
Download Lectures on Biostatistics (1971). Corrected and searchable version of Google books edition
Download review of Lectures on Biostatistics (THES, 1973).
chiropractic
The first post was NICE falls for Bait and Switch by acupuncturists and chiropractors: it has let down the public and itself.
That was followed by NICE fiasco, part 2. Rawlins should withdraw guidance and start again.
Since then, something of a maelstrom has engulfed NICE, so it’s time for an update.
It isn’t only those who are appalled that NHS should endorse voodoo medicine on the basis of very slim evidence who are asking NICE to rethink their guidance on low back pain. Pain specialists are up in arms too, and have even started a blog, ‘Not Nearly as NICE as you think …‘, to express their views. Equally adverse opinions are being expressed in the Britsh Medical Journal. A letter there is signed by over 50 specialists in pain medicine. It ends thus
“Because of these new guidelines patients will continue to experience unnecessary pain and suffering and their rights to appropriately individually tailored treatment have been removed on the basis of a flawed analysis of available evidence. We believe the guidelines do not reflect best practice, remove patient choice and are not in our patients’ best interests.”
In a contribution headed “NICE misguidance”. Dr Michel Vagg ends
It seems to me that this guideline has been used as a propaganda vehicle to allow cherry-picked evidence to be enshrined as doctrine. This is an abuse of the guideline development process . . . ”
I have to say, though, that it seems to me that some of these people are promoting their own interests as much as chiropractors and acupuncturists. The evidence that spinal injections produce worthwhile benefits seems to be as thin as the evidence that chiropractic and acupuncture produce worthwhile benefits. But no doubt the injections are good for the budgets of PCTs or private practice doctors.. Could it perhaps be the case that some of the clinicians’ anger is being generated by doctors who are rushing to defend their own favourite ineffective treatment?
Why, oh why, can’t either NICE or the pain consultants bring themselves to state the obvious, that nothing works very well. The only thing that can be said for most of the regular treatments is that although they may not be much more effective than acupuncture or chiropractic, at least they don’t come with the intellectually-offensive hokum that accompanies the latter. Very sensible attempts have been made to identify the cause of low back pain [reviewed here], Occasionally they succeed. Mostly they don’t.
One clinician’s letter deserves special attention because it goes into the evidence, and the costs, in some detail. Its conclusions are very different from those in the NICE guidance.
The letter, a Review of NICE guidance, is from Dr C.J.D. Wells [download the whole letter]. He is a pain relief consultant from Liverpool.
Let’s look at some highlights.
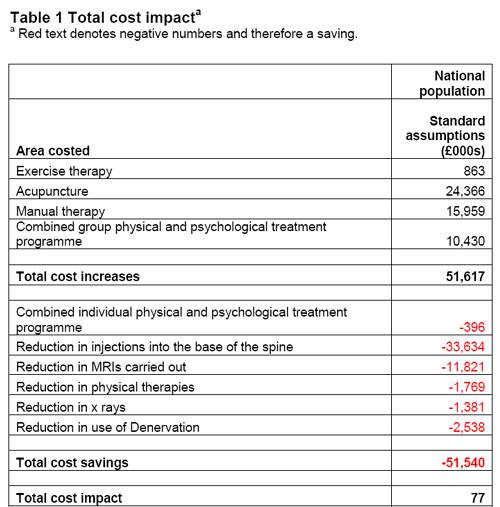
Wells points out the absurdity of the cost estimates
“In the pricing section, they estimate that this will require an increase of facilities so that 3,500 patients can be treated instead of 1,000 at present (again see comments on pricing). This is not many treatments for the 20 million sufferers, of whom we can estimate that at least 2 million will have significant long-term disability and psychological distress”
And that is without even costing all the secondary costs of miseducating a new generation of students in fables about “Qi”, meridians, energy flow, subluxations and innate intelligence.
“The abysmal ignorance of the committee is reflected in the poor overall advice. So if you have a committee with special interests in Exercise, Manipulation, PMP’s, and Surgery, and you call an expert on Acupuncture, you get advice to use Exercise, Manipulation, Acupuncture, PMP’s and Surgery. Amazing.”
Another pain consutant, Charles Guaci, says in a comment in the Daily Mail.
I am a Pain Consultant of 30 years experience, have published two books (one translated into different languages).
NICE never asked me for my opinion.
This is the most ridicuculous pseudo-scientific document I have ever seen.
The panel consisted of a surgeon, psychologist, osteopath, acupuncturist a physiotherapist and an academic; not one pain consultant! The conclusions are simply a means of increasing the employment of their friends!
All evidence submitted to NICE was ignored.
It is almost certain than unless NICE rethink their ideas that Pain Consultants will be seeking a judicial review as well as full disclosure of how the panel arrived at their bizarre findings under the Freedom of information act.
Patients should realise that they are being taken for a ride.
Despite the outcry from opponents of magic medicine and from pain specialists, the assessment by the normally excellent NHS Choices site was disappointing. It made no mention at all of the secondary consequences of recommending CAM and described the assertions of the guidance group quite uncritically.
The reputation of NICE
NICE has been criticised before, though usually unjustly. In the past I have often supported them. For example. when NICE said that treatment of dementia with anticholinesterase drugs like galantamine was ineffective, there was a great outcry, but NICE were quite right. There is little or no rationale for such treatments, and more importantly, very little evidence that they work. But patients, especially when they are desperate, have greater faith in drug treatments than most pharmacologists, They want to clutch at straws. A bit like the NICE guidance committee, faced with a bunch of treatments most of which are almost ineffective, clutched at the straws of acupuncture and chiropractic. But this time it isn’t only the patients who are cross. It is most of the medical and scientific world too.
One interpretation of these bizarre events is that they represent a case of medical/scientific arrogance. Ben Goldacre wrote of another aspect of the same problem thus week, in Dodgy academic PR [download the paper on which this is based].
The first job of a scientist is to say openly when the answer to a question is not known. But scientists are under constant pressure to exaggerate the importance of their results. Last year we published an article which I feel may, if verified, turn out to be the second most important that I have ever been an author on. Because it happened to be published in Nature (not because of its quality), a press release was written (by an arts graduate!). It took some argument to prevent the distorted and exaggerated account being imposed on the public. This is typical of the sort of thing reported in Goldacre’s column. I reported a similar case a while ago, Why honey isn’t a wonder cough cure: more academic spin.
If NICE does not reconsider this guidance, it is hard to see how it can be taken seriously in the future. I hope that when NICE’s director, Professor Sir Michael Rawlins, returns from his trips abroad, he will find time to look at the case himself.
Indirectly, then, it can be argued that NICE’s bizarre guidance is just another manifestation of the management of science being passed from the hands of scientists into the hands of administrators and spin experts. It is yet another example of DC’s rule
Never trust anyone who uses the word ‘stakeholder’
Some bone-headed bureaucrat decides that any charlatan or quack is a ‘stakeholder’ in the provision of NHS care and gives them a quite disproportionate say in how taxpayers’ money is spent. The bureaucrats are so busy following processes and procedures, ticking boxes, and so deficient in scientific education, that they failed to notice that they’ve been caught out by the old trick of used car salesmen, bait and switch.
The consequences
The expected consequences have already started to materialise. The Prince of Wales’ Foundation for Magic Medicine is jubilant about having been endorsed by NICE. And I’m told that “The chiropractors have now just written letters to all health boards in Scotland asking for contracts for their services to deal with back pain”.
There could hardly have been a worse time for NICE to endorse chiropractic. We are in the middle of a storm about free speech because of the disgraceful action of the British Chiropractic Associaton in suing one of our best science writers, Simon Singh, for defamation because he had the temerity to express an opinion, Of course, even if the BCA wins in court, it will be the overall loser, because chiropractic claims are now being scrutinised as never before (just look at what they told me).
Follow-up
A much-cited paper. The paper that is most often cited by chiropractors who claim to be able to cure colic by spinal manipulation is Klougart N, Nilsson N and Jacobsen J (1989) Infantile Colic Treated by Chiropractors: A Prospective Study of 316 Cases, J Manip Physiol Ther,12:281-288. This is not easy to get hold of but Steve Vogel has sent me s scanned copy which you can download here. As evidence it is about as useless as the infamous Spence study so beloved of homeopaths. There was no control group at all. It simply follows 316 babies and found that most of them eventually got better. Well, they do, don’t they? It is a sign of the pathetic standard of reaearch in chiropractic that anyone should think this paper worth mentioning at all.
June 6 2009. More flak for NICE from the Royal College of Anaesthetists, and more adverse comment in the BMJ. And of course the blogs. for example, “If this is “evidence based medicine” I want my old job back“.
“Acupuncture on the NHS: a dangerous precedent”: a good analysis at counterknowledge.com.
June 6 2009, Comment sent to the BMJ. The comment was submitted, as below, early on Friday 5th June. The BMJ said it was a “sensitive issue” and for the next five days lawyers pondered over it.
Underwood and Littlejohns describe their guidance as being a “landmark”. I can only agree with that description. It is the first time that NICE has ever endorsed alternative medicine in the face of all the evidence. The guidance group could hardly have picked a worse moment to endorse chiropractic. Chiropractors find it so hard to find evidence for their practices that, when one of our finest science writers, Simon Singh, asked to see the evidence they sued him for defamation. I suggest that the guidance group should look at the formidable list of people who are supporting Singh, after his brave decision to appeal against this iniquitous persecution.
Of course I’m sure this bizarre decision has nothing to do with the presence on the guidance group of Peter Dixon, chair of the General Chiropractic Council. Nevertheless, I am curious to know why it is that when I telephoned two of the practices belonging to Peter Dixon Associates, I was told that they could probably treat infantile colic and asthma. Such claims have just been condemned by the Advertising Standards Authority.
The low back pain guidance stands a good chance of destroying NICE’s previously excellent reputation for dispassionate assessment of benefits and costs. Yes, that is indeed a landmark of sorts.
If NICE is ever to recover its reputation, I think that it will have to start again. Next time it will have to admit openly that none of the treatments work very well in most cases. And it will have to recognise properly the disastrous cultural consequences of giving endorsement to people who, when asked to produce evidence, resort to legal intimidation.
Eventually, on Wednesday 10 June the comment appeared in the BMJ, and it wasn’t greatly changed. Nevertheless if is yet another example of legal chill. This is the final version.
Underwood and Littlejohns describe their guidance as being a “landmark”. I can only agree with that description. It is the first time that NICE has ever endorsed alternative medicine in the face of all the evidence. The guidance group could hardly have picked a worse moment to endorse chiropractic. Chiropractors are so sensitive about criticisms of their practices that, when one of our finest science writers, Simon Singh, queried the evidence-base for their therapeutic claims they sued him for defamation. I suggest that the guidance group should look at the formidable list of people who are supporting Singh, after his brave decision to appeal against an illiberal court ruling in this iniquitous persecution.
One wonders whether this bizarre decision by NICE has anything to do with the presence on the guidance group of Peter Dixon, chair of the General Chiropractic Council. I am also curious to know why it is that when I telephoned two of the practices belonging to Peter Dixon Associates, I was told that chiropractic could be effective in the treatment of infantile colic and asthma. Similar claims about treating colic have just been condemned by the Advertising Standards Authority.
The low back pain guidance stands a good chance of destroying NICE’s previously excellent reputation for dispassionate assessment of benefits and costs. Yes, that is indeed a landmark of sorts.
If NICE is ever to recover its reputation, I think that it will have to start again. Next time it will have to admit openly that none of the treatments works very well in most cases. And it will have to recognise properly the disastrous cultural consequences of giving endorsement to people who, instead of engaging in scientific debate, resort to legal intimidation.
Bait and switch. Oh dear, oh dear. Just look at this. British Chiropractic Association tell their members to hide their sins from prying eyes.
Excellent round-up of the recent outburst of writing about “chiroquacktic” (Tut, tut, is there no respect?).
Dr Crippen writes “NICE recommends a cure for all known disease” [Ed some exaggeration, surely]
Two days ago I wrote NICE falls for Bait and Switch by acupuncturists and chiropractors: it has let down the public and itself
Now the official ‘guidance’ is out, and it is indeed quite as bad as the draft.
The relevant bits now read thus.
- Offer one of the following treatment options, taking into account patient preference: an exercise programme, a course of manual therapy or a course of acupuncture. Consider offering another of these options if the chosen treatment does not result in satisfactory improvement.
- Consider offering a structured exercise programme tailored to the person:
- This should comprise of up to a maximum of 8 sessions over a period of up to 12 weeks.
- Offer a group supervised exercise programme, in a group of up to 10 people.
- A one-to-one supervised exercise programme may be offered if a group programme is not suitable for a particular person.
- Consider offering a course of manual therapy, including spinal manipulation, comprising up to a maximum of nine sessions over a period of up to 12 weeks
- Consider offering a course of acupuncture needling comprising up to a maximum of 10 sessions over a period of up to 12 weeks.
The summary guidance still doesn’t mention chiropractic explicitly, just a coy reference to “spinal manipulation”. At a time when the British Chiropractic Association is busy trying to suppress free speech via the law courts, I guess it isn’t surprising that they don’t like to use the word.
The bias in the recommendations is perhaps not surprising because the guidance development group had a heavy representation from alternative medicine advocates, and of people with a record of what, is, in my view, excessive tolerance of mumbo-jumbo.
Royal College of General Practitioners (RCGP) played a large part in writing the guidance. That is an organisation thar has steadfastly refused to make any sort of sensible statement of policy about magic medicine. It isn’t long since I was told by a senior person at the RCGP that there was nothing odd about neuro-linguistic programming. That does not bode well.
Professor Martin Underwood, Professor of Primary Care Research Warwick Medical School, University of Warwick. Underwood chaired the guidance development group. Martin Underwood is also a GP in Coventry See also the British Osteopathic Association. Underwood was lead author of the BEAM trial (download reprint). It is well worth reading the comments on this trial too. It was a randomised trial (though not, of course, blind).
|
Our main aim was to estimate, for patients consulting their general practitioner with back pain, the effectiveness of adding the following to best care in general practice: a class based exercise programme (“back to fitness”), a package of treatment by a spinal manipulator (chiropractor, osteopath, or physiotherapist), or manipulation followed by exercise Conclusions |
In other words, none of them worked very well. The paper failed to distinguish between manipulation by physiotherapists, chiropractors and osteopaths and so missed a valuable chance to find out whether there is an advantage to employing people from alternative medicine (the very problem that this NICE guidance should have dealt with)
Steve Vogel, another member of the guidance development group, is an osteopath. Osteopathy has cast off its shady origins better than chiropractic, but it remains a largely evidence-free zone, and is still usually classified as alternative medicine.
Peter Dixon DC FCC FBCA is chairman of the General Chiropractic Council and founder of Peter Dixon Associates. They run six chiropractic clinics. The claims made by these clinics on their web site are mostly related to musculo-skeletal conditions (not, all spine-related however). But they also include
“Chiropractic is also suitable for relieving the symptoms of stress, and optimizing the way the body works is one of the best ways of enhancing health and wellbeing.”
I wonder how they could justify that claim? Then we get
A chiropractor is always willing to discuss individual conditions or answer questions in order to assess whether chiropractic may be of benefit.
Thanks for the invitation. I accepted it. After the first two phone calls, I had learned all I needed.
The first of Peter Dixon’s clinics that I called, was asked about my son who was suffeiing from perpetual colic. I asked for advice. I was put through to the chiropractor. Here are some extracts from the conversation.
“I think now it’s termed irritable baby syndrome. . . . . We’ve found chiropractic is very effective for colic . . . . £50 up to 3/4 hour which would involve taking a case history, examining the baby, with regard to seeing how the joints in the spine work because often colic is down to, er um, faulty movement patterns in the spine. We deal with an awful lot of things to do with the frame -how the spine moves -and it’s often problems with the way that the bones of the spine move in infants and babies that is the underlying cause in colicky symptoms. . . usually on the whole, I’ve shot myself in the foot by saying this in the past, if there are -um when I say back problems they’re usually temporary issues -when they are there the response for most babies is quite quick . . . it depends on how it’s related to what’s gone on in the birth process -there is usually some traumatic cause and it usually sets up a problem in the upper neck or the mid-back and that will drive those colic symptoms. . . . Yes it’s quite a straightforward thing we just check the baby’s spine and see if it’s problem we can deal with or not.”
