
Download Lectures on Biostatistics (1971). Corrected and searchable version of Google books edition
Download review of Lectures on Biostatistics (THES, 1973).
evidence
This is the first of a several posts that have arisen from a visit to North America. One thing that the trip led to was an interest in how HR departments influence science -if you have a story about that, please email me.
Following the media publicity that surrounded the lecture in Toronto, I was sent this poem by Anne Spencer, of Canada.
It is based on the style of Jonathan Swift (1667-1745), and she had earlier went a more political version, below, which was a runner up in the international Swift satire poetry competition, 2004. Anne Spencer has been kind enough to let me reproduce both her poems here.
What men wish, they like to believe.
Julius Caesar
Verses on folly, faith and fantasy
Great Caesar saw what we still find
In much of modern humankind,
That wishful thinking will suppress
The reason we should all possess.
Take health. That is a main concern.
We look for cures at every turn
For sicknesses that cause unease
And nasty things that bring disease.
But from the science of the age
Too many now will disengage,
Forget the studies, evidence
Of remedies that will dispense
A tested way of healing those
Conditions doctors diagnose.
They say they’ve lost their confidence
In science, and have a preference
For substances that they perceive
Fit in with what they all believe
In nature’s realm of field and flowers,
Along with supernatural powers
Or energies that ebb and flow
And are released by those who know
The proper touch or breath or spell
For proper paying clientele.
And other forms of therapy
Like healing touch they all agree
Despite their failure to explain
Result in easing of their pain.
For grave conditions that could kill
It’s nature’s bounty fills the bill,
From goats a serum crushes AIDS
And grape juice makes Altzheimers fade,
Red clover makes the blood come clean
And sugar pills become routine
As remedies for things they feel
They cannot count on science to heal.
And substances that they produce
To cure complaints or pain reduce
They say they must dilute and then
Dilute, dilute, dilute again
Because the less you have, not more
Will guarantee a better cure.
(Conclusions such as this imply
There’s no attempt to reason why.)
And quite impervious they stay
To anything their critics say
About placebos and effects
That challenge rational intellects.
Their gurus sanction their belief
That things they give them bring relief
From anything they want to try,
(Because the more they wish, they buy)
If people give them hope and say
That black is white, then that’s OK.
But there’s the rub – for harm can come
By seeing this as rule of thumb
For if you disregard the facts
That science tells, then this detracts
From treatments that show evidence
Of beneficial consequence.
More harm than good can come to those
Rejecting treatments that propose
Results that doctors can compile
Which don’t depend upon a smile
Or harmony with sundry forces
Brought to bear by doubtful sources.
So those who wish upon a star
Or herb or potion in a jar
To grant relief from ache or pain
Could well decide to think again
And weigh the chances that desire
Not reason is what we require
To make us well when we succumb
To ailments that are troublesome.
For wishful thoughts beguile the mind
But leave reality behind.
And here is the political version of Anne Spence’s poem
Great Caesar, famed in Gallic wars,
A champion of the Roman cause,
Who came, and saw and conquered when
The sword was mightier than the pen,
Was yet a statesman, author, who
Knew much of human nature too.
For Caesar saw what we still find
In much of modern humankind,
That wishful thinking reason dims
And validates our selfish whims.
But more we see in public spheres
How much this maxim oft appears,
To show how leaders are consumed
By things believed their wish presumed.
And lately this seems quite okay
With rulers of the USA.
(But we, like Swift, will make our claim
By ‘lashing vice’ but sparing name).
With politics that are complex
Illusions tend to blur the specs
When men believe whate’er they wish
Some policies get devilish.
And when you add religion too
We have a complicated brew,
And here a leader we can see
Who joins the ruling company
Of men who demonstrate the state
Of those who wish with truth equate.
He left a weak addicted past
To seek his destiny at last.
Became a Christian, born again
Aspiring to a higher plane.
(Genetically he was ahead
Since daddy had the nation led.)
But, once elected by a fluke,
(That all just men would sure rebuke)
He saw his mission godly sent
To show the world enlightenment.
And he believed that evil dwelt
Within an oil producing belt,
Its ruler evil incarnate
A tyrant quite degenerate.
And so when terrorists attacked
The World Trade towers, this proved the fact,
Or so he said, for who could not
Connect events with dot to dot?
He’d purge the world of evil’s stain
In person of Saddam Hussein.
