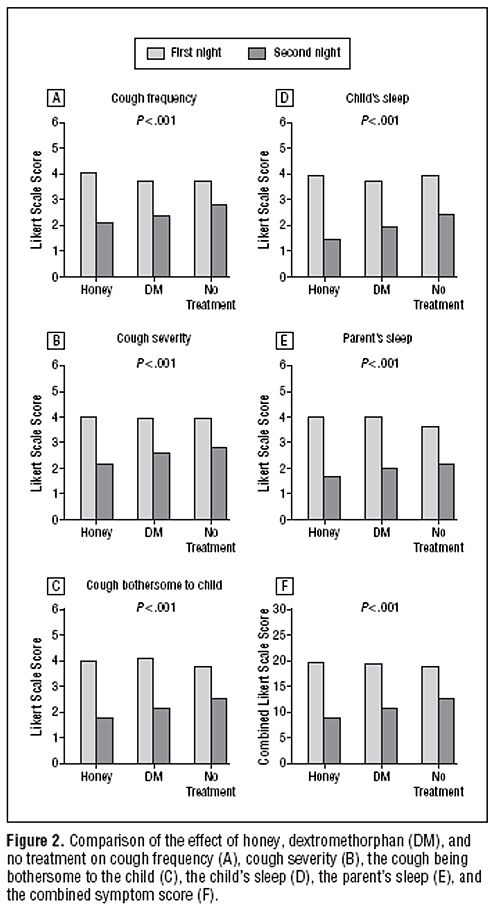 The charts show the results for 5 different measures of the severity of cough, and the last chart (F) shows the aggregate score for all the criteria.
The charts show the results for 5 different measures of the severity of cough, and the last chart (F) shows the aggregate score for all the criteria.
The first thing to notice is that there are no error bars on these charts. In my area, at least, no journal would accept a chart like this with no indication of scatter. There is a snag, though. Each patient acts as his/her own control, and that would not be reflected properly if errors bars were calculated for the numbers plotted in Fig. 2. It would therefore have been better to have a chart in which the difference in score between day 1 and day 2 was calculated from each patient, and the size of these differences plotted, with a standard deviation of the mean to indicate the amount of scatter in the observations. I have asked Dr Paul to send me a version that indicates the scatter of the numbers in this way (but I don’t think it will come).
The second thing to notice is that there is there is quite a big difference between the score on the first day (pale columns) and on the second day (dark columns), even in the no treatment group .
Thirdly, the pale columns are all much the same. On the first day the average score was about 4 (“a lot”) though on the second day, even with no treatment, the score fell quite a lot, to something between 2 (“a little”) and 3 (“somewhat”). This is a bit baffling because no treatment was given on either day. Presumably it results from the different settings in which the survey was given, or because the kids were getting better anyway.
Fourthly, insofar as the pale columns (baseline values) are all much the same, the thing you need to concentrate on is the difference, on each chart, between the height of the dark bars, for honey, DM and no treatment. These differences are pretty small, but on all the charts, the honey score is slightly smaller than the DM score, and the DM score is slightly smaller than the ‘no treatment’ score. What are we to make of that?
Here beginneth the statistical lesson.
Because the differences are small, and the scatter is quite big, we have to ask whether the differences are just random fluctuations rather than a result of any real difference between the treatments. That means we need statistics. Here is how the statistical argument works. Put roughly, we ask “how probable is it that the observations could arise by chance”. More precisely, the question is this. If there were no difference between the treatments, what is the probability that we would observe by chance a difference as big as, or bigger than, that seen in the experiment? (You need the subjunctive mood to explain statistics -pity it’s vanishing.)
Above each chart in the Figure we see P < 0.001. This means that there is less than a one in 1000 chance of the results arising by chance. More precisely, if all three treatments (honey, DM and no treatment) were actually identical, it is very unlikely that we’d see these results. The reasonable conclusion is, therefore, that all three treatments are not identical. The problem with this argument is that it tells you nothing about where the differences lie, so it is of no help whatsoever to a patient who is trying to decide what to do about a cough. The other problem is that it includes the ‘no treatment’ group, which was not blind. Both the children and parents were well aware that no treatment was given.
The most helpful comparison is really the properly-blinded comparison between honey and DM. And when this was looked at the result was no significant differences. In other words the small differences between the heights of the dark columns for honey and DM could perfectly well have arisen by chance if honey and DM were identical in their properties.
There isn’t any reason at all to think that honey is better than the standard (but ineffective) cough medicine.