Yes, I think you just shot yourself in the foot again. I have no idea in what fraction of cases a chiropractor would fail to claim that it was a case that they could deal with. At least that possibility was envisaged. But when I asked where he’d refer me to in such case I was told it might be a result of bottle feeding -“what they consume”. So I expect it would have been sent to some sort of “nutritional therapist” who would have used one of their usual battery of unreliable tests for food allergies.
I tried a second clinic in Peter Dixon’s empire and asked if chiropractic could help with asthma.”It can do, depending on what type of asthma you have". After some questions I was asked
“Do you have any general aches and pains otherwise, any tension .problems round the rib cage or thoracic spine . . . There are two things we’d look as chiropractors as to whether we could help or not and that would include the tension round the rib cage -in any type of asthma you’ll become tight round the rib cage and merely by keeping that area loose you’d help to stop the asthma from becoming quite as bad. And the second part is we’d look at the neck area with you to see if there is any restriction there -which houses the nerve supply to the lungs which can be indicated in some asthma cases also.”
I was invited to come for a free screen, so I asked if it usually worked quickly, “It depends what the problem is but you’d need a course I suspect”. £45 for the first appointment then £28 per session. “In most cases you’d need to look at a six to eight session course”.
Would anyone with experience of crying babies or of asthma like to comment on these proposed treatments? They are not my idea of evidence-based treatments and I find it quite surprising that someone who sponsors them is thought appropriate to write guidance for NICE.
This sort of ‘sting’ always makes me feel a bit uneasy, but it seems to be the only way to find out what actually goes on. And what goes on has all the appearance of classic bait and switch. You go in for your backache, and before you know where you are you are being sold a course of treatment to stop your baby crying.
Media follow-up after the NICE announcement
Sadly, I heard that the Today programme (my favourite news programme) was pretty wet. if only their science reporting was as good as their politics reporting.
The 27th May was certainly pretty busy for me, Apart from a couple of local paper interviews, this is what happened,
Sky News TV. Richard Suchet and two cameraman came to UCL and filmed a lot of stuff out of which a 20 second clip was used. And then they grumble that they don’t make money.
BBC TV 6 o’clock News. Similar, but at least only two people this time. Both TV stations spent ages showing pictures of people having needles pushed into them and very little time discussing the problems. A pathetically bad attempt at science reporting. Radio, on the whole, did much better
BBC Three Counties Radio (09.20) Host Ronnie Barbour, The daytime talk shows may be appalling to some of us, but the hosts did a far better job of airing the problems than TV [download the mp3].
Radio 5 Live Victoria Derbyshire [download the mp3]
BBC Radio Sheffield (12.05) was the best talk show by far. First speaker was Steve Vogel, the osteopath from the guidance development group. Although invited by the rather sensible host, Rony, to respond to the idea that a secondary consequence of the guidance would be to introduce hocus-pocus, he steadfastly refused to answer the question. At the end a rather sensible GP summed up the view from the coalface. [play the mp3]
Radio 4 PM programme This excellent early evening news programme is run by Eddie Mair. It was the best interview yet. The other side was put by Martin Underwood, chair of the guidance development group [play the mp3]
Underwood said “the evidence shows that it [acupuncture] works”. I disagree. The evidence shows that acupuncture, in a non-blind comparison with no acupuncture shows a small, variable additional effect that doesn’t last and is of marginal clinical significance, That is not what I call “works”. Underwood then indulges in the subgroup analysis fallacy by asserting that a few people get a large benefit from acupuncture. Or perhaps a few people just happen to get better that day. I was not convinced.
More 4 News TV 20.20 was an interview, with the other side being put by my old friend, George Lewith.
During the introduction, an acupuncturist. Lisa Sherman, ‘explained’ acupuncture in the usual sort of utterly meaningless words that illustrate perfectly the problem.
George Lewith said that “we don’t have a good pretend form of acupuncture”. “We don’t have a good placebo and we can demonstrate that acupuncture is literally twice as effective as conventional care”. The first is simply nonsense: huge efforts have gone into developing good controls in acupuncture studies (see, for example, Barker Bausell’s book, Snake Oil Science). And I hope that George will send the references for his “twice as effective” claim. It seems to me to be nothing short of preposterous.
My conclusions
So what went wrong?
One problem could be regarded as medical arrogance. The fact is that the problem of low back pain has not been solved, either by drugs or anything else. It is a failure of medicine (and of pharmacology). That should be the premise of all discussions, and it smacks of arrogance not to tell people straight out. Of course there are some cases when causes can be identified, and perhaps remedied, usually by surgery, but these are the exceptions not the rule.
One consequence of the inability of medicine to help much is that patients get desperate, and willing to try anything. And of course if they happen to have a remission, that is attributed to the treatment, however preposterous that treatment may have been. Conditions like back pain that come and go unpredictable are a gift for quacks.
Another consequence, for researchers rather than patients, is to clutch at straws. Even small and inconsistent effects are seized on as ‘successes’. This phenomenon seems to be part of the reason for the NICE guidance. Another reason is, almost certainly, the grinding of axes by some of the people who wrote it.
What should be done now?
Professor Sir Michael Rawlins is a sensible chap. He cares about evidence, But it does seem that in this case, he might have taken his eye off the ball, for once. In my opinion, he should restore the reputation of NICE by withdrawing this guidance and starting again.
Follow-up
An interesting document has come my way. It shows the responses of the guidance group to the consultation on the draft guidance. Many people made comments not unlike mone, but they were all brushed aside in a way that looks to me rather partisan. The document appears to have vanished from NICE’s web site, but you can download it here.
Friday 29th May. The Times prints a letter from two consultants in pain medicine, Joan Hestor and Stephen Ward. It says, inter alia
“As experienced pain specialists we feel that NICE has lost its way in publishing these guidelines.”
“We are saddened that NICE has chosen to ignore our important role and promote seemingly unworkable and for the most part clinically ineffective treatments”
Friday 29th May. NICE has had a good reputation in the USA for its important, and usually high-quality, attempts to assess what works and what doesn’t. That makes it all the sadder to see it condemned already from the USA for its latest effort. The excellent Yale neurologist, Steven Novella, has written about it on his Neurologica blog.
Friday 29th May. A correspondent points out that the costings of the guidance can be found on the NICE web site. Table 1 has a strong air of make-believe.
The Daily Mail (29 May 2009). Their article quotes serious criticisms of NICE.
Dr Ron Cooper, past chairman of the group and a consultant pain specialist in Northern Ireland, said: ‘I have never known so many pain medicine specialists to be so furious. More patients will end up having more expensive surgery, which is unnecessary, risky and has worse results.
‘NICE made it difficult for us to submit evidence to a committee on which there was not one experienced pain physician.
‘The guidelines will make us the laughing stock of Europe, Australia and the U.S. where pain specialists will continue to have full access to a wide range of treatments.’
Chirowatch suspended. 30 May 2009. The invaluable chiro-watch site, http://www.chirowatch.com, run by Dr Canadian physician, Dr Tom Polevoy, has been “suspended”. In fact the whole of his domain, healthwatcher.net, has been disabled. It seems that this was the result of a legal threat to his ISP, not by chiropractors this time, but by William O’Neill of the Canadian Cancer Research Group, which is far from being what the respectable-sounding title suggests, according to Dr Stephen Barrett. The site will be back soon, I’m told. Meanwhile you can read the suspended page here, and the only result of their hamfisted bullying will be to vastly increase the number of people who read it. You can read lots more at Quackwatch’s chirobase and at ebm-first.
A new blog, Not as NICE as you think appeared on May 30th. It is written by a pain physician, Stephen Ward. and is devoted to pointing out the serious problems raised by NICE’s guidance. It starts with the (very critical) World Institute of Pain Press Release.
British Medical Journal has more flak for the NICE guidelines
And the BMJ has published a letter signed by 50 consultants in pain medicine, NICE guidelines on low back pain are flawed.(this will probably appear as a letter in the print edition of the BMJ).
First the MHRA lets down the public by allowing deceptive labelling of sugar pills (see here, and this this blog). Now it is the turn of NICE to betray its own principles.
The National Institute for Health and Clinical Excellence (NICE) describes its job thus
“NICE is an independent organisation responsible for providing national guidance on promoting good health and preventing and treating ill health.”
Its Guidance document on Low Back Pain will be published on Wednesday 27 May 2009, but the newspapers have already started to comment, presumably on the assumption that it will have changed little from the Draft Guidance of September 2008. These comments may have to be changed as soon as the final version becomes available.
The draft guidance, though mostly sensible, has two recommendations that I believe to be wrong and dangerous. The recommendations include (page 7) these three.
- Consider offering a course of manual therapy including spinal manipulation of up to 9 sessions over up to 12 weeks.
- Consider offering a course of acupuncture needling comprising up to 10 sessions over a period of up to 12 weeks.
- Consider offering a structured exercise programme tailored to the individual.
All three of this options are accompanied by a footnote that reads thus.
“A choice of any of these therapies may be offered, taking into account patient preference.”
On the face if it, this might seem quite reasonable. All three choices seem to be about as effective (or ineffective) as each other, so why not let patients choose between them?
Actually there are very good reasons, but NICE does not seem to have thought about them. In the past I have had a high opinion of NICE but it seems that even they are now getting bogged down in the morass of political correctness and officialdom that is the curse of the Department of Health. It is yet another example of DC’s rule number one.
Never trust anyone who uses the word ‘stakeholder’.
They do use it, often.
So what is so wrong?
For a start, I take it that the reference to “spinal manipulation” in the first recommendation is a rather cowardly allusion to chiropractic. Why not say so, if that’s whar you mean? Chiropractic is mentioned in the rest of the report but the word doesn’t seem to occur in the recommendations. Is NICE perhaps nervous that it would reduce the credibility of the report if the word chiropractic were said out loud?
Well, they have a point, I suppose. It would.
That aside, here’s what’s wrong.
The Evidence
I take as my premise that the evidence says that no manipulative therapy has any great advantage over the others. They are all more or less equally effective. Perhaps I should say, more or less equally ineffective, because anyone who claims to have the answer to low back pain is clearly deluded (and I should know: nobody has fixed mine yet). So for effectiveness there are no good grounds to choose between exercise, physiotherapy, acupuncture or chiropractic. There is, though, an enormous cultural difference. Acupuncture and chiropractic are firmly in the realm of alternative medicine. They both invoke all sorts of new-age nonsense for which there isn’t the slightest good evidence. That may not poison your body, but it certainly poisons your mind.
Acupuncturists talk about about “Qi”, “meridians”, “energy flows”. The fact that “sham” and “real” acupuncture consistently come out indistinguishable is surely all the evidence one needs to dismiss such nonsense. Indeed there is a small group of medical acupuncturists who do dismiss it. Most don’t. As always in irrational subjects, acupuncture is riven by internecine strife between groups who differ in the extent of their mystical tendencies,
Chiropractors talk of “subluxations”, an entirely imaginary phenomenon (but a cause of much unnecessary exposure to X-rays). Many talk of quasi-religious things like “innate energy”. And Chiropractic is even more riven by competing factions than acupuncture. See, for example, Chiropractic wars Part 3: internecine conflict.
The bait and switch trick
This is the basic trick used by ‘alternative therapists’ to gain respectability.
There is a superb essay on it by the excellent Yale neurologist Steven Novella: The Bait and Switch of Unscientific Medicine. The trick is to offer some limited and reasonable treatment (like back manipulation for low back pain). This, it seems, is sufficient to satisfy NICE. But then, once you are in the showroom, you can be exposed to all sorts of other nonsense about “subluxations” or “Qi”. Still worse, you will also be exposed to the claims of many chiropractors and acupuncturists to be able to cure all manner of conditions other than back pain. But don’t even dare to suggest that manipulation of the spine is not a cure for colic or asthma or you may find yourself sued for defamation. The shameful legal action of the British Chiropractic Association against Simon Singh (follow it here) led to an addition to DC’s Patients’ Guide to Magic Medicine.
(In the face of such tragic behaviour, one has to be able to laugh).
Libel: A very expensive remedy, to be used only when you have no evidence. Appeals to alternative practitioners because truth is irrelevant.
NICE seems to have fallen for the bait and switch trick, hook line and sinker.
The neglected consequences
Once again, we see the consequences of paying insufficient attention to the Dilemmas of Alternative Medicine.
The lying dilemma
If acupuncture is recommended we will have acupuncturists telling patients about utterly imaginary things like “Qi” and “meridians”. And we will have chiropractors telling them about subluxations and innate energy. It is my opinion that these things are simply make-believe (and that is also the view of a minority of acupuncturist and chiropractors). That means that you have to decide whether the supposed benefits of the manipulation are sufficient to counterbalance the deception of patients.
Some people might think that it was worth it (though not me). What is unforgivable is not to consider even the question. The NICE guidance says not a word about this dilemma. Why not?
The training dilemma
The training dilemma is even more serious. Once some form of alternative medicine has successfully worked the Bait and Switch trick and gained a toehold in the NHS, there will be an army of box-ticking HR zombies employed to ensure that they have been properly trained in “subluxations” or “Qi”. There will be quangos set up to issue National Occupational Standards in “subluxations” or “Qi”. Skills for Health will issue “competences” in “subluxations” or “Qi” (actually they already do). There will be courses set up to teach about “subluxations” or “Qi”, some even in ‘universities’ (there already are).
The respectability problem
But worst of all, it will become possible for aupuncturists and chiropractors to claim that they now have official government endorsement from a prestigious evidence-based organisation like NICE for “subluxations” or “Qi”. Of course this isn’t true. In fact the words “subluxations” or “Qi” are not even mentioned in the draft report. That is the root of the problem. They should have been. But omitting stuff like that is how the Bait and Switch trick works.
Alternative medicine advocates crave, above all, respectability and acceptance. It is sad that NICE seems to have given them more credibility and acceptance without having considered properly the secondary consequences of doing so,
How did this failure of NICE happen?
It seems to have been a combination of political correctness, failure to consider secondary consequences, and excessive influence of the people who stand to make money from the acceptance of alternative medicine.
Take, for example, the opinion of the British Pain Society. This organisation encompasses not just doctors. It
includes “doctors, nurses, physiotherapists, scientists, psychologists, occupational therapists and other healthcare professionals actively engaged in the diagnosis and treatment of pain and in pain research for the benefit of patients”. Nevertheless, their response to the draft guidelines pointed out that the manipulative therapies as a whole were over-represented.
|
Manipulation The guidelines assess 9 large groups of interventions of which manual therapies are only one part. The full GDG members panel of 13 individuals included two proponents of spinal manipulation/mobilisation (P Dixon and S Vogel). In addition, the chair of the panel (M Underwood) is the lead author of the UKBEAM trial on which the positive recommendation for |
It seems that the Pain Society were quite right.
LBC 97.3 Breakfast Show (25 May 2009) had a quick discussion on acupuncture (play mp3 file). After I had my say, the other side was put by Rosey Grandage. She has (among other jobs) a private acupuncture practice so she is not quite as unbiassed as me). As usual, she misrepresents the evidence by failing to distinguish between blind and non-blind studies. She also misrepresented what I said by implying that I was advocating drugs. That was not my point and I did not mention drugs (they, like all treatments, have pretty limited effectiveness, and they have side effects too). She said “there is very good evidence to show they (‘Qi’ and ‘meridians’] exist”. That is simply untrue.
There can’t be a better demonstration of the consequences of falling for bait and switch than the defence mounted by Rosey Grandage. NICE may not mention “Qi” and “meridians”; but the people they want to allow into the NHS have no such compunctions.
I first came across Rosey Grandage when I discovered her contribution to the Open University/BBC course K221. That has been dealt with elsewhere. A lot more information about acupuncture has appeared since then. She doesn’t seem to have noticed it. Has she not seen the Nordic Cochrane Centre report? Nor read Barker Bausell, or Singh & Ernst? Has she any interest in evidence that might reduce her income? Probably not.
Where to find out more
An excellent review of chiropractic can be found at the Layscience site. It was written by the indefatigable ‘Blue Wode’ who has provided enormous amounts of information at the admirable ebm-first site (I am authorised to reveal that ‘Blue Wode’ is the author of that site). There you will also find much fascinating information about both acupuncture and about chiropractic.