He would not shrink from duty’s call
To seek Saddam’s decline and fall,
For he believed his destiny
Proclaimed by God – Divine decree.
He’d find the hidden weapons and
He’d bring new freedom to the land
Where western values were deplored
By villains who lived by the sword
(Or torture, rape, or nasty gases
With which they murdered ethnic masses).
And so he would avenge the dead,
Depose the tyrant, and instead
Lead on his troops –at least he’d send
Them forth to bring about this end.
God chose him evil to despoil
(And as reward he’d get the oil).
Despite the cautions he received
He was inspired, he still believed
His mission was to crush this foe
Both God and Tony told him so.
So off to conquer all that’s bad
The forces left to bomb Baghdad.
Their leader stayed at home to see
How his crusade looked on tv.
The mighty tanks, the skies aflame
Were better than a video game.
The statues fell, the prisoners freed
The regime’s downfall guaranteed
The patriot missiles, patriot men
Would soon, he thought, be home again.
Though some had breathed their final breath
The ‘victory’ justified their death
And they’d be heroes ever more
While blest upon another shore.
They played their part, they fought the fight,
Their president bid them goodnight.
They left behind a populace
Who now could western life embrace.
Well, most of it – religiously
They kept their views on sanctity.
Their heaven, they said, was nicer, and
They could have virgins on demand.
(It seems this wish- belief thing will
For any culture fill the bill).
But though the war, it seemed, was won
The problems only had begun.
The leader’s view that freedom would
Make people act the way they should
Once out from under evil’s thrall,
It turned out didn’t work at all.
Because he’d only wished , not thought
Things through with wisdom as he ought,
The leader found his plans rejected
Much more than he had once expected.
His mandate from his holy source
Was not so easy to enforce.
His ignorance of tribal clans,
Of loyalties and partisans,
Reliance on intelligence
Which didn’t make a lot of sense,
Attending to his favourites
And lots of other deficits,
Caused wild confusion in the land
So hard for him to understand.
The law and order that he craved,
Now he’d removed the ones depraved
Was not forthcoming, but instead
A lot more people ended dead.
But still he had to carry on,
With pressure from the Pentagon,
Because he thought and wished it so
That God would help him beat the foe,
Despite continual loss of life
Of those confronting all the strife.
But strange! His enemies were sure
That Allah would their cause secure.
So God to God and wish to wish
The conflict grew more feverish.
And back at home the leader found
Himself on much more shaky ground,
And world opinion, never sure
He really had the grounds for war
Began to further criticize
His too aggressive enterprise.
(As still ongoing was the strife
With still ongoing loss of life).
And God and Allah seem, to date,
Not sure which side to vindicate.
And so men’s own reality
Ignores that it’s their vanity
That is at root the primal cause.
This makes us think and gives us pause.
For men in highest places show
How vain beliefs can bring us low.
And those our leaders who are prone
To wish for things we can’t condone,
Believing they are in the right,
Might look up at the sky at night.
To wish upon a star is nice
Less likely to elicit vice,
Corrupt belief and common sense
Or make ambition too intense.
(And Judy Garland did endorse
The great celestial resource)
But when as president they act
They’d better base beliefs on fact.
The truth will out, and leaders who
Ignore it, they should exit too.
As I have often said, you don’t need to be a scientist to see that most alternative medicine is bunk, though it is bunk that is supported and propagated by an enormously wealthy industry..
There were two good examples this week, John Sutherland, who was until recently professor of English literature at UCL, understands it very well. And so does political columnist, Polly Toynbee.
“Complementary and Natural Healthcare Council”
Polly Toynbee’s column, “Quackery and superstition – available soon on the NHS“, was prompted by the announcement in The Times that the government was to set up a “Natural Healthcare Council”. It was soon renamed the “Complementary and Natural Healthcare Council” (CNHC) It was instantly dubbed ‘OfQuack’ in an admirable analysis by quackometer.a>
The very name is tendentious and offensive to any thinking person. What is “natural” about sticking needles in yourself, or taking homeopathic polonium?
Toynbee comments
“Put not your trust in princes, especially not princes who talk to plants. But that’s what the government has decided to do. The Department of Health has funded the Prince of Wales Foundation for Integrated Healthcare to set up the Natural Healthcare Council to regulate 12 alternative therapies, such as aromatherapy, reflexology and homeopathy. Modelled on the General Medical Council, it has the power to strike therapists off for malpractice.”