The direct comparison between DM and ‘no treatment’ also shows no significant difference. Yet there are signs of a real difference between ‘no treatment’ and honey, though only for the cough frequency, not the other four measures. The aggregate measure (F in the figure) gave P = 0.04 for the comparison, so the authors are running a risk of 1 in 25 of being wrong in claiming a real effect. Although some people seem to regard a value of P = 0.05 as indicating a real effect, the fact that you’ll make a fool of yourself 1 time in 20 by claiming a real effect when none exists has never seemed to me to be good enough odds to stake one’s reputation on.
The ‘no treatment’ group certainly has some interest, but the fact that it was not blind means that the fact that honey was marginally better than ‘no treatment’ could perfectly well mean that taking honey has a better placebo effect that doing nothing at all. It provides no evidence at all that honey has any genuine therapeutic effect. If it had, one would then have to find out if the therapeutic effect was specific to buckwheat honey, or whether any old honey would do. It could be argued that even if the effect were real rather than placebo, the size of the effect is too small to make all that effort worthwhile.
A couple more things
It is already well known, from several good studies, that DM is useless, no better than placebo. This inconvenient fact has not yet reached many places that it should have (not even mentioned on wikipedia for example), but the American Academy of Pediatrics says
“Numerous prescription and nonprescription medications are currently available for suppression of cough, a common symptom in children. Because adverse effects and overdosage associated with the administration of cough and cold preparations in children have been reported, education of patients and parents about the lack of proven antitussive effects and the potential risks of these products is needed.”
The discussion in the paper by Paul et al, seems surprisingly upbeat about honey, in the light of their own findings. I’m surprised that they use the term ‘demulcent’ which I had thought to have died out, like the word ‘tonic’, on the grounds that it had no defined meaning
It is because meaningless terms and useless medicines die out eventually that medicine makes progress. The problem with alternative medicine is that nothing dies out: on the contrary they keep adding myths.
And finally
Always look at the end of the paper. On this one we see that the study was paid for by the National Honey Board. Dr Paul assures me that the funding source had no say in the design or analysis, which is as it should be.
Financial Disclosure: Dr Paul has been a consultant to the Consumer Healthcare Products Association and McNeil Consumer Healthcare.
Funding/Support: This work was supported by an unrestricted research grant from the National Honey Board, an industry-funded agency of the US Department of Agriculture.
So what is the practical outcome?
My conclusion from all this is simple. If you have got a cough, tough luck. There isn’t really anything available, conventional or alternative, that does much good. You’ll just have to wait for it to get better. But if you want to take something that tastes nice, why not honey? It almost certainly won’t do any good but it tastes good and it’s safer than the standard cough medicine.
The sponsor’s interpretation
It seems that the sponsor of the work is happy with the misinterpretation.
Charlotte Jordan a project manager of research at the National Honey Board, believes the finding confirms what your grandmother told you.
“This is a really exciting finding,” she said. “For a long time it’s been folklore medicine to use honey when you have a cough or a cold, but it’s exciting to have a scientific study to back that up.”
Just one problem, That is NOT what the paper says.
How did all this mis-reporting happen?
One reason is misleading press releases. Universities and Academic journals now engage in shameless PR, spin and hype. They prostitute good science.
Download press releases from Penn State, JAMA and Press Association [pdf file]
Here is the highly misleading bit of hype that came from the Press Office of the Pennsylvania State University. The headline is “Honey a better option for childhood cough than OTCs” (OTC means over-the-counter medicines that contain DM). That contradicts directly the paper which says “Comparison of honey with DM revealed no significant differences”.
Likewise the statement in the Penn State release “Honey did a better job reducing the severity, frequency and bothersome nature of nighttime cough from upper respiratory infection than DM or no treatment” is equally incompatible with “Comparison of honey with DM revealed no significant differences”. Its only possible justification is from the 3 way comparison by analysis of variance and that does not tell us what we need to know.
To make matters worse, the media office is not to blame this time. Ms Manlove told me tonight that the press release had been approved by Dr Paul himself.
| Contact: Megan W. Manlove Penn State Honey a better option for childhood cough than OTCs A new study by a Penn State College of Medicine research team found that honey may offer parents an effective and safe alternative than over the counter children’s cough medicines. The study found that a small dose of buckwheat honey given before bedtime provided better relief of nighttime cough and sleep difficulty in children than no treatment or dextromethorphan (DM), a cough suppressant found in many over-the-counter cold medications. Honey did a better job reducing the severity, frequency and bothersome nature of nighttime cough from upper respiratory infection than DM or no treatment. Honey also showed a positive effect on the sleep quality of both the coughing child and the child’s parents. DM was not significantly better at alleviating symptoms than no treatment. . . . |
All that Candice Yakel, of the Office for Research Protections at Penn State had ro say in the matter was
“Our investigators stand by the conclusions of the study as reported in the Archives of Pediatric and Adolescent Medicine and as characterized in our press release of December 3, 2007.”