I’m grateful to ‘Blue Wode’ for some of the references used here.
Follow-up
| The Prince of Wales’ Foundation for Integrated Health (FiH) is a propaganda organisation that aims to persuade people, and politicians, that the Prince’s somewhat bizarre views about alternative medicine should form the basis of government health policy.
His attempts are often successful, but they are regarded by many people as being clearly unconstitutional. |
 |
The FiH’s 2009 AnnualConferen ce conference was held at The King’s Fund, London 13 – 14 May 2009. It was, as always, an almost totally one-sided affair devoted to misrepresentation of evidence and the promotion of magic medicine. But according to the FiH, at least, it was a great success. The opening speech by the Quacktitioner Royal can be read here. It has already been analysed by somebody who knows rather more about medicine than HRH. He concludes
“It is a shocking perversion of the real issues driven by one man; unelected, unqualified and utterly misguided”.
We are promised some movie clips of the meeting. They might even make a nice UK equivalent of “Integrative baloney @ Yale“.
This post is intended to provide some background information about the speakers at the symposium. But let’s start with what seems to me to be the real problem. The duplicitous use of the word “integrated” to mean two quite different things.
The problem of euphemisms: spin and obfuscation
One of the problems of meetings like this is the harm done by use of euphemisms. After looking at the programme, it becomes obvious that there is a rather ingenious bit of PR trickery going on. It confuses (purposely?) the many different definitions of the word “integrative” . One definition of “Integrative medicine” is this (my emphasis).
” . . . orienting the health care process to engage patients and caregivers in the full range of physical, psychological, social, preventive, and therapeutic factors known to be effective and necessary for the achievement of optimal health.”
That is a thoroughly admirable aim. And that, I imagine, is the sense in which several of the speakers (Marmot, Chantler etc) used the term. Of course the definition is rather too vague to be very helpful in practice, but nobody would dream of objecting to it.
But another definition of the same term ‘integrative medicine’ is as a PR-friendly synonym for ‘alternative medicine’, and that is clearly the sense in which it is used by the Prince of Wales’ Foundation for Integrated Health (FIH), as is immediately obvious from their web site.
The guide to the main therapies supports everything from homeopathy to chiropractic to naturopathy, in a totally uncritical way. Integrated service refers explicitly to integration of ‘complementary’ medicine, and that itself is largely a euphemism for alternative medicine. For example, the FIH’s guide to homeopathy says
“What is homeopathy commonly used for?
Homeopathy is most often used to treat chronic conditions such as asthma; eczema; arthritis; fatigue disorders like ME; headache and migraine; menstrual and menopausal problems; irritable bowel syndrome; Crohn’s disease; allergies; repeated ear, nose, throat and chest infections or urine infections; depression and anxiety.”
But there is not a word about the evidence, and perhaps that isn’t surprising because the evidence that it works in any of these conditions is essentially zero.
The FIH document Complementary Health Care: A Guide for Patients appears to have vanished from the web after its inaccuracy received a very bad press, e.g. in the Times, and also here. It is also interesting that the equally widely criticised Smallwood report (also sponsored by the Prince of Wales) seems to have vanished too).
The programme for the meeting can be seen here, for Day 1, and Day 2
Conference chair Dr Phil Hammond, GP, comedian and health service writer. Hammond asked the FIH if I could speak at the meeting to provide a bit of balance. Guess what? They didn’t want balance.
09:30 Opening session
Dr Michael Dixon OBE
09:30 Introduction: a new direction for The Prince’s Foundation for Integrated Health and new opportunities in integrated health and care. Dr Michael Dixon, Medical Director, FIH
Michael Dixon is devoted to just about every form of alternative medicine. As well as being medical director of the Prince’s Foundation he also runs the NHS Alliance. Despite its name, the NHS Alliance is nothing to do with the NHS and acts, among other things, as an advocate of alternative medicine on the NHS, about which it has published a lot.
Dr Dixon is also a GP at College Surgery, Cullompton, Devon, where his “integrated practice” includes dozens of alternative practitioners. They include not only disproven things like homeopathy and acupuncture, but also even more bizarre practitioners in ‘Thought Field Therapy‘ and ‘Frequencies of Brilliance‘.
To take only one of these, ‘Frequencies of Brilliance’ is bizarre beyond belief. One need only quote its founder and chief salesperson.
“Frequencies of Brilliance is a unique energy healing technique that involves the activation of energetic doorways on both the front and back of the body.”
“These doorways are opened through a series of light touches. This activation introduces high-level Frequencies into the emotional and physical bodies. It works within all the cells and with the entire nervous system which activates new areas of the brain.”
“Frequencies of Brilliance is a 4th /5th dimensional work. The process is that of activating doorways by lightly touching the body or working just above the body.”
“Each doorway holds the highest aspect of the human being and is complete in itself. This means that there is a perfect potential to be accessed and activated throughout the doorways in the body.”
Best of all, it can all be done at a distance (that must help sales a lot). One is reminded of the Skills for Health “competence” in distant healing (inserted on a government web site at the behest (you guessed it) of the Prince’s Foundation, as related here)
“The intent of a long distance Frequencies of Brilliance (FOB) session is to enable a practitioner to facilitate a session in one geographical location while the client is in another.
A practitioner of FOB that has successfully completed a Stage 5 Frequency workshop has the ability to create and hold a stable energetic space in order to work with a person that is not physically present in the same room.
The space that is consciously created in the Frequencies of Brilliance work is known as the “Gap”. It is a space of nonlinear time. It contains ”no time and no space” or respectively “all time and all space”. Within this “Gap” a clear transfer of the energies takes place and is transmitted to an individual at a time and location consciously intended. Since this dimensional space is in non-linear time the work can be performed and sent backward or forward in time as well as to any location.
The Frequencies of Brilliance work cuts through the limitations of our physical existence and allows us to experience ourselves in other dimensional spaces. Therefore people living in other geographic locations than a practitioner have an opportunity to receive and experience the work.
The awareness of this dimensional space is spoken about in many indigenous traditions, meditation practices, and in the world of quantum physics. It is referred to by other names such as the void, or vacuum space, etc.”
This is, of course, preposterous gobbledygook. It, and other things in Dr Dixon’s treatment guide, seem to be very curious things to impose on patients in the 21st century.
Latest news. The Mid-Devon Star announces yet more homeopathy in Dr Dixon’s Cullompton practice. This time it comes in the form of a clinic run from the Bristol Homeopathic Hospital. I guess they must be suffering from reduced commissioning like all the other homeopathic hospitals, but Dr Dixon seems to have come to their rescue. The connection seems to be with Bristol’s homeopathic consultant, Dr Elizabeth A Thompson. On 11 December 2007 I wrote to Dr Thompson, thus
|
In March 2006, a press release http://www.ubht.nhs.uk/press/view.asp?257 announced a randomised trial for homeopathic treatment of asthma in children. This was reported also on the BBC http://news.bbc.co.uk/1/hi/england/bristol/4971050.stm . I’d be very grateful if you could let me know when results from this trial will become available. Yours sincerely David Colquhoun |
The reply, dated 11 December 2007, was unsympathetic
|
I have just submitted the funders report today and we have set ourselves the deadline to publish two inter-related papers by March 1st 2007. Can I ask why you are asking and what authority you have to gain this information. I shall expect a reply to my questions, |
I answered this question politely on the same day but nevertheless my innocent enquiry drew forth a rather vitriolic complaint from Dr Thompson to the Provost of UCL (dated 14 December 2007). In this case, the Provost came up trumps. On 14 January 2008 he replied to Thompson: “I have looked at the email that you copied to me, and I must say that it seems an entirely proper and reasonable request. It is not clear to me why Professor Colquhoun should require some special authority to make such direct enquiries”. Dr Thompson seems to be very sensitive. We have yet to see the results of her trial in which I’m still interested.
Not surprisingly, Dr Dixon has had some severe criticism for his views, not least from the UK’s foremost expert on the evidence for efficacy, Prof Edzard Ernst. Accounts of this can be found in Pulse,
and on Andrew Lewis’s blog.
Dixon is now (in)famous in the USA too. The excellent Yale neurologist, Steven Novella, has written an analysis of his views on Science Based Medicine. He describes Dr. Michael Dixon as “A Pyromaniac In a Field of (Integrative) Straw Men”
Peter Hain
09:40 Politics and people: can integrated health and care take centre stage in 2009/2010? Rt Hon Peter Hain MP
It seems that Peter Hain was converted to alternative medicine when his first baby, Sam, was born with eczema. After (though possibly not because of) homeopathic treatment and a change in diet, the eczema got better. This caused Hain, while Northern Ireland Secretary to spend £200,000 of taxpayers’ money to set up a totally uninformative customer satisfaction survey, which is being touted elsewhere in this meeting as though it were evidence (see below). I have written about this episode before: see Peter Hain and Get Well UK: pseudoscience and privatisation in Northern Ireland.
I find it very sad that a hero of my youth (for his work in the anti-apartheid movement) should have sunk to promoting junk science, and even sadder that he does so at my expense.
There has been a report on Hain’s contribution in Wales Online.
09:55 Why does the Health Service need a new perspective on health and healing? Sir Cyril Chantler, Chair, King’s Fund, previous Dean, Guy’s Hospital and Great Ormond Street
Cyril Chantler is a distinguished medical administrator. He also likes to talk and we have discussed the quackery problem several times. He kindly sent me the slides that he used. Slide 18 says that in order to do some good we “need to demonstrate that the treatment is clinically effective and cost effective for NHS use”. That’s impeccable, but throughout the rest of the slides he talks of integrating with complementary” therapies, the effectiveness of which is either already disproved or simply not known.
I remain utterly baffled by the reluctance of some quite sensible people to grasp the nettle of deciding what works. Chantler fails to grasp the nettle, as does the Department of Health. Until they do so, I don’t see how they can be taken seriously.
10.05 Panel discussion
The Awards
10:20 Integrated Health Awards 2009 Introduction: a review of the short-listed applications
10:45 Presentations to the Award winners by the special guest speaker
11:00 Keynote address by special guest speaker
Getting integrated
Dr David Peters
12:00 Integration, long term disease and creating a sustainable NHS. Professor David Peters, Clinical Director and Professor of Integrated Healthcare, University of Westminster
I first met David Peters after Nature ran my article, Science Degrees without the Science. .One of the many media follow-ups of that article was on Material World (BBC Radio 4). This excellent science programme, presented by Quentin Cooper, had a discussion between me and David Peters ( listen to the mp3 file).
There was helpful intervention from Michael Marmot who had talked, in the first half of the programme, about his longitudinal population studies.
Marmot stressed the need for proper testing. In the case of
homeopathy and acupuncture, that proper testing has largely been done. The tests were failed.
The University of Westminster has, of course, gained considerable notoriety as the university that runs more degree programmes in anti-scientific forms of medicine than any other. Their lecture on vibrational medicine teaches students that amethysts “emit high Yin energy so transmuting lower energies and clearing and aligning energy disturbances at all levels of being”. So far their vice-chancellor, Professor Geoffrey Petts, has declined to answer enquiries about whether he thinks such gobbledygook is appropriate for a BSc degree.
But he did set up an internal enquiry into the future of their alternative activities. Sadly that enquiry seems to have come to the nonsensical conclusion that the problem can be solved by injection of good science into the courses, as reported here and in the Guardian.
It seems obvious that if you inject good science into their BSc in homeopathy the subject will simply vanish in a puff of smoke.
In 2007, the University of Westminster did respond to earlier criticism in Times Higher Education, but their response seemed to me to serve only to dig themselves deeper into a hole.
Nevertheless, Westminster has now closed down its homeopathy degree (the last in the country to go) and there is intense internal discussion going on there. I have the impression that Dr Peters’ job is in danger. The revelation of more slides from their courses on homeopathy, naturopathy and Chinese herbal medicine shows that these courses are not only barmy, but also sometimes dangerous.
Professor Chris Fowler
12:10 Educating tomorrow’s integrated doctors. Professor Chris Fowler, Dean for Education, Barts and The London School of Medicine and Dentistry
I first came across Dr Fowler when I noticed him being praised for his teaching of alternative medicine to students at Barts and the London Medical School on the web site of the Prince’s Foundation. I wrote him a polite letter to ask if he really thought that the Prince of Wales was the right person to consult about the education of medical students. The response I got was, ahem, unsympathetic. But a little while later I noticed that two different Barts students had set up public blogs that criticised strongly the nonsense that was being inflicted on them.
At that point, I felt it was necessary to support the students who, it seemed to me, knew more about medical education than Professor Fowler. It didn’t take long to uncover the nonsense that was being inflicted on the students: read about it here.
There is a follow-up to this story here. Fortunately, Barts’ Director of Research, and, I’m told, the Warden of Barts, appear to agree with my view of the harm that this sort of thing can do to the reputation of Barts, so things may change soon,
Dame Donna Kinnair
12:30 Educating tomorrow’s integrated nurses.
Dame Donna Kinnair, Director of Nursing, Southwark PCT
As far as I can see, Donna Kinnair has no interest in alternative medicine. She is director of nursing at Southwark primary care trust and was an adviser to Lord Laming throughout his inquiry into the death of Victoria Climbié. I suspect that her interest is in integrating child care services (they need it, judging by the recent death of ‘Baby P’). Perhaps her presence shows the danger of using euphemisms like ‘integrated medicine’ when what you really mean is the introduction of unproven or disproved forms of medicine.
Michael Dooley
12:40 Integrating the care of women: an example of the new paradigm. Michael Dooley, Consultant Obstetrician and Gynecologist
DC’s rule 2. Never trust anyone who uses the word ‘paradigm’. It is a sure-fire sign of pseudoscience. In this case, the ‘new paradigm’ seems to be the introduction of disproven treatment. Dooley is a gynaecologist and Medical Director of the Poundbury Clinic. His clinic offers a whole range of unproven and disproved treatments. These include acupuncture as an aid to conception in IVF. This is not recommended by the Cochrane review, and one report suggests that it hinders conception rather than helps.
12.40 Discussion
13.00 – 14.00 Lunch and Exhibition
15.30 Tea
Boo Armstrong and Get Well UK
16.00 Integrated services in action: The Northern
Ireland experience: what has it shown us and what are its implications?
Boo Armstrong of Get Well UK with a team from the NI study
I expect that much will be made of this “study”, which, of course, tells you absolutely nothing whatsoever about the effectiveness of the alternative treatments that were used in it. This does not appear to be the view of Boo Armstrong, On the basis of the “study”, her company’s web site proclaims boldly
“Complementary Medicine Works
Get Well UK ran the first government-backed complementary therapy project in the UK, from February 2007 to February 2008″
This claim appears, prima facie, to breach the Unfair Trading Regulations of May 2008. The legality of the claim is, at the moment, being judged by a Trading Standards Officer. In any case, the “study” was not backed by the government as a whole, but just by Peter Hain’s office. It is not even clear that it had ethical approval.
The study consisted merely of asking people who had seen an alternative medicine practitioner whether they felt better or worse. There was no control group; no sort of comparison was made. It is surely obvious to the most naive person that a study like this cannot even tell you if the treatment has a placebo effect, never mind that it has any genuine effects of its own. To claim that it does so seems to be simply dishonest. There is no reason at all to think that the patients would not have got better anyway.
It is not only Get Well UK who misrepresent the evidence. The Prince’s
Foundation itself says
“Now a new, year long trial supported by the Northern Ireland health service has . . . demonstrated that integrating complementary and conventional medicine brings measurable benefits to patients’ health.”
That is simply not true. It is either dishonest or stupid. Don’t ask me which, I have no idea.
This study is no more informative than the infamous Spence (2005) ‘study’ of the same type, which seems to be the only thing that homeopaths can produce to support their case.
There is an excellent analysis of the Northern Ireland ‘study’ by Andy Lewis, The Northern Ireland NHS Alternative Medicine ‘Trial’. He explains patiently, yet again, what constitutes evidence and why studies like this are useless.
His analogy starts
” . . . the Apple Marketing Board approach the NHS and ask for £200,000 to do a study to show the truth behind the statement ‘An apple a day keeps the doctor away’. The Minister, being particularly fond of apples, agrees and the study begins.”