There was only one thing wrong in this article. Toynbee says
“The alternative lobby replies that conventional medicine can also do more harm than good. They chortle with glee at an article in the Lancet suggesting there is no scientific evidence for the efficacy of 46% of conventional NHS treatments. But that’s no reason to encourage more of it.”
Professor John Garrow has pointed out (see, also Healthwatch )
“It is true they chortle, but they have got their facts wrong. The 46% of treatments which are not proven to be effective is 46% of all treatments for 240 common conditions – and very few are used in the NHS. The great majority are treatments used by alternative practitioners. “
The unconstitutional interference by the Prince of Wales in public affairs has been noted often before, and it seems that it’s happening again.
For example, there is the TV programme, “Charles, the Meddling Prince”, or, for a US view, see “Homeopathy: Holmes, Hogwarts, and the Prince of Wales“. And then there’s Michael Baum’s superb “An open letter to the Prince of Wales: with respect, your highness, you’ve got it wrong“.
It isn’t that regulation isn’t needed, but that the sort of regulation being proposed won’t do the trick. The framework for the “Natural Healthcare Council” has been set up by Professor Dame Joan Higgins, and it seems to be very much along the lines proposed by the Prince of Wales. Here’s what’s wrong.
| Professor Dame Joan Higgins (Jan 10th) says “Complementary therapists have been in practice for many years” and “If complementary therapy is not to be banned, is it not, therefore, wise to regulate it and offer the public some measure of protection”. That’s fine, but I think the sort of regulation that she, and the Prince of Wales, are proposing won’t do the trick. We don’t need new laws, or new quangos, just the even-handed application of existing laws. Homeopathic arnica 30C contains no arnica, and one would expect that the Office of Fair Trading would have banned it. It is no different from selling strawberry jam that contains no strawberries. But absurd legal loopholes make homeopaths immune to prosecution for this obvious mislabeling, whereas jam fraudsters would be in deep trouble. The Advertising Standards Authority, likewise, is prevented from doing its job by legal loopholes, and by the fact that it has no jurisdiction over web advertising, which is now the main source of untrue claims. If alternative medicine advocates had to obey the same laws as the rest of us, the public would be better protected from fraud and delusion. What won’t work is to insist that homeopaths are “properly trained”. If one takes the view that medicines that contain no medicine can’t work, then years of being trained to say that they do work, and years spent memorizing the early 19th century mumbo-jumbo of homeopathy, does not protect the public, it imperils them. |
The “Natural Healthcare Council” isn’t the only example either. Try Skills for Health.
Skills for Health
This appears to be a vast bureaucratic enterprise devoted to HR-style box-ticking. Just in case you don’t know about this latest bit of HR jargon, there is a flash movie that explains all.
“Competences are descriptors of the performance criteria, knowledge and understanding that are required to undertake work activities. They describe what individuals need to do, and to know, to carry out the activity -regardless of who performs it.”
That sounds OK until you realise that no attention whatsoever is paid to the little problem of whether the “knowledge and understanding” are pure gobbledygook or not. It’s rather like the HR form that ensures UCLH that you are a fully-qualified spiritual healer “Laying on of hands: just tick the box“.
It is an invidious insult to human intelligence to suppose that exercises like this are an appropriate way to select people for jobs. They have precisely the opposite effect to that intended.
An indication of the level of their critical thinking is provided what is written about the 62 items listed under “Complementary Medicine” These include “CHH5 Provide Healing”.
“This workforce competence is applicable to:
- healing in the presence of the client
- distant healing in contact with the client
- distant healing not in contact with the client
Both healing in the presence of the client and distant healing use exactly the same mental and spiritual processes. Clearly, however, distant healing does not involve many of the physical aspects of healing in the presence of the client. The performance criteria have been written so as to be able to be interpreted for use in any healing situation.
The workforce competence links to CHH6 which is about evaluating the effectiveness of the healing.”
It also includes homeopathy, for example “HM_2: Plan, prescribe and review homeopathic treatment“.