And here is the equally misleading bit of hype issued by the Journal of the American Medical Association (Ms Manlove tells me that this was also approved bt Dr Paul).
| JAMA and Archives Journals Study suggests honey may help relieve children’s cough, improve sleep during colds
|
The Press Association release was equally bad, and probably the one used by many of the reporters as a basis for stories in the media. The opening statement is totally wrong.
| 1 HEALTH Honey Embargoed to 2100 Monday December 3 HONEY BEST FOR KIDDIES’ COUGHS SAY RESEARCHERS By John von Radowitz, PA Science Correspondent Natural honey is a better remedy for children’s coughs than expensive over-the-counter medicines, researchers said today. A dose of buckwheat honey before bedtime easily outperformed a cough suppressant widely used in commercial treatments, a US study found. . . . |
Follow-up
There is a review of over-the-counter cough medicines in the BMJ (2002) [free full text]. It concludes “Recommendation of over the counter cough medicines to patients is not justified by current evidence”.
This advertisement has to be one of the sneakiest bits of spin that I’ve seen in a while. It appeared in today’s Guardian. And a lot more people will see it than will look at the homeopathic nonsense on the Boots ‘education’ site.
What on earth does it mean? One interpretation could be this. We can’t make false claims for Vitamin(s) B in print, but your Boots Pharmacy Team will be happy to do so in private. OK gang, let’s find out. Get out there and ask them. I’ll be happy to post the answers you get (one of those little mp3 recorders is useful).

The Boots web site isn’t much better. Their Vitality Overview says
“The following vitamins and supplements are important for vitality..
B Vitamins
Ginkgo biloba
Ginseng
Iron
Magnesium
Vitamin C”
Needless to say “vitality” isn’t defined and there is the slightest reason to think that any of these things help the “energy level” of any person on a normal diet.
Sting number 1
I went into a large branch of Boots and asked to speak to a pharmacist. This what ensued (BP= Boots Pharmacist).
DC. My eye was caught by your advertisement. I’m pretty healthy for my age but I do get very tired sometimes and it says “ask your Boots pharmacy team, so what can you recommend?”
BP. “Well basically it helps release energy from your cells so you’ll feel more energetic if you have enough vitamin B in your, eh, blood system”
DC. “Ah, I see, I’ll feel more energetic?”
BP. “yes you’ll feel more energetic because it releases the energy from the cells ”
DC. “which vitamin B does that?”
BP. “It’s a complex. it has all the vitamins in it.”
DC. “So which one is it that makes you feel more energetic?”
BP. “Vitamin B”
DC. “All of them? ”
BP. “All of them. It’s mainly vitamin B12”
DC. “Vitamin B12. That makes you feel more energetic?”
BP. “Yes. B12 and B6.”
DC. “hmm B12 and B6. I wasn’t aware of that before so I’m a bit puzzled. I mean, vitamin B12. I thought that was for pernicious anaemia.”
At this point I think the pharmacist was getting a bit suspicious about all my questions (and spotted the recorder) and began to back off.
BP. “Not necessarily. You know its got [pause], basically what its [pause], if you have enough in your diet there’s no need to take an extra vitamin B.” . . .”This is really for people who are on the go and are, you know, unable to get fresh meals.”
Then the senior pharmacist (SP) was called and I repeated the question.
DC. “Will it give me extra energy? It says I should ask my Boots Pharmacy team about that.”
SP. “It may do, yes. It depends on your own body’s individual reaction to it.” . . . “To be honest I’m not the best person to ask about clinical data on it. If you have more detailed questions I can send them to head office”
At this point. I gave up. The first pharmacist ended up with reasonable advice, but only after she’d obviously become suspicious about all my questions (and spotted the recorder). The senior pharmacist just fudged it when asked a direct question. Initially, the ‘expert advice’ was pure gobbledygook. What does one make of it? The fact that I got the right answer in the end, one could argue, makes the first part worse rather than better. She knew the right answer, but didn’t give it straight away. Instead she talked a lot of nonsense in which two quite different meanings of the word ‘energy’ were confused in a way that is only too familiar in the supplement huckster business. I’m not impressed.
Sting number 2
An email enquiry to Boots customer service asked whether Vitamin B really helped ‘vitality’. It elicited this hilarious non-response (original spelling retained).
| Dear Mrs M*** Thank you for contacting us regarding an advertisement you have seen in relation to the benifits to vitamin C. Unfortunately as I am not medically trained I would be unable to provide you with advice on this particular product. I would however, advise that you contact our pharmacy team at your local store via the telephone directly. You’ll find that they will be more than happy to help you further. |
Aha, so the Pharmacy Team are medically-trained?