16.30 Social enterprise and whole systems integrated care. Dee Kyne, Sandwell PCT and a GP. Developing an integrated service in secondary care
Dee Kyne appears to be CEO of KeepmWell Ltd (a financial interest that is not mentioned).
Peter Mackereth, Clinical Lead, Supportive Services, Christie Hospital NHS Foundation Trust
I had some correspondence with Mackereth when the Times (7 Feb 2007) published a picture of the Prince of Wales inspecting an “anti-MRSA aromatherapy inhaler” in his department at the Christie. It turned out that the trial they were doing was not blind No result has been announced anyway, and on enquiry, I find that the trial has not even started yet. Surprising, then to find that the FIH is running the First Clinical Aromatherapy Conference at the Christie Hospital, What will there be to talk about?
Much of what they do at the Christie is straightforward massage, but they also promote the nonsensical principles of “reflexology” and acupuncture.
The former is untested. The latter is disproven.
Parallel Sessions
Developing a PCT funded musculoskeletal service Dr Roy Welford, Glastonbury Health Centre
Roy Welford is a Fellow of the Faculty of Homeopathy, and so promotes disproven therapies. The Glastonbury practice also advertises acupuncture (disproven), osteopathy and herbal medicine (largely untested so most of it consists of giving patients an unknown dose of an ill-defined drug, of unknown effectiveness and unknown safety).
Making the best of herbal self-prescription in integrated practice: key remedies and principles. Simon Mills, Project Lead: Integrated Self Care in Family Practice, Culm Valley Integrated Centre for Health, Devon
Simon Mills is a herbalist who now describes himself as a “phytotherapist” (it sounds posher, but the evidence, or lack of it, is not changed by the fancy name). Mills likes to say things like “there are herbs for heating and drying”, “hot and cold” remedies, and to use meaningless terms like “blood cleanser”, but he appears to be immune to the need for good evidence that herbs work before you give them to sick people. He says, at the end of a talk, “The hot and the cold remain the trade secret of traditional medicine”. And this is the 21st Century.
Practical ways in which complementary approaches can improve the treatment of cancer. Professor Jane Plant, Author of “Your life in your hands” and Chief Scientist, British Geological Society and Professor Karol Sikora, Medical Director, Cancer Partners UK
Jane Plant is a geologist who, through her own unfortunate encounter with breast cancer, became obsessed with the idea that a dairy-free diet cured her. Sadly there is no good evidence for that idea, according to the World Cancer Research Fund Report, led by Professor Sir Michael Marmot. No doubt her book on the subject sells well, but it could be held that it is irresponsible to hold out false hopes to desperate people. She is a supporter of the very dubious CancerActive organisation (also supported by Michael Dixon OBE –see above) as well as the notorious pill salesman, Patrick Holford (see also here).
Karol Sikora, formerly an oncologist at the Hammersmith Hospital, is now Dean of Medicine at the University of Buckingham (the UK’s only private university). He is also medical director at CancerPartners UK, a private cancer company.
He recently shot to fame when he appeared in a commercial in the USA sponsored by “Conservatives for Patients’ Rights”, to pour scorn on the NHS, and to act as an advocate for the USA’s present health system. A very curious performance. Very curious indeed.
His attitude to quackery is a mystery wrapped in an enigma. One was somewhat alarmed to see him sponsoring a course at what was, at first, called the British College of Integrated Medicine, and has now been renamed the Faculty of Integrated Medicine That grand title makes it sound like part of a university. It isn’t.

The alarm was as result of the alliance with Dr Rosy Daniel (who promotes an untested herbal conconction, Carctol, for ‘healing’ cancer) and Dr Mark Atkinson (a supplement salesman who has also promoted the Qlink pendant. The Qlink pendant is a simple and obvious fraud designed to exploit paranoia about WiFi killing you.
The first list of speakers on the proposed diploma in Integrated Medicine was an unholy alliance of outright quacks and commercial interests. It turned out that, although Karol Sikora is sponsoring the course, he knew nothing about the speakers. I did and when I pointed this out to Terence Kealey, vice-chancellor of Buckingham, he immediately removed Rosy Daniel from directing the Diploma. At the moment the course is being revamped entirely by Andrew Miles. There is hope that he’ll do a better job. It has not yet been validated by the University of Buckingham. Watch this space for developments.
Stop press It is reported in the Guardian that Professor Sikora has been describing his previous job at Imperial College with less than perfect accuracy. Oh dear. More developments in the follow-up.
The role of happy chickens in healing: farms as producers of health as well as food – the Care Farm Initiative Jonathan Dover, Project Manager, Care Farming, West Midlands.
“Care farming is a partnership between farmers, participants and health & social care providers. It combines the care of the land with the care of people, reconnecting people with nature and their communities.”
Sounds lovely, I wonder how well it works?
What can the Brits learn from the Yanks when it comes to integrated health? Jack Lord, Chief Executive Humana Europe
It is worth noticing that the advisory board of Humana Europe includes Micheal Dixon OBE, a well known advocate of alternative medicine (see
above). Humana Europe is a private company, a wholly owned subsidiary of Humana Inc., a health benefits company with 11 million members and 22,000 employees and headquarters in Louisville, Kentucky. In 2005 it entered into a business partnership with Virgin Group. Humana was mentioned in the BBC Panorama programme “NHS for Sale”. The company later asked that it be pointed out that they provide commissioning services, not clinical services [Ed. well not yet anyway].
Humana’s document “Humana uses computer games to help people lead healthier lives” is decidedly bizarre. Hang on, it was only a moment ago that we were being told that computer games rewired your brain.
Day 2 Integrated health in action
09.00 Health, epidemics and the search for new solutions. Sir Michael Marmot, Professor of Epidemiology and Public Health, Royal Free and University College Medical School
It is a mystery to me that a distinguished epidemiologist should be willing to keep such dubious company. Sadly I don’t know what he said, but judging my his publications and his appearence on Natural World, I can’t imagine he’d have much time for homeopaths.
9.25 Improving health in the workplace. Dame Carol Black, National Director, Health and Work, Department of Health
This is not the first time that Dame Carol has been comtroversial.
9.45 Integrated health in focus: defeating obesity. Professor Chris Drinkwater, President, NHS Alliance.
The NHS Alliance was mentioned above. Enough said.
10.00 Integrated healthcare in focus: new approaches to managing asthma, eczema and allergy. Professor Stephen Holgate, Professor of Immunopharmacology, University of Southampton
10.15 Using the natural environment to increase activity. The Natural England Project: the results from year one. Dr William Bird and Ruth Tucker, Natural England.
10.30 Panel discussion
10.45 Coffee
Self help in action
11.10 Your health, your way: supporting self care through care planning and the use of personal budgets. Angela Hawley, Self Care Lead, Department of Health
11.25 NHS Life Check: providing the signposts to
integrated health. Roy Lambley, Project Director, NHS LifeCheck Programme
This programme was developed with the University of Westminster’s “Health and Well-being Network”. This group, with one exception, is separate from Westminster’s extensive alternative medicine branch (it’s mostly psychologists).
11.45 The agony and the ecstasy of helping patients to help themselves: tips for clinicians, practices and PCTs. Professor
Ruth Chambers, FIH Foundation Fellow.
11.55 Providing self help in practice: Department of Health Integrated Self Help Information Project. Simon Mills, Project Lead: Integrated Self Care in Family Practice, Culm Valley Integrated Centre for Health, Devon and Dr Sam Everington, GP, Bromley by Bow.
The Culm Valley Integrated Centre for health is part of the College Surgery Partnership, associated with Michael Dixon OBE (yes, again!).
Simon Mills is the herbalist who says “The hot and the cold remain the trade secret of traditional medicine” .
Sam Everington, in contrast, seems to be interested in ‘integration’ in the real sense of the word, rather than quackery.
Integrated health in action
How to make sense of the evidence on complementary approaches: what works? What might work? What doesn’t work?
Dr Hugh MacPherson, Senior Research Fellow in Health Sciences, York University and Dr Catherine Zollman, Bravewell Fellow
Hugh MacPherson‘s main interest is in acupuncture and he publishes in alternative medicine journals. Since the recent analysis in the BMJ from the Nordic Cochrane Centre (Madsen et al., 2009) it seems that acupuncture is finally dead. Even its placebo effect is too small to be useful. Catherine Zollman is a Bristol GP who is into homeopathy as well as acupuncture. She is closely connected with the Prince’s Foundation via the Bravewell Fellowship. That fellowship is funded by the Bravewell Collaboration, which is run by Christie Mack, wife of John Mack (‘Mack the Knife’), head of Morgan Stanley (amazingly, they still seem to have money). This is the group which, by sheer wealth, has persuaded so many otherwise respectable US universities to embrace every sort of quackery (see, for example, Integrative baloney @ Yale)
The funding of integrated services
14.15 How to get a PCT or practice- based commissioner to fund your integrated service. A PCT Chief Executive and a Practice-Based Commissioning lead.
14.30 How I succeeded: funding an integrated service. Dr John Ribchester, Whitstable
14.45 How we created an acupuncture service in St Albans and Harpenden PBC group. Mo Girach, Chief Executive, STAHCOM
Uhuh Acupunture again. Have these people never read Bausell’s
book? Have they not read the BMJ? Acupuncture is now ell-established to be based on fraudulent principles, and not even to have a worthwhile placeobo effect. STAHCOM seem to be more interested in money than in what works.
Dragon’s Den. Four pitchers lay out their stall for the commissioning dragons
And at this stage there is no prize for guessing that all four are devoted to trying to get funds for discredited treatments
- An acupuncture service for long-term pain. Mike Cummings Chair, Medical Acupuncture Association
- Manipulation for the treatment of back pain Simon Fielding, Founder Chairman of the General Osteopathic Council
- Nigel Clarke, Senior Partner, Learned Lion Partners Homeopathy for long term conditions
- Peter Fisher, Director, Royal Homeopathic Hospital
Sadly it is not stated who the dragons are. One hopes they will be more interested in evidence than the supplicants.
Mike Cummings at least doesn’t believe the nonsense about meridians and Qi. It’s a pity he doesn’t look at the real evidence though.
You can read something about him and his journal at BMJ Group promotes acupuncture: pure greed.
Osteopathy sounds a bit more respectable than the others, but in fact it has never shaken off its cult-like origins. Still many osteopaths make absurd claims to cure all sorts of diseases. Offshoots of osteopathy like ‘cranial osteopathy’ are obvious nonsense. There is no reason to think that osteopathy is any better than any other manipulative therapy and it is clear that all manipulative therapies should be grouped into one.
Osteopathy and chiropractic provide the best ever examples of the folly of giving official government recognition to a branch of alternative medicine before the evidence is in.
Learned Lion Partners is a new one on me. It seems it is
part of Madsen Gornall Ashe Chambers (‘MGA Chambers’) “a grouping of top level, independent specialists who provide a broad range of management consultancy advice to the marketing community”. It’s a management consultant and marketing outfit. So don’t expect too much when it comes to truth and evidence. The company web site says nothing about alternative medicine, but only that Nigel Clarke
“. . . has very wide experience of public affairs issues and campaigns, having worked with clients in many sectors in Europe, North America and the Far East. He has particular expertise in financial, competition and healthcare issues. “
However, all is revealed when we see that he is a Trustee of the Prince’s Foundation where his entry says
“Nigel Clarke is senior partner of Learned Lion Partners. He is a director of Vidapulse Ltd, Really Easy Ltd, Newscounter Ltd and Advanced Transport Systems Ltd. He has worked on the interfaces of public policy for 25 years. He has been chair of the General Osteopathic Council since May 2001, having been a lay member since it was formed. He is now a member of the Council for Healthcare Regulatory Excellence”
The Council for Healthcare Regulatory Excellence is yet another quango that ticks boxes and fails absolutely to grasp the one important point, does it work?. I came across them at the Westminster Forum, and they seemed a pretty pathetic way to spend £2m per year.
Peter Fisher is the last supplicant to the Dragons. He is clinical director of the Royal London Homeopathic Hospital (RLHH), and Queen’s homeopathic physician, It was through him that I got an active interest in quackery. The TV programme QED asked me to check the statistics in a paper of his that claimed that homeopathy was good for fibrositis (there was an elementary mistake and no evidence for an effect). Peter Fisher is also remarkable because he agreed with me that BSc degrees in homeopathy were not justified (on TV –see the movie). And he condemned homeopaths who were caught out recommending their sugar pills for malaria. To that extent Fisher represents the saner end of the homeopathic spectrum. Nevertheless he still maintains that sugar pills work and have effects of their own, and tries to justify the ‘memory of water’ by making analogies with a memory stick or CD. This is so obviously silly that no more comment is needed.
Given Fisher’s sensible condemnation of the malaria fiasco, I was rather surprised to see that he appeared on the programme of a conference at the University of Middlesex, talking about “A Strategy To Research The Potential Of Homeopathy In Pandemic Flu”. The title of the conference was Developing Research Strategies in CAM. A colleague, after seeing the programme, thought it was more like “a right tossers’ ball”.
Much of the homeopathy has now vanished from the RLHH as a result of greatly reduced commissioning by PCTs (read about it in Fisher’s own words). And the last homeopathy degree in the UK has closed down. It seems an odd moment for the FIH to be pushing it so hard.
Follow-up
Stop press It is reported in the Guardian (22 May 2009) that Professor Sikora has been describing his previous job at Imperial College with less than perfect accuracy. Oh dear, oh dear.
This fascinating fact seems to have been unearthed first by the admirable NHS Blog Doctor, in his post ‘Imperial College confirm that Karol Sikora does not work for them and does not speak on their behalf‘.
| One of the most extraordinary bits of journalism I’ve read for a long time appeared as an editorial in the Sri Lankan newspaper, the Sunday Leader, on Sunday January 11th 2009 It was reproduced in the Guardian on 13th January, and in The Times. It was written by Lasantha Wickrematunge, editor of the Sunday Leader, and it was the last thing he wrote. Days after writing it he was assassinated. |  |
It is a plea for freedom of speech. In particular, for the freedom of journalists to tell the truth, It is deeply moving and it is also written in more beautiful English than many native speakers can manage. The second person to leave a comment in the Guardian said
“Extraordinary, humbling and deeply moving.
Cif Eds, please leave this at the top of the page for about a week, and then nail copies it to every available surface at Guardian HQ.”
Writing blogs like this one (and a thousand others) need some of the skills of investigative journalism. Those skills are not so different from those you need in science, Curiosity, a willingness to look under stones, a preference for truth over myth, some skill with Google and a good deal of tenacity. You also need to be resilient to abuse and defamation by people who disagree with you. But you do not risk your life. It does not take much courage. That isn’t true in large parts of the world.
Read it all. Here are a few quotations to persuade you it’s worth the time.
“No other profession calls on its practitioners to lay down their lives for their art save the armed forces – and, in Sri
Lanka , journalism. In the course of the last few years, the independent media have increasingly come under attack. Electronic and print institutions have been burned, bombed, sealed and coerced. Countless journalists have been harassed, threatened and killed. It has been my honour to belong to all those categories, and now especially the last.”“The Sunday Leader has been a controversial newspaper because we say it like we see it: whether it be a spade, a thief or a murderer, we call it by that name. We do not hide behind euphemism. The investigative articles we print
are supported by documentary evidence thanks to the public-spiritedness of citizens who at great risk to themselves pass on this material to us. We have exposed scandal after scandal, and never once in these 15 years has anyone proved us wrong or successfully prosecuted us.”“The free media serve as a mirror in which the public can see itself sans mascara and styling gel. From us you learn the state of your nation, and especially its management by the people you elected to give your children a better future.”
“It is well known that I was on two occasions brutally assaulted, while on another my house was sprayed with machine-gun fire. Despite the government’s sanctimonious assurances, there was never a serious police inquiry into the perpetrators of these attacks, and the attackers were never apprehended.
In all these cases, I have reason to believe the attacks were inspired by the government. When finally I am killed, it will be the government that kills me.”
“In the wake of my death I know you will make all the usual sanctimonious noises and call upon the police to hold a swift and thorough inquiry.
But like all the inquiries you have ordered in the past, nothing will come of this one, too. For truth be told, we both know who will be behind my death, but dare not call his name. Not just my life but yours too depends on it.