I sent an email to Skills for Health to ask who wrote this stuff. A reply from their Technical Development Director failed to elicit any names.
| We develop competences to fit sector needs and demands. When that need is moved into a competence project we establish a number of groups from the specific area to work with us to develop the competences. One of these groups is a “reference” group which is made up of experts from the field. In effect these experts give us the content of the competences, we write them in our format. So I guess the answer as to who is the author is Skills For Health, but with more complexity behind statement.Please do not hesitate to get in touch with me for further clarity. |
A conversation with Skills for Health
I did want more clarity, so I phoned Skills for Health. Here are some extracts from what I was told.
“It’s not quite as simple as that”
“the competencies on our data base are written by “experts in the field”
DC. Yes and it is their names that I was asking for
“I’m not sure I can give you the names . . . We’re starting to review them in the New Year. Those competencies are around six years old. ”
“We are working with the Prince’s Foundation for Integrated Health [FIH] via Ian Cambray-Smith to review these competencies, all the complementary therapy competences on our web site”
“They are written as a consensus decision across a wide number of stakeholders across that area of …”
DC. Written by whom though?
“written by a member of Skills for Health staff or a contractor that we employ simply to write them, and the writing is a collation of information rather than their original thoughts, if you like”
DC yes, I still think the sources can and should be given.
“FIH didn’t spend any money with us on this project. This project was funded by the Education act regulatory bodies, QCA, the Qualifications and Curriculum Authority . . . ”
“They [FIH] may well have put in and supported members of their professions or groups to do part of this . . they were there as experts on that particular area of complementary therapy ”
DC it’s their names that I was after
“There may well have been members [of FIH] on the reference groups that I’ve referreed to who are members of the FiH . . .they were there as experts from that area of complementary therapies.”
DC Oh, and are the names of [the people on] these reference groups published?
“No they are not published”
DC ah, why not?
“We do not consider it necessary”
DC Well, I consider it very necessary myself
“Tell me why”
DC It’s a question of public accountability
“I guess the accountability lies with us as the owners of those competencies”
DC Uh I’m afraid your bureaucratic jargon is a bit much for me there. “The owners of those competencies”? I’m not sure what that means
“Why do you want the information?”
DC haha, well if you want me to be entirely blunt, it’s because I’m appalled that this black magic is appearing on a government web site
“. . . can I say that as an organisation funded by a number of sources, one being Department of Health England, none of our work condones the practice you’ve just suggested. Our work supports best practice in areas that are evidence- and research-based”
DC Ah would you mind pointing me to the evidence for homeopathy and distant healing?
“Uh [pause] there is [pause]”
DC Yes, go on
“Well homeopathy is a contentious issue, because every newspaper article I read seems to suggest that homeopathy, in itself, is not an appropriate, uh, not an, uhm, appropriate, uh, therapy.”
DC Yes so why are you laying down standards in it?. You know I’m curious. I’m genuinely curious about this
“The areas involved in them have asked us to, including the Prince’s Trust hence the reason we are doing . . .”
DC But the Prince’s Trust is not part of government. Ha, it behaves as though it was , I agree, sometimes but it is surely for the Department of Health to ask you to do these things, not the Prince of Wales.
“We cover the whole health sector.. We don’t purely work for, or are an organisation of, the Department of Health.”
DC. I’m very baffled by the fact that you say, you very accurately the research on homeopathy, namely that it doesn’t work, but you are still setting standards for it. It’s quite baffling to me.
“Working with the Foundation for Integrated Health, as we are doing, homeopathy is one of the 10 areas that is listed for regulation by FIH ”
DC. Well yes the Prince of Wales would like that. His views on medicine are well known, and they are nothing if not bizarre. Haha are you going to have competencies in talking to trees perhaps?
“You’d have to talk to LANTRA, the land-based organisation for that.”
DC. I’m sorry, I have to talk to whom?
“LANTRA which is the sector council for the land-based industries uh, sector, not with us sorry . . . areas such as horticulture etc.”
DC. We are talking about medicine aren’t we? Not horticulture.
“You just gave me an example of talking to trees, that’s outside our remit ”
After explaining that talking to trees was a joke, the conversation continued
DC So can I clarify then? Who is it that said you must include these fairly bizarre things like distance healing and homeopathy? Who decides whether it goes in?
“We did”
“We are going to do a major review. We are doing that review in partnership with the FiH and the awarding bodies that award the qualifications that are developed from these competencies”
“When that need is moved into a competence project we establish a number of groups from the specific area to work with us to develop the competences. One of these groups is a “reference” group which is made up of experts from the field. In effect these experts give us the content of the competences, we write them in our format.”
Conclusions from this dialogue
We still don’t know the names of the people who wrote the stuff, but a Freedom of Information Act request has been submitted to find out
The Skills for Health spokesperson seems to a a bit short of a sense of humour when it comes to talking to trees.
The statement that “Our work supports best practice in areas that are evidence- and research-based” is not true, and when pressed the spokesperson more or less admitted as much.
Most importantly, though, we do now know that the revision of this gobbledygook will be carried out entirely by the Prince’s Foundation for Integrated Health and the people who set exams in the relevant form of gobbledygook. No critical voice will have an input, so don’t expect much improvement. “We are working with the Prince’s Foundation for Integrated Health [FIH] via Ian Cambray-Smith to review these competencies”. And in case you don’t know about the medical expertise of Ian Cambray-Smith, it is described on the FIH web site. He is the FIH’s Health Professionals Manager.
 |
Ian Cambray-Smith acts as the focus for FIH’s involvement with healthcare professionals. He works collaboratively to develop a range of work programmes, policies and initiatives to support healthcare professionals and help them to deliver a truly integrated approach to health. Ian’s background is in plastics research, project management and business development; he has an MSc in polymer technology. He joined the Foundation in 2006. |
The press releases (STOP PRESS)
Uhuh, here we go again.
All over the media we see headlines like “Honey ‘beats cough medicine’ “.
Take for example, the Daily Telegraph, where Ben Farmer writes “Honey is better at treating children’s coughs than an ingredient used in many over-the-counter medicines, according to new research”.
That is NOT what the research found This is what the research paper itself says (DM refers to the standard ‘cough suppressant’ dextromethorphan, which is already known to be ineffective).
| “honey was significantly superior to no treatment for cough frequency’ DM was not better than no treatment for any outcome. Comparison of honey with DM revealed no significant differences.” |
See it? No detectable difference between honey and standard cough medicine.
Everyone in the media misinterpreted what the paper said, but at least one blogger is already on to it, with Today’s “duh” study is a honey”.
At first sight, the results seem contradictory, No difference between honey and DM, No difference between DM and ‘no treatment’. So how can honey be better than ‘no treatment’?
The study was by Ian M. Paul, MD, MSc; Jessica Beiler, MPH; Amyee McMonagle, RN; Michele L. Shaffer, PhD; Laura Duda, MD; Cheston M. Berlin Jr, MD, published in Archives of Pediatrics & Adolescent Medicine 2007, 161, 1140 – 1146.
What was done
The design of this trial was pretty good apart from one thing Three things were compared (a) buckwheat honey, (b) a standard ‘cough suppressant’, dextromethorphan in a honey-flavoured syrup that was designed to be similar to the honey (DM for short), and (c) no treatment whatsoever.
The median age of the children who completed the study was 5.2 years (range, 2.2 – 16.9 years). They all had coughs attributed to upper respiratory tract infection. Thirty-five patients received honey, 33 received DM, and 37 received no treatment.The good thing is that the treatments were allocated randomly to the children, and that the person doing the assessment didn’t know which treatment each child had received. The children didn’t know whether they were getting honey or DM either, but they DID know when they got ‘no treatment’. The trial was carried out over two days. On day one nobody got a treatment, but they filled in a survey that asked, for example, “How frequent was your child’s coughing last night”. The parent had to tick one of seven boxes, from ‘not at all’ (score zero) to ‘extremely’ (score 6). They were then given the treatment allocated to them in a brown paper bag, so the person who gave it didn’t know which it was. The patients then went home and on the next day the same survey was completed by the same parent, over the telephone.
What happened?