As for me, I have the satisfaction of knowing that I walked tall and bowed to no man. And I have not travelled this journey alone. Fellow journalists in other branches of the media walked with me: most are now dead, imprisoned
without trial or exiled in far-off lands.”“People often ask me why I take such risks and tell me it is a matter of time before I am bumped off. Of course I know that: it is inevitable. But if we do not speak out now, there will be no one left to speak for those who cannot,
whether they be ethnic minorities, the disadvantaged or the persecuted. An example that has inspired me throughout my career in journalism has been that of the German theologian, Martin Niemöller. In his youth he was an antisemite and an admirer of Hitler. As nazism took hold of Germany, however, he saw nazism for what it was. It was not just the Jews Hitler sought to extirpate, it was just about anyone with an alternate point of view. Niemöller spoke out, and for his trouble was incarcerated in the Sachsenhausen and Dachau concentration camps from 1937 to 1945, and very nearly executed. While incarcerated, he wrote a poem that, from the first time I read it in my teenage years, stuck hauntingly in my mind:
First they came for the Jews
and I did not speak out because I was not a Jew.Then they came for the Communists
and I did not speak out because I was not a Communist.Then they came for the trade unionists
and I did not speak out because I was not a trade unionist.Then they came for me and there was no one left to speak out for me.
If you remember nothing else, let it be this: the Leader is there for you, be you Sinhalese, Tamil, Muslim, low-caste, homosexual, dissident or disabled.”
This man puts to shame the those who won’t speak out in the safety of the West, despite the fact that they have nothing to lose but their ministerial jobs or their knighthoods. Or running the risk of being sued by chiropractors.
How about some nominations for Western journalists who live up to these ideals? I’d start with Seymour Hersh and Paul Krugman in the USA, and our own Ben Goldacre. It’s interesting though, that two of these three are not full time journalists. Blogs do rather better than most newspapers. They have become an important force for freedom of speech. That more than counterbalances the use of the web for promoting junk. It is a lot harder to keep a secret than it used to be.
There is an obituary of Lasantha Wickrematunge in the Sunday Leader, and a report from Amnesty International.
I’m perfectly happy to think of alternative medicine as being a voluntary, self-imposed tax on the gullible (to paraphrase Goldacre again). But only as long as its practitioners do no harm and only as long as they obey the law of the land. Only too often, though, they do neither.
When I talk about law, I don’t mean lawsuits for defamation. Defamation suits are what homeopaths and chiropractors like to use to silence critics. heaven knows, I’ve becomes accustomed to being defamed by people who are, in my view. fraudsters, but lawsuits are not the way to deal with it.
I’m talking about the Trading Standards laws Everyone has to obey them, and in May 2008 the law changed in a way that puts the whole health fraud industry in jeopardy.
The gist of the matter is that it is now illegal to claim that a product will benefit your health if you can’t produce evidence to justify the claim.
I’m not a lawyer, but with the help of two lawyers and a trading standards officer I’ve attempted a summary. The machinery for enforcing the law does not yet work well, but when it does, there should be some very interesting cases.
The obvious targets are homeopaths who claim to cure malaria and AIDS, and traditional Chinese Medicine people who claim to cure cancer.
But there are some less obvious targets for prosecution too. Here is a selection of possibilities to savour..
- Universities such as Westminster, Central Lancashire and the rest, which promote the spreading of false health claims
- Hospitals, like the Royal London Homeopathic Hospital, that treat patients with mistletoe and marigold paste. Can they produce any real evidence that they work?
- Edexcel, which sets examinations in alternative medicine (and charges for them)
- Ofsted and the QCA which validate these exams
- Skills for Health and a whole maze of other unelected and unaccountable quangos which offer “national occupational standards” in everything from distant healing to hot stone therapy, thereby giving official sanction to all manner of treatments for which no plausible evidence can be offered.
- The Prince of Wales Foundation for Integrated Health, which notoriously offers health advice for which it cannot produce good evidence
- Perhaps even the Department of Health itself, which notoriously referred to “psychic surgery” as a profession, and which has consistently refused to refer dubious therapies to NICE for assessment.
The law, insofar as I’ve understood it, is probably such that only the first three or four of these have sufficient commercial elements for there to be any chance of a successful prosecution. That is something that will eventually have to be argued in court.
But lecanardnoir points out in his comment below that The Prince of Wales is intending to sell herbal concoctions, so perhaps he could end up in court too.
The laws
We are talking about The Consumer Protection from Unfair Trading Regulations 2008. The regulations came into force on 26 May 2008. The full regulations can be seen here, or download pdf file. They can be seen also on the UK Statute Law Database.
The Office of Fair Trading, and Department for Business, Enterprise & Regulatory Reform (BERR) published Guidance on the Consumer Protection from Unfair Trading Regulations 2008 (pdf file),
Statement of consumer protection enforcement principles (pdf file), and
The Consumer Protection from Unfair Trading Regulations: a basic guide for business (pdf file).
Has The UK Quietly Outlawed “Alternative” Medicine?
On 26 September 2008, Mondaq Business Briefing published this article by a Glasgow lawyer, Douglas McLachlan. (Oddly enough, this article was reproduced on the National Center for Homeopathy web site.)
“Proponents of the myriad of forms of alternative medicine argue that it is in some way “outside science” or that “science doesn’t understand why it works”. Critical thinking scientists disagree. The best available scientific data shows that alternative medicine simply doesn’t work, they say: studies repeatedly show that the effect of some of these alternative medical therapies is indistinguishable from the well documented, but very strange “placebo effect” ”
“Enter The Consumer Protection from Unfair Trading Regulations 2008(the “Regulations”). The Regulations came into force on 26 May 2008 to surprisingly little fanfare, despite the fact they represent the most extensive modernisation and simplification of the consumer protection framework for 20 years.”
The Regulations prohibit unfair commercial practices between traders and consumers through five prohibitions:-
- General Prohibition on Unfair Commercial
Practices (Regulation 3)- Prohibition on Misleading Actions (Regulations 5)
- Prohibition on Misleading Omissions (Regulation 6)
- Prohibition on Aggressive Commercial Practices (Regulation 7)
- Prohibition on 31 Specific Commercial Practices that are in all Circumstances Unfair (Schedule 1). One of the 31 commercial practices which are in all circumstances considered unfair is “falsely claiming that a product is able to cure illnesses, dysfunction or malformations”. The definition of “product” in the Regulations includes services, so it does appear that all forms medical products and treatments will be covered.
Just look at that!
| One of the 31 commercial practices which are in all circumstances considered unfair is “falsely claiming that a product is able to cure illnesses, dysfunction or malformations” |
Section 5 is equally powerful, and also does not contain the contentious word “cure” (see note below)
Misleading actions
5.—(1) A commercial practice is a misleading action if it satisfies the conditions in either paragraph (2) or paragraph (3).
(2) A commercial practice satisfies the conditions of this paragraph—
(a) if it contains false information and is therefore untruthful in relation to any of the matters in paragraph (4) or if it or its overall presentation in any way deceives or is likely to deceive the average consumer in relation to any of the matters in that paragraph, even if the information is factually correct; and
(b) it causes or is likely to cause the average consumer to take a transactional decision he would not have taken otherwise.
These laws are very powerful in principle, But there are two complications in practice.
One complication concerns the extent to which the onus has been moved on to the seller to prove the claims are true, rather than the accuser having to prove they are false. That is a lot more favourable to the accuser than before, but it’s complicated.
The other complication concerns enforcement of the new laws, and at the moment that is bad.
Who has to prove what?
That is still not entirely clear. McLachlan says
“If we accept that mainstream evidence based medicine is in some way accepted by mainstream science, and alternative medicine bears the “alternative” qualifier simply because it is not supported by mainstream science, then where does that leave a trader who seeks to refute any allegation that his claim is false?
Of course it is always open to the trader to show that his the alternative therapy actually works, but the weight of scientific evidence is likely to be against him.”
On the other hand, I’m advised by a Trading Standards Officer that “He doesn’t have to refute anything! The prosecution have to prove the claims are false”. This has been confirmed by another Trading Standards Officer who said
“It is not clear (though it seems to be) what difference is implied between “cure” and “treat”, or what evidence is required to demonstrate that such a cure is false “beyond reasonable doubt” in court. The regulations do not provide that the maker of claims must show that the claims are true, or set a standard indicating how such a proof may be shown.”
The main defence against prosecution seems to be the “Due diligence defence”, in paragraph 17.
Due diligence defence
17. —(1) In any proceedings against a person for an offence under regulation 9, 10, 11 or 12 it is a defence for that person to prove—
(a) that the commission of the offence was due to—
(i) a mistake;
(ii) reliance on information supplied to him by another person;
(iii) the act or default of another person;
(iv) an accident; or
(v) another cause beyond his control; and
(b) that he took all reasonable precautions and exercised all due diligence to avoid the commission of such an offence by himself or any person under his control.
If “taking all reasonable precautions” includes being aware of the lack of any good evidence that what you are selling is effective, then this defence should not be much use for most quacks.
Douglas McLachlan has clarified, below, this difficult question
False claims for health benefits of foods
A separate bit of legislation, European regulation on nutrition and health claims made on food, ref 1924/2006, in Article 6, seems clearer in specifying that the seller has to prove any claims they make.
Article 6
Scientific substantiation for claims
1. Nutrition and health claims shall be based on and substantiated by generally accepted scientific evidence.
2. A food business operator making a nutrition or health claim shall justify the use of the claim.
3. The competent authorities of the Member States may request a food business operator or a person placing a product on the market to produce all relevant elements and data establishing compliance with this Regulation.
That clearly places the onus on the seller to provide evidence for claims that are made, rather than the complainant having to ‘prove’ that the claims are false.
On the problem of “health foods” the two bits of legislation seem to overlap. Both have been discussed in “Trading regulations and health foods“, an editorial in the BMJ by M. E. J. Lean (Professor of Human Nutrition in Glasgow).
“It is already illegal under food labelling regulations (1996) to claim that food products can treat or prevent disease. However, huge numbers of such claims are still made, particularly for obesity ”
“The new regulations provide good legislation to protect vulnerable consumers from misleading “health food” claims. They now need to be enforced proactively to help direct doctors and consumers towards safe, cost effective, and evidence based management of diseases.”
In fact the European Food Standards Agency (EFSA) seems to be doing a rather good job at imposing the rules. This, predictably, provoked howls of anguish from the food industry There is a synopsis here.
“Of eight assessed claims, EFSA’s Panel on Dietetic Products, Nutrition and Allergies (NDA) rejected seven for failing to demonstrate causality between consumption of specific nutrients or foods and intended health benefits. EFSA has subsequently issued opinions on about 30 claims with seven drawing positive opinions.”
“. . . EFSA in disgust threw out 120 dossiers supposedly in support of nutrients seeking addition to the FSD’s positive list.
If EFSA was bewildered by the lack of data in the dossiers, it needn’t hav been as industry freely admitted it had in many cases submitted such hollow documents to temporarily keep nutrients on-market.”
Or, on another industry site, “EFSA’s harsh health claim regime”
“By setting an unworkably high standard for claims substantiation, EFSA is threatening R&D not to mention health claims that have long been officially approved in many jurisdictions.”
Here, of course,”unworkably high standard” just means real genuine evidence. How dare they ask for that!
Enforcement of the law
Article 19 of the Unfair Trading regulations says
19. —(1) It shall be the duty of every enforcement authority to enforce these Regulations.
(2) Where the enforcement authority is a local weights and measures authority the duty referred to in paragraph (1) shall apply to the enforcement of these Regulations within the authority’s area.
Nevertheless, enforcement is undoubtedly a weak point at the moment. The UK is obliged to enforce these laws, but at the moment it is not doing so effectively.
A letter in the BMJ from Rose & Garrow describes two complaints under the legislation in which it appears that a Trading Standards office failed to enforce the law. They comment
” . . . member states are obliged not only to enact it as national legislation but to enforce it. The evidence that the government has provided adequate resources for enforcement, in the form of staff and their proper training, is not convincing. The media, and especially the internet, are replete with false claims about health care, and sick people need protection. All EU citizens have the right to complain to the EU Commission if their government fails to provide that protection.”
This is not a good start. A lawyer has pointed out to me
“that it can sometimes be very difficult to get Trading Standards or the OFT to take an interest in something that they don’t fully understand. I think that if it doesn’t immediately leap out at them as being false (e.g “these pills cure all forms of cancer”) then it’s going to be extremely difficult. To be fair, neither Trading Standards nor the OFT were ever intended to be medical regulators and they have limited resources available to them. The new Regulations are a useful new weapon in the fight against quackery, but they are no substitute for proper regulation.”
Trading Standards originated in Weights and Measures. It was their job to check that your pint of beer was really a pint. Now they are being expected to judge medical controversies. Either they will need more people and more training, or responsibility for enforcement of the law should be transferred to some more appropriate agency (though one hesitates to suggest the MHRA after their recent pathetic performance in this area).
Who can be prosecuted?
Any “trader”, a person or a company. There is no need to have actually bought anything, and no need to have suffered actual harm. In fact there is no need for there to be a complainant at all. Trading standards officers can act on their own. But there must be a commercial element. It’s unlikely that simply preaching nonsense would be sufficient to get you prosecuted, so the Prince of Wales is, sadly, probably safe.
Universities who teach that “Amethysts emit high Yin energy” make an interesting case. They charge fees and in return they are “falsely claiming that a product is able to cure illnesses”.
In my view they are behaving illegally, but we shan’t know until a university is taken to court. Watch this space.
The fact remains that the UK is obliged to enforce the law and presumably it will do so eventually. When it does, alternative medicine will have to change very radically. If it were prevented from making false claims, there would be very little of it left apart from tea and sympathy
Follow-up
New Zealand must have similar laws.
Just as I was about to post this I found that in New Zealand a
“couple who sold homeopathic remedies claiming to cure bird flu, herpes and Sars (severe acute respiratory syndrome) have been convicted of breaching the Fair Trading Act.”
They were ordered to pay fines and court costs totalling $23,400.
A clarification form Douglas McLachlan
On the difficult question of who must prove what, Douglas McLachlan, who wrote Has The UK Quietly Outlawed “Alternative” Medicine?, has kindly sent the following clarification.
“I would agree that it is still for the prosecution to prove that the trader committed the offence beyond a reasonable doubt, and that burden of proof is always on the prosecution at the outset, but I think if a trader makes a claim regarding his product and best scientific evidence available indicates that that claim is false, then it will be on the trader to substantiate the claim in order to defend himself. How will the trader do so? Perhaps the trader might call witness after witness in court to provide anecdotal evidence of their experiences, or “experts” that support their claim – in which case it will be for the prosecution to explain the scientific method to the Judge and to convince the Judge that its Study evidence is to be preferred.
Unfortunately, once human personalities get involved things could get clouded – I could imagine a small time seller of snake oil having serious difficulty, but a well funded homeopathy company engaging smart lawyers to quote flawed studies and lead anecdotal evidence to muddy the waters just enough for a Judge to give the trader the benefit of the doubt. That seems to be what happens in the wider public debate, so it’s easy to envisage it happening a courtroom.”
The “average consumer”.
(3) A commercial practice is unfair if—
(a) it contravenes the requirements of professional diligence; and
(b) it materially distorts or is likely to materially distort the economic behaviour of the average consumer with regard to the product.
It seems,therefore, that what matters is whether the “average consumer” would infer from what is said that a claim was being made to cure a disease. The legal view cited by Mojo (comment #2, below) is that expressions such as “can be used to treat” or “can help with” would be considered by the average consumer as implying successful treatment or cure.
The drugstore detox delusion. A nice analysis “detox” at .Science-based Pharmacy
Shortly after I published my editorial in the New Zealand Medical Journal, Dr Who?, I was delighted to get a letter from someone who had trained in chiropractic and seen it all from the inside.
Sadly this wonderful letter had to be removed within a few weeks of posting it because its author was threatened and bullied by chiropractors. Its author is too young and too vulnerable to risk his future career. As a result of this shameful and vindictive treatment, I was asked to remove the letter and did so immediately. Other copies on the web have now vanished too.
The experiences described in the letter justified much of what I said in the editorial, and in some ways went further. This letter doubtless contributed to dropping of the threatened legal action by chiropractors against the Journal and against me. The letter was posted originally on 21 August 2008, with the permission of its author. See also the follow-up in Chiropractic wars. Part 3: internecine conflict.
Now I have been sent a much more anonymous version, and it is a great pleasure to post this inside information.
| David
I must begin by stating my background in relation to chiropractic. I am a graduate of a chiropractic college and have practiced for several years. I have elected not to register or practice again and have returned to study to begin a new career. Prior to studying chiropractic, I gained undergraduate and postgraduate qualifications in science. First I would like to address your comment about the validity of a qualification from a private chiropractic college, especially in relation to the difference between studying there and studying at a university. A major difference is the education and experience of faculty. At the time I was there, most of the faculty at my college had only undergraduate qualifications (I would suggest that the American DC degree is of undergraduate level as it is the primary qualifying degree for chiropractic in the US and Canada -it is not the equivalent of a doctorate in a British or Australasian university) and have not published in peer-reviewed journals. This is quite different to my experience of universities where the all of the faculty usually have at least a PhD and are actively involved in research. The content of the chiropractic curriculum was voluminous. It included basic sciences, chiropractic subjects and social sciences. The college I attended did not have any laboratory facilities so the experience of learning science from a textbook was quite different to the way I had been taught at university, where each subject had a significant laboratory program that had to be passed separately to pass the subject. As chiropractic is a clinical discipline, the course contained subjects in common with a medical degree. Sadly, the attitude towards medicine and the medical profession was not always the most constructive. For example, I can recall a noticeboard where newspaper clippings of media reports of medical misadventure and adverse effects of pharmaceuticals were posted regularly. Clinical experience was gained by a 2 year internship in the school health centre concurrent with the last 2 years of academic study; so it was not a full-time internship. The requirements for passing this component of the course were complex but centred around seeing a number of patients, a number of visits, performing a number of various kinds of x-rays and reading a number of x-ray films. Every student was responsible for finding all of their own patients to meet the requirements. The result of this was a clinical experience that was quite narrow for most people. This would seem to be quite different to the hospital internship of a medical degree, the clinical internship of a dental degree or the range of placements in a physiotherapy degree in terms of the breadth of experience of different kinds of patients of different ages and states of health. For people who are not aware, there are a range of ideas within chiropractic about what it is and what it is for. The “wellness”, subluxation-based kind of chiropractic is taught by a minority of schools and is what chiropractors call a “philosophical view”. It advocates that chiropractic care be independent from symptoms or treatment and be a regular part of peoples’ lives. The expectation is that healthy, asymptomatic people will be “adjusted” on a regular basis to keep them free from “vertebral subluxation”. To that end, the training at schools that teach this approach is adequate (and probably even excessive). The issue that you wrote about related to the use of the title “doctor” by chiropractors in New Zealand. In licensing chiropractors and allowing them the use of the title “Dr” in front of their names (provided that the title is qualified by the word “chiropractor”) governments have awarded chiropractors with recognition and prestige that has usually been associated with a level of academic achievement or with a medical qualification. It indicates that the bearer of the title can be trusted to give credible advice within their area of expertise. The issue may seem benign, but in allowing chiropractors to use the title, people who would not normally feel safe to submit to the treatment of an alternative health practitioner, choose to try chiropractic. I make this point because at its core, chiropractic is quite different to medicine, dentistry and physiotherapy. A chiropractic office often looks like a lot like a doctor’s surgery. The layout is similar (with waiting rooms and consultation rooms; there are things like stethoscopes and x-ray machines and there are often informative and education posters and brochures. In many cases, the title “doctor” is used in I have found that some people believe chiropractors are medical doctors. Some even believe that chiropractic is a kind of medical speciality. I have seen patients who choose chiropractic as their primary health care and come to a chiropractic office as their first port of call when they are unwell. I Two practices are of particular concern in some chiropractic offices and in my view; these alone should be sufficient reason to prevent chiropractors from calling themselves “doctor”. The first is the systematic and deliberate erosion of a person’s confidence in the medical system. Many offices have anti medical literature in their libraries. Chiropractors are sometimes taught practices to subvert medical credibility. See http://chirobase.org/20PB/top7.html for an example. The second is a subset of the first but is particularly damaging. It is active opposition to vaccination. At chiropractic school, I was taught anti-vaccination information in my paediatrics course. I have seen books written by chiropractors opposing vaccination and I have seen many offices with anti vaccination leaflets and books in abundance. Now I am all for informed choice but this type of material is rarely accurate or balanced. People are being encouraged not to vaccinate their children by professionals who they believe to be a reliable and prestigious source of information. Although it may sound paternalistic to people who have not had the privilege of clinical practice (albeit in a profession I no longer agree with), it made me realise several things. The first is that people who are unwell are vulnerable. The second is that there are people who trust “medical” advice unquestioningly. I believe we should be very careful about who we title as a credible source of advice about health care. Legislation treads a fine line between limiting personal freedom and protecting people from harm. Aside from the qualification being inconsistent with the academic level that is usually required to use the title “Doctor”, the greatest danger, in my opinion, is that the legal recognition and permission to use the title has allowed chiropractors to assume the mantle of a doctor. In the guise of this respectability, some chiropractors are deliberately eroding confidence in doctors and denying children (and possibly populations) the protection of vaccination. David, thank you for having the courage to question the use of the title “doctor” by chiropractors. Historically (and in your case), chiropractors fight their battles through litigation so it takes personal courage and integrity to do so. |
All I can say is, don’t thank me. It doesn’t take much courage at my age. It takes a lot at yours and the world should be grateful to you.
Replies from chiropractors in the NZMJ
The New Zealand Medical Journal, very properly, allowed right of reply to chiropractore. This week’s issue contains three letters, one of which is from Paul Kelly. It is signed “Dr Brian Kelly B App Sci (Chiro), President, New Zealand College of Chiropractic”. This is not quite the same as appears on his College’s web site which shows the president’s welcome.

It seems that Kelly has not been quite so careful about use of his title on the web site because (as of 21 August) the signature on his address looks like this.

“Dr Brian Kelly, President”. That does seem a bit careless, given that his usage of “Dr” was pointed out in my original editorial, published on 25th July.
Replies to these letters appeared in the September 5th issue of NZMJ.
It’s hard enough to communicate basic ideas about how to assess evidence to adults without having the effort hindered by schools.
The teaching of quackery to 16 year-olds has been approved by a maze of quangos, none of which will take responsibility, or justify their actions. So far I’ve located no fewer than eight of them.
[For non-UK readers, quango = Quasi-Autonomous Non-Governmental Organisation].
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
A lot of odd qualifications are accredited by OfQual (see here). Consider, for example, Edexcel Level 3 BTEC Nationals in Health and Social Care (these exams are described here), Download the specifications here and check page 309.
Unit 23: Complementary Therapies for Health and Social Care
NQF Level 3: BTEC National
Guided learning hours: 60Unit abstract
“In order to be able to take a holistic view towards medicine and health care, health and social care professionals need to understand the potential range of complementary therapies available and how they may be used in the support of conventional medicine.”
Well, Goldacre has always said that homeopathy makes the perfect vehicle for teaching how easy it is to be deceived by bad science, so what’s wrong? But wait
“Learners will consider the benefits of complementary therapies to health and wellbeing, as well as identifying any contraindications and health and safety issues in relation to their use.”
Then later
“The holistic approach to illnesses such as cancer could be used as a focus here. For example, there could be some tutor input to introduce ideas about the role of complementary therapies in the treatment and management of cancer, this being followed up by individual or small group research by learners using both the internet and the services available locally/regionally. If available, a local homeopathic hospital, for example, would be an interesting place to visit.”
It’s true that to get a distinction, you have to “evaluate the evidence relating to the use of complementary therapies in contemporary society”, but it isn’t at all clear that this refers to evidence about whether the treatment works.
The really revealing bit comes when you get to the
“Indicative reading for learners
There are many resources available to support this unit.Websites
www.acupuncture.org.uk British Acupuncture Council
www.bant.org.uk British Association for Nutritional Therapy
www.exeter.ac.uk/sshs/compmed Exeter University’s academic department of Complementary medicine
www.gcc-uk.org General Chiropractic Council
www.nimh.org.uk National Institute of Medical Herbalists
www.nursingtimes.net The Nursing Times
www.osteopathy.org.uk General Osteopathic Council
www.the-cma.org.uk The Complementary Medical Association”
This list is truly astonishing. Almost every one of them can be relied on to produce self-serving inaccurate information about the form of “therapy” it exists to promote. The one obvious exception is the reference to Exeter University’s academic department of complementary medicine (and the link to that one is wrong). The Nursing Times should be an exception too, but their articles about CAM are just about always written by people who are committed to it.
It is no consolation that the 2005 version was even worse. In its classification of ‘therapies’ it said “Pharmaceutically mediated: eg herbalism, homeopathy “. Grotesque! And this is the examinng body!
The Teacher
This particular educational disaster came to my attention when I had a letter from a teacher. She had been asked to teach this unit, and wanted to know if I could provide any resources for it. She said that Edexcel hadn’t done so. She asked ” Do you know of any universities that teach CT’s [sic] so I could contact them about useful teaching resources?.” She seemed to think that reliable information about homeopathy could be found from a ‘university’ homeopathy teacher. Not a good sign. It soon emerged why.
She said.
“My students are studying BTEC National Health Studies and the link is Edexcel BTEC National Complimentary [sic] studies.”
“I am a psychotherapist with an MA in Education and Psychology. I am also trained in massage and shiatsu and have plenty of personal experience of alternative therapy”
Shiatsu uh? It seems the teacher is already committed to placebo medicine. Nevertheless I spent some time looking for some better teaching material for 16 year-old children. There is good stuff at Planet
Science, and in some of the pamphlets from Sense about Science, not least their latest, I’ve got nothing to lose by trying it – A guide to weighing up claims about cures and treatments. I sent all this stuff to her, and prefaced the material by saying
“First of all, I should put my cards on the table and say that I am quite appalled by the specification of Unit 23. In particular, it has almost no emphasis at all on the one thing that you want to know about any therapy, namely does it work? The reference list for reading consists almost entirely of organisations that are trying to sell you various sorts of quackery, There is no hint of balance; furthermore it is all quite incompatible with unit 22, which IS concerned with evidence.”
At this point the teacher the teacher came clean too, As always, anyone who disagrees with the assessment (if any) of the evidence by a true believer is unmeasured and inflammatory.
“I have found your responses very unmeasured and inflammatory and I am sorry to say that this prejudicial attitude has meant that I have not found your comments useful.”
shortly followed by
“I am not coming from a scientific background, neither is the course claiming to be scientific.”
That will teach me to spend a couple of hours trying to help a teacher.
What does Edexcel say?
I wrote to Edexcel’s science subject advisors with some questions about what was being taught. The response that I got was not from the science subject advisors but from the Head of Customer support, presumably a PR person.
| From: (Bola Arabome) 12/11/2008 04.31 PM
Dear Professor Colquhoun Thank you for email communication concerning the complementary therapies unit which is available in our BTEC National in Health and BTEC National in Health and Social Care qualifications. I have replied on behalf of Stephen Nugus, our science subject advisor, because your questions do not refer to a science qualification. I would like to answer your questions as directly as possible and then provide some background information relating to the qualifications. The units and whole qualifications for all awarding bodies are accredited by the regulator, the Qualifications and Curriculum Authority. The resource reading list is also produced by us to help teachers and learners. The qualification as a whole is related to the National Occupational Standards for the vocational sectors of Health and Health and social care with consultation taken from the relevant sector skills councils . As you will be aware many of these complementary therapies are available in care centres and health centres under the NHS and in the private sector. The aim of BTEC qualifications is to prepare people for work in these particular sectors. Clearly a critical awareness is encouraged with reference to health and safety and regulation. There are other units, in some cases compulsory, within the qualification with a scientific approach. ‘ ‘ ‘ ‘ ‘ Stephen Harris Head of Customer Support |
Aha, so it seems that teaching people to treat sick patients is “not a science qualification”. Just a business qualification perhaps?. I haven’t yet managed to reach the people who make these decisions, so I persisted with the PR man. Here is part of the next letter (Edexcel’s reply in italic).
| 19 November
I find it quite fascinating that Edexcel regards the treatment of sick patients as not being part of science (“do not refer to a science qualification”). Does that mean Edexcel regard the “Health” part of “Health and Social Care” as being nothing to do with science, and that it therefore doesn’t matter if Health Care is unscientific, or even actively anti-scientific? I am sorry if my answer lacked clarity. My comment, that I had taken your enquiry on behalf of our Science Advisor because this was not a science qualification, was intended to explain why I was replying. It was not intended as a comment on the relationship between Health and Social Care and science. At Edexcel we use bureaucratic categories where we align our management of qualifications with officially recognised occupational sectors. Often we rely on sector bodies such as Sector Skills Councils to endorse or even approve the qualifications we offer. Those involved in production of our Science qualifications and our (4) You say “The qualification as a whole is related to the National Occupational Standards for the vocational sectors of Health and Health and social care with consultation taken from the relevant sector skills councils”. Are you aware that the Skills for Health specifications for Alternative medicine were written essentially by the Prince of Wales Foundation? The qualification was approved by both ‘Skills for Health’ and ‘Skills for Care and Development’ prior to being accredited by QCA. It uses the NOS in Health and Social Care as the basis for many of the mandatory units. The ‘Complementary Therapies’ NOS were not used. This was not a requirement of a ‘Health and Social Care’ qualification. “Are the NOS in Health and Social Care that you mention the ones listed here? http://www.ukstandards.org/Find_Occupational_Standards.aspx?NosFindID=1&ClassificationItemId=174 If so, I can see nothing there about ‘complementary therapies’. if I have missed it, I’d be very grateful if you could let me know where it is. If it is not there, I remain very puzzled about the provenance of Unit 23, since you say it is not based on Skills for Health.” |
Now we are immediately at sea, struggling under a tidal wave of acronyms for endless overlapping quangos. In this one short paragraph we have no fewer than four of them. ‘Skills for Health’, ‘Skills for Care and Development’ , ‘Quality and Curriculum Authority (QCA) and NOS.
It seems that the specification of unit 23 was written by Edexcel, but Harris (25 Nov) declines to name those responsible
“When I refer to our “Health and Social care team” I mean the mix of Edexcel Staff and the associates we employ on a contract basis as writers, examiners and external verifiers. The writers are generally recruited from those who are involved in teaching and assessment the subjects in schools and colleges. The editorial responsibility lies with the Edexcel Staff. I do not have access to the names of the writers and in any case would not be able to pass on this information. Specifications indicate the managers responsible for authorising publication”
“Edexcel takes full responsibility for its ethical position on this and other issues. However we can not accept responsibility for the opinions expressed in third party materials. There is a disclaimer to this effect at the beginning of the specification. ”
” You have the correct link to the Health NOS . These are the standards, which where appropriate, influence our qualifications. However in the case of Unit 23 I understand that there is no link with the Health NOS. I don’t know if the NOS cover the unit 23 content.”
So, contrary to what I was told at first, neither Skills for Health, nor NOS were involved Or were they (see below)?
So who does take responsibility? Aha that is secret. And the approval by the QCA is also secret.
“I cannot provide you with copies of any correspondence between Skills for Health and Edexcel. We regard this as confidential. “
What does the QCA say?
The strapline of the QCA is
“We are committed to building a world-class education and training framework. We develop and modernise the curriculum, assessments, examinations and qualifications.”
Referring school children to the Society of Homeopaths for advice seems to be world-class bollocks rather than world-class education.
When this matter was brought to light by Graeme Paton in the Daily Telegraph, he quoted Kathleen Tattersall, CEO of the QCA. She said
“The design of these diplomas has met Ofqual’s high standards. We will monitor them closely as they are delivered to make sure that learners get a fair deal and that standards are set appropriately.”
Just the usual vacuous bureaucratic defensive sound-bite there. So I wrote to Kathleen Tattersall myself with some specific questions. The letter went on 2nd September 2008. Up to today, 26 November, I had only letters saying
“Thank you for your email of 12 November addressed to Kathleen Tattersall, a response is being prepared which will be forwarded to you shortly.”
“Thank you for your email of 25th November addressed to Kathleen Tattersall. A more detailed response is being prepared which will be sent to you shortly.”