First look at the raw data. Here is Figure 2 from the original paper.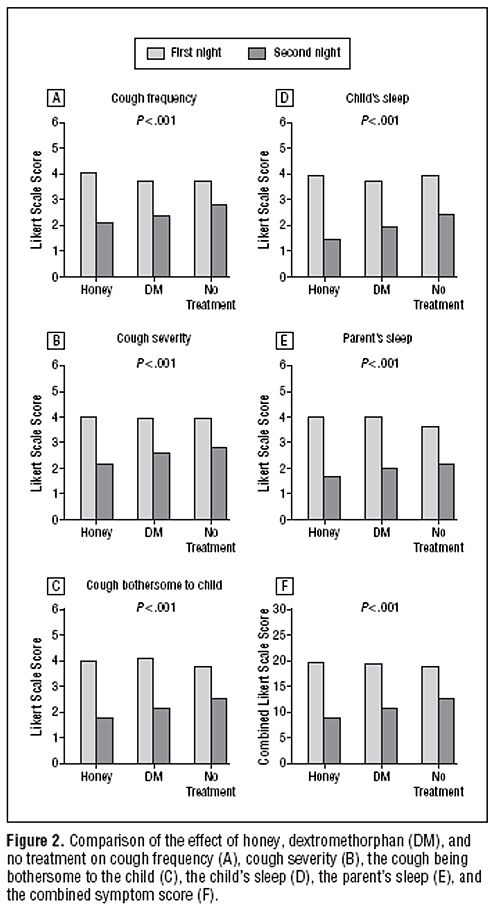 The charts show the results for 5 different measures of the severity of cough, and the last chart (F) shows the aggregate score for all the criteria.
The charts show the results for 5 different measures of the severity of cough, and the last chart (F) shows the aggregate score for all the criteria.
The first thing to notice is that there are no error bars on these charts. In my area, at least, no journal would accept a chart like this with no indication of scatter. There is a snag, though. Each patient acts as his/her own control, and that would not be reflected properly if errors bars were calculated for the numbers plotted in Fig. 2. It would therefore have been better to have a chart in which the difference in score between day 1 and day 2 was calculated from each patient, and the size of these differences plotted, with a standard deviation of the mean to indicate the amount of scatter in the observations. I have asked Dr Paul to send me a version that indicates the scatter of the numbers in this way (but I don’t think it will come).
The second thing to notice is that there is there is quite a big difference between the score on the first day (pale columns) and on the second day (dark columns), even in the no treatment group .
Thirdly, the pale columns are all much the same. On the first day the average score was about 4 (“a lot”) though on the second day, even with no treatment, the score fell quite a lot, to something between 2 (“a little”) and 3 (“somewhat”). This is a bit baffling because no treatment was given on either day. Presumably it results from the different settings in which the survey was given, or because the kids were getting better anyway.
Fourthly, insofar as the pale columns (baseline values) are all much the same, the thing you need to concentrate on is the difference, on each chart, between the height of the dark bars, for honey, DM and no treatment. These differences are pretty small, but on all the charts, the honey score is slightly smaller than the DM score, and the DM score is slightly smaller than the ‘no treatment’ score. What are we to make of that?
Here beginneth the statistical lesson.
Because the differences are small, and the scatter is quite big, we have to ask whether the differences are just random fluctuations rather than a result of any real difference between the treatments. That means we need statistics. Here is how the statistical argument works. Put roughly, we ask “how probable is it that the observations could arise by chance”. More precisely, the question is this. If there were no difference between the treatments, what is the probability that we would observe by chance a difference as big as, or bigger than, that seen in the experiment? (You need the subjunctive mood to explain statistics -pity it’s vanishing.)
Above each chart in the Figure we see P < 0.001. This means that there is less than a one in 1000 chance of the results arising by chance. More precisely, if all three treatments (honey, DM and no treatment) were actually identical, it is very unlikely that we’d see these results. The reasonable conclusion is, therefore, that all three treatments are not identical. The problem with this argument is that it tells you nothing about where the differences lie, so it is of no help whatsoever to a patient who is trying to decide what to do about a cough. The other problem is that it includes the ‘no treatment’ group, which was not blind. Both the children and parents were well aware that no treatment was given.
The most helpful comparison is really the properly-blinded comparison between honey and DM. And when this was looked at the result was no significant differences. In other words the small differences between the heights of the dark columns for honey and DM could perfectly well have arisen by chance if honey and DM were identical in their properties.
There isn’t any reason at all to think that honey is better than the standard (but ineffective) cough medicine.
The direct comparison between DM and ‘no treatment’ also shows no significant difference. Yet there are signs of a real difference between ‘no treatment’ and honey, though only for the cough frequency, not the other four measures. The aggregate measure (F in the figure) gave P = 0.04 for the comparison, so the authors are running a risk of 1 in 25 of being wrong in claiming a real effect. Although some people seem to regard a value of P = 0.05 as indicating a real effect, the fact that you’ll make a fool of yourself 1 time in 20 by claiming a real effect when none exists has never seemed to me to be good enough odds to stake one’s reputation on.