Here are some of the questions that I asked.
| I wrote to Edexcel’s subject advisors about unit 23 and I was told “your questions do not refer to a science qualification”. This seems to mean that if it comes under the name “Health Care” then the care of sick patients is treated as though it were nothing to do with science, That seems to me to be both wrong and dangerous, and I should like to hear your view about that question.
Clearly the fundamental problem here is that the BTEC is intended as a vocational training for careers in alternative medicine, As a body concerned with education, surely you cannot ignore the view of 99% of scientists and doctors that almost all alternative medicine is fraud. That doesn’t mean that you can’t make a living from it, but it surely does create a dilemma for an educational organisation. What is your view of that dilemma? |
Eventually, on 27th November, I get a reply (of sorts) It came not from the Kathleen Tattersall of the QCA but from yet another regulatory body, OfQual, the office of the Qualifications and Examinations Regulator. You’d think that they’d know the answers, but if they do they aren’t telling, [download whole letter. It is very short. The “more detailed response” says nothing.
Ofqual does not take a view on the detailed content of vocational qualifications as that responsibility sits with the relevant Sector Skills Council which represents employers and others involved in the sector. Ofqual accredits the specifications, submitted by sector-skilled professionals, after ensuring they meet National Occupational Standards. Ofqual relies on the professional judgement of these sector-skilled professionals to include relevant subjects and develop and enhance the occupational standards in their profession. The accreditation of this BTEC qualification was supported by both Skills for Health, and Skills for Care and Development, organisations which represent the emerging Sector Qualifications Strategies and comply with the relevant National Occupational Standards Isabel Nisbet Acting Chief Executive |
So no further forward. Every time I ask a question, the buck gets passed to another quango (or two, or three). This letter, in any case, seems to contradict what Edexcel said about the involvement of Skills for Health (that’s the talking to trees outfit),
A nightmare maze of quangos
You may well be wondering what the relationship is between Ofqual and the QCA. There is an ‘explanation’ here.
Ofqual will take over the regulatory responsibilities of the Qualifications and Curriculum Authority (QCA), with stronger powers in relation to safeguarding the standards of qualifications and assessment and an explicit remit as a market regulator. The QCA will evolve into the Qualifications and Curriculum Development Agency (QCDA): supporting Ministers with advice and undertaking certain design and delivery support functions in relation to the curriculum, qualifications, learning and development in the Early Years Foundation Stage, and National Curriculum and Early Years Foundation Stage assessments.
Notice tha QCA won’t be abolished. There will be yet another quango.
The result of all this regulatory bureaucracy seems to be worse regulation, Exactly the same thing happens with accreditiation of dodgy degrees in universities.
At one time, a proposal for something like Unit 23 would have been shown to any competent science teacher, who would have said”you must be joking” and binned it. Now a few hundred bureaucrats tick their boxes and rubbish gets approved.
There seems to be nobody in any of these quangos with the education to realise that if you want to know the truth about homeopathy, the last person you ask is the Society of Homeopaths or the Prince of Wales.
What next?
So the mystery remains. I can’t find out who is responsible for the provenance of the appallingly anti-science Unit 23, and I can’t find out how it got approved. Neither can I get a straight answer to the obvious question about whether it is OK to encourage vocational qualifications for jobs that are bordering on being fraudulent.
.All I can get is platitudes and bland assurances. Everything that might be informative is clouded in secrecy.
The Freedom of Information requests are in. Watch this space. But don’t hold your breath.
Follow-up
Here are some attempts to break through the wall of silence.
Edexcel. I sent them this request.
Freedom of Information Act
Hello
I should like to see please all documents from Edexcel and OfQual or QCA (and communications between then) that concern the formulation and approval of Unit 23 (Complementary Therapies) in the level3 BTEC (page 309 in attached document). In vew of the contentious nature of the subject matter, I believe that is is in the public interest that this information be provided
David Colquhoun
The answer was quite fast, and quite unequivocal, Buzz off.
| Dear Mr Colquhoun,
Thank you of your e-mail of today’s date. I note your request for information pursuant to The Freedom of Information Act. As you may know this Act only applies to public bodies and not to the private sector. Edexcel Limited is privately owned and therefore not subject to this Act. Edexcel is therefore not obliged to provide information to you and is not prepared to give you the information you seek. Please do not hesitate to contact me again if you have any further queries. Kate Gregory |
This lack of public accountability just compounds their appalling inability to distinguish education from miseducation.
International Therapy Examination Council (ITEC)
Mojo’s comment, below, draws attention to the Foundation degree in Complementary Therapies offered by Cornwall College, Camborne, Cornwall (as well as to the fact that the Royal National Lifeboat Institution has been wasting money on ‘research’ on homeopathy –write to them).
At least the courses are held on the Camborne campus of Cornwall College, not on the Duchy campus (do we detect the hand of the Quacktitioner Royal in all this nonsense?).
Cornwall College descends to a new level of barminess in its course Crystal Healing VTCT Level 3
“Who is this course for?
This course is designed to enhance the skills of the Holistic Therapist. Crystals may be used on their own in conjunction with other therapies such as Indian Head Massage, Aromatherapy and Reflexology. Due to the nature of the demands of the holistic programme this course is only suitable for students over the age of 18.”
“What will I be doing on the course?
Students will study the art of Crystal healing which is an energy based treatment where crystals and gemstones are used to channel and focus various energy frequencies.”
| .VTCT stands for the Vocational Training Charitable Trust.
It is yet another organisation that runs vocational exams, and it is responsible for this particular horror |
The crystals are here. I quote.
Objectives
- the use of interpersonal skills with client
- how to complement other therapies with crystals
- the types and effects of different crystals
- uses of crystals including cleansing, energising, configurations
- concepts of auras and chakras
This is, of course, pure meaningless nonsense. Utter bollocks being offered as further education
Cornwall College has many courses run by ITEC.
The College says
“You will become a professional practitioner with the International Therapy Examination Council (ITEC), study a number of essential modules to give a vocational direction to your study that include: Homeopathy and its application,”
| Who on earth, I hear you cry, are ITEC? That brings us to the seventh organisation in the maze of quangos and private companies involved in the miseducation of young people about science and medicine. It appears, like Edexcel, to be a private company though its web site is very coy about that. |
After the foundation degree you can go on to “a brand new innovative BSc in Complementary Health Studies (from Sept 2009)”
The ITEC web site says
- ITEC qualifications are accredited by the Office of the Qualifications and Examination Regulator (OFQUAL)
- ITEC qualifications are funded in the uk by the on behalf of Department for Innovation, Universities and Skills (DIUS)
- ITEC qualifications have been mapped to the National Occupational Standards, where they exist
Oddly enough, there is no mention of accreditation by a University (not that that is worth much). So a few more Freedom of Information requests are going off, in an attempt to find out why are kids are being miseducated about science and medicine.
Meanwhile you can judge the effect of all that education in physiology by one of the sample questions for ITEC Unit 4, reflexology.
The pancreas reflex:
A Extends across both feet
B Is on the right foot only
C Is on the left foot only
D Is between the toes on both feet
Uhuh, they seem to have forgotten the option ‘none of the above’.
Or how about a sample question from ITEC Unit 47 – Stone Therapy Massage
Which organ of the body is associated with the element fire?
A Heart
B Liver
C Spleen
D Pancreas
Or perhaps this?
Which incantation makes hot stones work best?
A Incarcerous
B Avada Kedavra,
C Dissendium
D Expelliarmus.
(OK I made the last one up, with help from Harry Potter, but it makes just about as much sense as the real ones).
And guess what? You can’t use the Freedom of Information Act to find out how this preposterous rubbish got into the educational system because ” ITEC is a private organisation therefore does not come under this legislation”. The ability to conduct business in secret is a side effect of the privatisation of public education is another reason why it’s a bad idea.
Ofsted
|
Ofsted has inspected Cornwall College. They say “We inspect and regulate to achieve excellence in the care of children and young people, and in education and skills for learners of all ages.”. I can find no mention of this nonsense in their report, so I’ve asked them. |
|
Ofsted has admitted a spectacular failure in its inspection of child care in the London Borough of Haringey. Polly Curtis wrote in the Guardian (6 Dec 2008) “We failed over Haringey – Ofsted head”. It was the front page story. But of course Ofsted don’t take the blame, they say they were supplied with false information,
That is precisely what happens whenever a committee or quango endorses rubbish. They look only at the documents sent to them and they don’t investigate, don’t engage their brains.
In the case of these courses in utter preposterous rubbish, it seems rather likely that the ultimate source of the misinformation is the Princes’ Foundation for Integrated Health. Tha views of the Prince of Wales get passed on to the ludicrous Skills for Health and used as a criterion by all the other organisations, without a moment of critical appraisal intervening at any point.
2 December 2008 A link from James Randi has sent the hit rate for this post soaring. Someone there left are rather nice comment.
“A quango seems to be a kind of job creation for the otherwise unemployable ‘educated ‘( degree in alternative navel contemplation) middle classes who can’t be expected to do anything useful like cleaning latines ( the only other thing they seem qualified for ). I really hate to think of my taxes paying for this codswollop.”
The publication of Gilbey’s paper and my editorial in the New Zealand Medical Journal (NZMJ) led to a threat of legal action by the NZ Chiropractors’ Association Inc for alleged defamation. After publishing a defiant editorial, the editor of the NZMJ offered chiropractors the chance to put their case.
In the last issue of NZMJ (22 Aug 2008) three letters appeared. One was from Brian Kelly, (President, New Zealand College of Chiropractic) [download letter]. One was from Karl Bale (CEO/Registrar, Chiropractic Board New Zealand) [download letter], and one was from Simon Roughan (Registered Chiropractor and Acting President of the New Zealand Chiropractors’ Association) [download letter].
In the current issue (5 September 2008) Gilbey, Ernst and I responded.{download Gilbey response] [download Ernst response].
Here’s mine. The printed version differs in minor ways [download pdf]
| I’m grateful for the opportunity to reply to the defences of chiropractic from Kelly1, Roughan2 and Bale3 in your last issue.
I’d like first to deal with the minor matter of titles, before getting on to the more important question of vidence. I notice that Brian Kelly signs his letter “Dr Brian Kelly B App Sci (Chiro)” in his letter to NZMJ. He seems to be a bit less careful in his use of titles on his own school’s web site where his president’s welcome4 is signed simply “Dr Brian Kelly”, a title he adopts in at least three other places. Karl Bale3 (CEO/Registrar, Chiropractic Board New Zealand) points out that “Failure to qualify the use of the title ‘Doctor’ may contravene the provisions of the Medical Practitioners Act 1995”. One wonders whether Bale has done anything to stop Kelly’s apparent breaches of this rule? This example makes on wonder whether the Chiropractic Board take its responsibilities seriously? It seems often to be the case that ‘voluntary self-regulation’ doesn’t work, because there are too many vested interests. Karl Bale points out that some ruthless sales methods characteristic of chiropractic are also contrary to the Chiropractic Board’s code of ethics. One would hope their well-known antipathy to vaccination and to medicine as a whole were also considered unethical. These practices seem to continue so the the code of ethics It seems to me quite remarkable that none of the letters mentions the ‘subluxation’ that lies at the heart of their subject6. Could that be because they are reluctant to admit openly that it is a mere metaphysical concept, that no one can see or define? It is sad that so many patients are subjected to X-rays in search of this phantom idea. It is this metaphysical nature of chiropractic that separates it quite clearly from science. Brian Kelly says “How can any reader take seriously, anything suggested by a writer who opines that a 19th Century journalist possessed superior “intellectual standards” to “the UK’s Department of Health” and “several university vice chancellors”. The views of the Davenport Leader on chiropractic were mild compared with those of the great H.L. Mencken (1924)7 who wrote “This preposterous quackery flourishes lushly in the back reaches of the Republic, and begins to conquer the less civilized folk of the big cities….” The problem is that the Department of Health is full of arts graduates who may be very good at classics but can’t understand the nature of evidence. And the UK has one vice-chancellor, a geomorphologist, who defends a course in his university that teaches that “amethysts emit high yin energy”8 I’ll admit, though, that perhaps ‘intellect’ is not what’s deficient in this case, but rather honesty. Your correspondents seem to confuse the duration of a course with its intellectual content. You can study homeopathy for years too, but after all that they are still treating sick people with medicines that contain no medicine. Anyone who works in a university knows that you can easily get accreditation for anything whatsoever if you choose the right people to sit on the committee. I have seen only too many of these worthless pieces of paper. “Amethysts emit high yin energy”8 was part of an accredited course (at the University of Westminster) too. Need I say more? Now to the real heart of the problem, namely the question of evidence. Brian Kelly says that the book by Singh and Ernst9 shows “extreme bias”, but what that book actually shows is an extremely scrupulous regard for evidence, Ernst is in a better position to do this than just about anyone else. He has qualified and practised both regular and alternative medicine, and he was appointed to his present position, as professor of complementary and alternative medicine to assess the evidence. Perhaps most importantly of all, his position allows him to do that assessment with complete lack of bias because, unlike Kelly, his livelihood does not depend on any particular outcome of the assessment. I’m afraid that what Kelly describes as “extreme bias” is simply a display of pique because it has turned out that when all the evidence is examined dispassionately, the outcome is not what chiropractors hoped. The fact of the matter is that when you look at all of the evidence, as Singh & Ernst do, it is perfectly clear that chiropractic is at best no better than conventional treatments even for back pain. For all other conditions its benefits fail to outweigh its risks – contrary to the many claims by chiropractors. Both the New Zealand and the UK governments have got themselves into an impossible position by giving official recognition to chiropractic before the evidence was in. Since the conventional manipulative treatments are cheaper, and may be well be safer, and because they involve no quasi-religious ideas like “subluxation” or “innate intelligence”, the only reasonable conclusion is that there is no need for chiropractic to exist at all. They do nothing they do that could not be done as well by medical practitioners and physiotherapists. What will governments do about that, I wonder? David Colquhoun 1. Kelly, B. New Zealand College of Chiropractic response to 2. Roughan, S. Setting the record straight: New Zealand Chiropractors’ Association response letter. NZMJ 22 3. Bale, 4. http://www.nzchiro.co.nz/about_president.php 6. http://www.chirobase.org/01General/chirosub.html 7. http://www.geocities.com/healthbase/mencken_chiro.html 8. http://dcscience.net/?p=227 9. Singh S, Ernst E. Trick or Treatment. Bantam Press; 2008 |
The wars within chiropractic
Although the chiropractors seem to be rather upset by the criticisms that have been levelled against them, the most interesting war is not between chiropractors and people who think that medicine should not be based on metaphysics. It’s the war within chiropractic itself.
The internecine wars within chiropractic have been going almost from the day it was invented. The (ex-)insider’s view gives us a rare insight into what chiropractic schools actually do. Now support has come from a rather unexpected quarter. An article by five chiropractors has just appeared by Murphy et al. (Chiropractic & Osteopathy, 2008, 16:10).
Although the authors declare that they have “a financial interest in the success” of chiropractic, the changes that they propose are so drastic that, if implemented, tthey would leave little left to distinguish chiropractic from, say, physiotherapy. The authors ask the very pertinent question, ‘why is it that podiatry (chiropody in the UK) is well accepted and chiropractic remains on the controversial fringe of medicine?.. Here are some quotations.
“It is also vital that those chiropractors who dogmatically oppose common public health practices, such as immunization [15] and public water fluoridation, cease such unfounded activity.”
“We are concerned that the common perception (which is well supported, in our experience) that chiropractors are only interested in “selling” a lifetime of chiropractic visits may be one of the primary factors behind our low standing in the minds of members of the public [2].”
“One of the problems that we encounter frequently in our interaction with chiropractic educational institutions is the perpetuation of dogma and unfounded claims. Examples include the concept of spinal subluxation as the cause of a variety of internal diseases and the metaphysical, pseudo-religious idea of “innate intelligence” flowing through spinal nerves, with spinal subluxations impeding this flow. These concepts are lacking in a scientific foundation [27] [28] [29] and should not be permitted to be taught at our chiropractic institutions as part of the standard curriculum. Much of what is passed off as “chiropractic philosophy” is simply dogma [30], or untested (and, in some cases, untestable) theories [27] which have no place in an institution of higher learning, except perhaps in an historical context.”
“The Council on Chiropractic Education requirement of 250 adjustments forces interns to use manipulation on patients whether they need it or not, and the radiographic requirement forces interns to take radiographs on patients whether they need them or not.”