The ‘no treatment’ group certainly has some interest, but the fact that it was not blind means that the fact that honey was marginally better than ‘no treatment’ could perfectly well mean that taking honey has a better placebo effect that doing nothing at all. It provides no evidence at all that honey has any genuine therapeutic effect. If it had, one would then have to find out if the therapeutic effect was specific to buckwheat honey, or whether any old honey would do. It could be argued that even if the effect were real rather than placebo, the size of the effect is too small to make all that effort worthwhile.
A couple more things
It is already well known, from several good studies, that DM is useless, no better than placebo. This inconvenient fact has not yet reached many places that it should have (not even mentioned on wikipedia for example), but the American Academy of Pediatrics says
“Numerous prescription and nonprescription medications are currently available for suppression of cough, a common symptom in children. Because adverse effects and overdosage associated with the administration of cough and cold preparations in children have been reported, education of patients and parents about the lack of proven antitussive effects and the potential risks of these products is needed.”
The discussion in the paper by Paul et al, seems surprisingly upbeat about honey, in the light of their own findings. I’m surprised that they use the term ‘demulcent’ which I had thought to have died out, like the word ‘tonic’, on the grounds that it had no defined meaning
It is because meaningless terms and useless medicines die out eventually that medicine makes progress. The problem with alternative medicine is that nothing dies out: on the contrary they keep adding myths.
And finally
Always look at the end of the paper. On this one we see that the study was paid for by the National Honey Board. Dr Paul assures me that the funding source had no say in the design or analysis, which is as it should be.
Financial Disclosure: Dr Paul has been a consultant to the Consumer Healthcare Products Association and McNeil Consumer Healthcare.
Funding/Support: This work was supported by an unrestricted research grant from the National Honey Board, an industry-funded agency of the US Department of Agriculture.
So what is the practical outcome?
My conclusion from all this is simple. If you have got a cough, tough luck. There isn’t really anything available, conventional or alternative, that does much good. You’ll just have to wait for it to get better. But if you want to take something that tastes nice, why not honey? It almost certainly won’t do any good but it tastes good and it’s safer than the standard cough medicine.
The sponsor’s interpretation
It seems that the sponsor of the work is happy with the misinterpretation.
Charlotte Jordan a project manager of research at the National Honey Board, believes the finding confirms what your grandmother told you.
“This is a really exciting finding,” she said. “For a long time it’s been folklore medicine to use honey when you have a cough or a cold, but it’s exciting to have a scientific study to back that up.”
Just one problem, That is NOT what the paper says.
How did all this mis-reporting happen?
One reason is misleading press releases. Universities and Academic journals now engage in shameless PR, spin and hype. They prostitute good science.
Download press releases from Penn State, JAMA and Press Association [pdf file]
Here is the highly misleading bit of hype that came from the Press Office of the Pennsylvania State University. The headline is “Honey a better option for childhood cough than OTCs” (OTC means over-the-counter medicines that contain DM). That contradicts directly the paper which says “Comparison of honey with DM revealed no significant differences”.
Likewise the statement in the Penn State release “Honey did a better job reducing the severity, frequency and bothersome nature of nighttime cough from upper respiratory infection than DM or no treatment” is equally incompatible with “Comparison of honey with DM revealed no significant differences”. Its only possible justification is from the 3 way comparison by analysis of variance and that does not tell us what we need to know.
To make matters worse, the media office is not to blame this time. Ms Manlove told me tonight that the press release had been approved by Dr Paul himself.
| Contact: Megan W. Manlove Penn State Honey a better option for childhood cough than OTCs A new study by a Penn State College of Medicine research team found that honey may offer parents an effective and safe alternative than over the counter children’s cough medicines. The study found that a small dose of buckwheat honey given before bedtime provided better relief of nighttime cough and sleep difficulty in children than no treatment or dextromethorphan (DM), a cough suppressant found in many over-the-counter cold medications. Honey did a better job reducing the severity, frequency and bothersome nature of nighttime cough from upper respiratory infection than DM or no treatment. Honey also showed a positive effect on the sleep quality of both the coughing child and the child’s parents. DM was not significantly better at alleviating symptoms than no treatment. . . . |
All that Candice Yakel, of the Office for Research Protections at Penn State had ro say in the matter was
“Our investigators stand by the conclusions of the study as reported in the Archives of Pediatric and Adolescent Medicine and as characterized in our press release of December 3, 2007.”