“They [podiatrists] did not invent a “lesion” and a “philosophy” and try to force it on the public. They certainly did not claim that all disease arose from the foot, without any evidence to support this notion. The podiatric medical profession simply did what credible and authoritative professions do [32] – they provided society with services that people actually wanted and needed.”
“In the beginning, DD Palmer invented a lesion, and a theory behind this lesion, and developed a profession of individuals who would become champions of that lesion. This is not what credible professions do.”
“In the interim it [chiropractic] has seen its market share dwindle from 10% of the population [4] to 7.5% [3] [42]. Even amongst patients with back pain, the proportion of patients seeing chiropractors dropped significantly between 1987 and 1997, a period of time in which the proportion seeing both medical doctors and physical therapists increased [43].”
“When an individual consults a member of any of the medical professions, it is reasonably expected that the advice and treatment that he or she receives is based in science, not metaphysics or pseudoscience.”
“The chiropractic profession has an obligation to actively divorce itself from metaphysical explanations of health and disease as well as to actively regulate itself in refusing to tolerate fraud, abuse and quackery, which are more rampant in our profession than in other healthcare professions [46].”
“Podiatric medicine is a science-based profession dedicated to the diagnosis and treatment of foot disorders. Foot reflexology is a metaphysically-based group consisting of non-physicians who believe that many physical disorders arise from the foot. Podiatrists have rejected foot reflexology as an unproven and unscientific practice, and do not consider it part of mainstream podiatric practice.”
“We must finally come to the painful realization that the chiropractic concept of spinal subluxation as the cause of “dis-ease” within the human body is an untested hypothesis [27]. It is an albatross around our collective necks that impedes progress.”
All this, remember, comes from five chiropractors. That looks like all out war between their view of chiropractic and that taught in New Zealand College of Chiropractic, and, in the UK by the three chiropractic colleges in the UK.
Follow-up
A report in the New Zealand Herald (18 September 2008) is rather relevant to all this.
Chiropractor to apologise after patient has stroke
A chiropractor has been recommended to apologise to a woman patient who suffered a stroke after he treated her.
The case report is here.
The Advertising Standards Authority has had a bit to say about chiropractors too.
An editorial in today’s issue of the New Zealand Medical Journal prints in full a letter sent to the Journal by Paul Radich, a lawyer who acts for the New Zealand Chiropractors’ Association Inc and its members. The letter alleges defamation by Andrew Gilbey’s article, and by my editorial which sets the wider context of his paper. The articles in question are here.
Here are some quotations from the Editorial by the Journal’s editor, Professor Frank A Frizelle, Department of Surgery, Christchurch Hospital, NZ. [Download the whole editorial].
| In the article by Gilbey, data is provided about use of inappropriate titles by New Zealand practitioners of acupuncture, chiropractic, and osteopathy while the greater context is provided by Colquhoun. The comments made by Paul Radich are entirely consistent with the response as expressed by Professor Edzard Ernst (Editor-in-Chief of Focus on Alternative and Complementary Medicine (FACT) and Chair in Complementary Medicine at the University of Exeter) in his humorous article In praise of the data-free discussion. Towards a new paradigm5 when he states “data can be frightfully intimidating and non-egalitarian”. . . . The Journal has a responsibility to deal with all issues and not to steer clear of those issues that are difficult or contentious or carry legal threats. Let the debate continue in the evidence-based tone set by Colquhoun and others. I encourage, as we have done previously, the chiropractors and others to join in, let’s hear your evidence not your legal muscle. |
My article said nothing that has not been said many times before. I regard it as fair scientific comment, and I believe that expression of those opinions is in the public interest, The reaction of the Journal is thoroughly admirable.
The outcome of legal bullying can be very counterproductive, as the UK’s Society of Homeopaths found recently to their cost.
The lawyers’ letter demanded a response by 11th August, but in the advice of a lawyer I have decided to ignore for now this rather crude attempt to stifle discussion.
For further developments, watch this space.
The story was picked up within hours, It seems that a storm may be brewing round the world for New Zealand Chiropractors. Here are some of them.
Silence Dissent Ben Goldacre’s badscience,net
HolfordWatch Professor Frizelle’s Instant Classic: Let’s hear your evidence not your legal muscle
The first New Zealand site.
More Legal Chill -from spine-cracking chiropractors on jdc325’s blog
And A beginners guide to chiropractic, on the same site.
Andy Lewis’s Quackometer takes a sharp look too, in They are bone doctors aren’t they?
Support from a NZ blog, Evidence-based thought NZ Chiropractors vs NZ Medical Journal
And another New Zealand blog, Chiropractors attack NZ Medical Journal on SillyBeliefs.com
and another: Evidence should trump “legal muscle”, on “Open Parachute. The mind doesn’t work if it’s closed”
New Zealand Doctor magazine. “Kiwi-practors legal wrangle” in the Nature world news blog, The Great Beyond.
“Self-destructing chiropractors” on Jonathan Hearsay’s blog is particularly interesting because he is a (sceptical) osteopath. He says “Chiropractors are seemingly hell-bent on destroying themselves as a therapy”.
There are now so many allusions on the web to the behaviour of the New Zealand Chiropractors’ Association Inc that I’ll give up trying to list all of them. Their action seems tp have done much to damage their own reputation.
Shortly after this came the news that the British Chiropractic Association is to sue one of out best science communicators, Simon Singh, because he had the temerity to inspect the evidence and give his opinion about it in the Guardian. His original article has gone (for now) from the Guardian web site, but as always happens with attempts at bullying and intimidation, it is more easily available then ever, For example here, and here.
Chiropractic in the UK is analysed by Andy Lewis on Quackometer,
The article below is an editorial that I was asked to write for the New Zealand Medical Journal, as a comment on article in today’s edition about the misuse of the title ‘doctor’ by chiropractors [download pdf]. Titles are not the only form of deception used by chiropractors, so the article looks at some of the others too. For a good collection of articles that reveal chiropractic for what it is, look at Chirobase
THE NEW ZEALAND
MEDICAL JOURNAL
Journal of the New Zealand Medical Association
NZMJ 25 July 2008, Vol 121 No 1278; ISSN 1175 8716

URL: http://www.nzma.org.nz/journal/121-1278/3158/ ©NZMA
Doctor Who?
Inappropriate use of titles by some alternative “medicine” practitioners
David Colquhoun
Who should use the title ‘doctor’? The title is widely abused as shown by Gilbey1 in this issue of the NZMJ in an article entitled Use of inappropriate titles by New Zealand practitioners of acupuncture, chiropractic, and osteopathy. Meanwhile, Evans and colleagues 2, also in this issue, discuss usage and attitudes to alternative treatments.
Gilbey finds that the abuse of the title doctor is widespread and that chiropractors are the main culprits. An amazing 82% of 146 chiropractics used the title Doctor, andL most of them used the title to imply falsely that they were registered medical practitioners.
Although it is illegal in New Zealand to do that, it seems clear that the law is not being enforced and it is widely flouted. This is perhaps not surprising given the history of chiropractic. It has had a strong element of ruthless salesmanship since it was started in Davenport, Iowa by D.D. Palmer (1845–1913). His son, B.J. Palmer, said that their chiropractic school was founded on “a business, not a professional basis. We manufacture chiropractors. We teach them the idea and then we show them how to sell” (Shapiro 2008)3 It is the same now. You can buy advice on how to build “build high-volume, subluxation-based, cash-driven, lifetime family wellness practices”
In her recent book3 , Rose Shapiro comments on the founder of chiropractic as follows.
“By the 1890s Palmer had established a magnetic healing practice in Davenport, Iowa, and was styling himself “doctor”. Not everyone was convinced, as a piece about him in an 1894 edition of the local paper, the Davenport Leader, shows.
A crank on magnetism has a crazy notion hat he can cure the sick and crippled with his magnetic hands. His victims are the weak-minded, ignorant and superstitious,those foolish people who have been sick for years and have become tired of the regular physician and want health by the short-cut method he has certainly profited by the ignorance of his victim. His increase in business shows what can be done in Davenport, even by a quack.”
D.D. Palmer was a curious mixture: grocer, spiritual healer, magnetic therapist, fairground huckster, religious cult leader—and above all, a salesman. He finally found a way to get rich by removing entirely imaginary “subluxations”.
Over 100 years later, it seems that the “weak-minded, ignorant, and superstitious” include the UK’s Department of Health, who have given chiropractics a similar status to the General Medical Council.
The intellectual standards of a 19th Century Mid-Western provincial newspaper journalist are rather better than the intellectual standards of the UK’s Department of Health, and of several university vice-chancellors in 2007.
Do the treatments work?
Neither Gilbey nor Evans et al. really grasp the nettle of judging efficacy. The first thing one wants to know about any treatment —alternative or otherwise — is whether it works. Until that is decided, all talk of qualifications, regulation, and so on is just vacuous bureaucratese. No policy can be framed sensibly until the question of efficacy has been addressed honestly.
It is one good effect of the upsurge of interest in alternative treatments that there are now quite a lot of good trials of the most popular forms of treatments (as well as many more bad trials). Some good summaries of the results are now available too. Cochrane reviews set the standard for good assessment of evidence. New Zealand’s Ministry of Health commissioned the Complementary and Alternative Medicine
website to assess the evidence, and that seems to have done a good job too. Their assessment of chiropractic treatment of low back pain is as follows:
There appears to be some evidence from one systematic review and four other studies, although not conclusive, that chiropractic treatment is as effective as other therapies but this may be due to chance. There is very little evidence that chiropractic is more effective than other therapies.
And two excellent summaries have been published as books this year. Both are by people who have had direct experience of alternative treatments, but who have no financial interest in the outcome of their assessment of evidence. The book by Singh and Ernst4 summarises the evidence on all the major alternative treatments, and the book by Bausell5 concentrates particularly on acupuncture, because the author was for 5 years involved in research in that area, Both of these books come to much the same conclusion about chiropractic. It is now really very well-established that chiropractic is (at best) no more effective than conventional treatment. But it has the disadvantage of being surrounded by gobbledygook about “subluxations” and, more importantly, it kills the occasional patient.
Long (2004)7 said “the public should be informed that chiropractic manipulation is the number one reason for people suffering stroke under the age of 45.”
The chiropractors of Alberta (Canada) and the Alberta Government are now facing a class-action lawsuit8. The lead plaintiff is Sandra Nette. Formerly she was a fit 41 year old. Now she is tetraplegic. Immediately
after neck manipulation by a chiropractor she had a massive stroke as a result of a torn vertebral artery.
Acupuncture comes out of the assessments equally badly. Bausell (2007) concludes that it is no more than a theatrical placebo.
Are the qualifications even real?
It is a curious aspect of the alternative medicine industry that they often are keen to reject conventional science, yet they long for academic respectability. One aspect of this is claiming academic titles on the flimsiest of grounds. You can still be held to have misled the public into thinking you are a medical
practitioner, even if you have a real doctorate. But often pays to look into where the qualifications come from.
A celebrated case in the UK concerned the ‘lifestyle nutritionist’, TV celebrity and multi-millionaire, Dr Gillian McKeith, PhD. A reader of Ben Goldacre’s excellent blog, badscience.net did a little investigation. The results appeared in Goldacre’s Bad Science column in the Guardian9.
She claimed that her PhD came from the American College of Nutrition, but it turned out to come from a correspondence course from a non-accredited US ‘college’. McKeith also boasted of having “professional membership” of the American Association of Nutritional Consultants, for which she provided proof of her degree and three professional references.
The value of this qualification can be judged by the fact that Goldacre sent an application and $60 and as a result “My dead cat Hettie is also a “certified professional member” of the AANC. I have the certificate hanging in my loo”.
Is the solution government regulation?
In New Zealand the law about misleading the public into believing you are a medical practitioner already exists. The immediate problem would be solved if that law were taken seriously, but it seems that it is not.
It is common in both the UK and in New Zealand to suggest that some sort of official government regulation is the answer. That solution is proposed in this issue of NZMJ by Evans et al2. A similar thing has been proposed recently in the UK by a committee headed by Michael Pittilo, vice-chancellor of Robert Gordon’s University, Aberdeen.
I have written about the latter under the heading A very bad report. The Pittilo report recommends both government regulation and more degrees in alternative medicine. Given that we now know that most alternative medicine doesn’t work, the idea of giving degrees in such subjects must be quite ludicrous to any thinking person.
The magazine Nature7 recently investigated the 16 UK universities who run such degrees. In the UK, first-year students at the University of Westminster are taught that “amethysts emit high yin energy” . Their vice chancellor, Professor Geoffrey Petts, describes himself a s a geomorphologist, but he cannot be tempted to express an opinion about the curative power of amethysts.
There has been a tendency to a form of grade inflation in universities—higher degrees for less work gets bums on seats. For most of us, getting a doctorate involves at least 3 years of hard experimental research in a university. But in the USA and Canada you can get a ‘doctor of chiropractic’ degree and most chiropractic (mis)education is not even in a university but in separate colleges.
Florida State University famously turned down a large donation to start a chiropractic school because they saw, quite rightly, that to do so would damage their intellectual reputation. This map, now widely distributed on the Internet, was produced by one of their chemistry professors, and it did the trick.
Other universities have been less principled. The New Zealand College of Chiropractic [whose President styles himself “Dr Brian Kelly”,though his only qualification is B. App Sci (chiro)] is accredited by the New Zealand Qualifications Authority (NZQA). Presumably they, like their UK equivalent (the QAA), are not allowed to take into account whether what is being taught is nonsense or not. Nonsense courses are accredited by experts in nonsense. That is why much accreditation is not worth the paper it’s written on.
Of course the public needs some protection from dangerous or fraudulent practices, but that can be done better (and more cheaply) by simply enforcing existing legislation on unfair trade practices, and on false advertising. Recent changes in the law on unfair trading in the UK have made it easier to take legal action against people who make health claims that cannot be justified by evidence, and that seems the best
way to regulate medical charlatans.
Conclusion
For most forms of alternative medicine—including chiropractic and acupuncture—the evidence is now in. There is now better reason than ever before to believe that they are mostly elaborate placebos and, at best, no better than conventional treatments. It is about time that universities and governments recognised the evidence and stopped talking about regulation and accreditation.
Indeed, “falsely claiming that a product is able to cure illnesses, dysfunction, or malformations” is illegal in Europe10.
Making unjustified health claims is a particularly cruel form of unfair trading practice. It calls for prosecutions, not accreditation.
Competing interests: None.
NZMJ 25 July 2008, Vol 121 No 1278; ISSN 1175 8716
URL: http://www.nzma.org.nz/journal/121-1278/3158/ ©NZMA
Author information: David Colquhoun, Research Fellow, Dept of Pharmacology, University College London, United Kingdom (http://www.ucl.ac.uk/Pharmacology/dc.html)
Correspondence: Professor D Colquhoun, Dept of Pharmacology, University College London, Gower Street, London WC1E 6BT, United Kingdom. Fax: +44(0)20 76797298; email: d.colquhoun@ucl.ac.uk
References:
1. Gilbey A. Use of inappropriate titles by New Zealand practitioners of acupuncture, chiropractic, and osteopathy. N Z Med J. 2008;121(1278). [pdf]
2. Evans A, Duncan B, McHugh P, et al. Inpatients’ use, understanding, and attitudes towards traditional, complementary and alternative therapies at a provincial New Zealand hospital. N Z Med J. 2008;121(1278).
3 Shapiro. Rose. Suckers. How Alternative Medicine Makes Fools of Us All Random House, London 2008. (reviewed here)
4. Singh S, Ernst E. Trick or Treatment. Bantam Press; 2008 (reviewed here)
5. Bausell RB. Snake Oil Science. The Truth about Complementary and Alternative Medicine. (reviewed here)
Oxford University Press; 2007
6. Colquhoun D. Science degrees without the Science, Nature 2007;446:373–4. See also here.
7. Long PH. Stroke and spinal manipulation. J Quality Health Care. 2004;3:8–10.
8. Libin K. Chiropractors called to court. Canadian National Post; June21, 2008.
9. Goldacre B. A menace to science. London: Guardian; February 12, 2007/
10. Department for Business Enterprise & Regulatory Reform (BERR). Consumer Protection from Unfair Trading Regulations 2008. UK: Office of Fair Trading.