And here is the equally misleading bit of hype issued by the Journal of the American Medical Association (Ms Manlove tells me that this was also approved bt Dr Paul).
| JAMA and Archives Journals Study suggests honey may help relieve children’s cough, improve sleep during colds
|
The Press Association release was equally bad, and probably the one used by many of the reporters as a basis for stories in the media. The opening statement is totally wrong.
| 1 HEALTH Honey Embargoed to 2100 Monday December 3 HONEY BEST FOR KIDDIES’ COUGHS SAY RESEARCHERS By John von Radowitz, PA Science Correspondent Natural honey is a better remedy for children’s coughs than expensive over-the-counter medicines, researchers said today. A dose of buckwheat honey before bedtime easily outperformed a cough suppressant widely used in commercial treatments, a US study found. . . . |
Follow-up
There is a review of over-the-counter cough medicines in the BMJ (2002) [free full text]. It concludes “Recommendation of over the counter cough medicines to patients is not justified by current evidence”.
Here is an interchange of letters from this week’s BMJ. George Lewith says more money should be spent by the government on research on alternative medicine. Well, only if it is spent properly, and that is not what has happened in the past. (Letters here, if you have a subscription.)
In all probability money spent in this way would be money down the drain, just as it has proved to be in the USA. As pointed out by Wallace I. Sampson, M.D., NCCAM has spent almost a billion dollars on research into alternative medicine, and
“. . it has not proved effectiveness for any “alternative” method. It has added evidence of ineffectiveness of some methods that we knew did not work before NCCAM was formed.”
It is a bottomless pit, and there are more promising ways to spend the money.
|
||||
| George T Lewith, Reader in Complementary Medicine, University of Southampton Primary Medical Care, Aldermoor Health Centre, Southampton SO16 5ST Send response to journal: Re: Valuing Research |
I remain unclear about John Garrow and David Colquhoun’s position with respect to “funding CAM”. Are they suggesting that there should be no funding for CAM research or are they suggesting this embargo should apply to the provision of CAM services within the NHS? If the former, how do they justify this position with respect to the many UK taxpayers who use CAM each year and for whom the government has some obligation to provide information? Competing interests: None declared |
|||
|
||||
| John S. Garrow, vice-chairman HealthWatch The Dial House, Rickmansworth, WD3 7DQ Send response to journal: Re: Taxpayer funding of CAM research |
Dr Lewith wants clarification of my view about public funding of CAM research. It has changed over the last 7 years. In 2000 the House of Lords Select Committee (HLSC)advised the Department of Health to fund research on acupuncture, chiropractic, herbal medicine, homeopathy and osteopathy to see if these therapies were safe, more effective than placebo and good value for money, At the time I supported this decision. However in 2003 it was disclosed that £1.3m had funded 8 research projects, at the Universities of Leeds, Southampton, Bristol, Brunel, Sheffield and York, but none of these were directly testing the safety, efficacy or value-for- money of the main CAM therapies.[1] I noted that these Universities did not have as good a record of research into the efficacy of CAM as Exeter, which had applied but failed to get funding. It was also noticable that the panel awarding the grants tended to work at the funded Universities. CAM research is not so impoverished as Dr Lewith implies. The onus is now upon the researchers who received £1.3m from the taxpayer, and more from the Foundation for Integrated Health, to tell us what answers they have found to HLSC’s very pertinent questions. Only in the light of these answers can we judge if they deserve further public funding. If initially the Government had an “obligation” to fund CAM research I think the £1.3m discharged it, and now there is an obligation on CAM practitioners to show that they have not misappropriated these funds. [1]Garrow JS et al. UK government funds CAM research. FACT 8:397-402, 2003 Competing interests: None declared |
|||
|
||||
| David Colquhoun, Prof of Pharmacology UCL Send response to journal: Re: Funding for alternative medicine research |
I agree entirely with John Garrow’s response. A corollary of his analysis is that, if there is to be any more funding for research in alternative medicine, it is essential that the allocation of the money should not be in the hands of alternative medicine people. The reason for that is that past experience has shown that they will give the money to projects that don’t answer the real questions. If no applications are received that address the proper questions with rigorous experimental design then the money should be clawed back and spent on something that has a better chance of being a real advance. I am perpetually amazed by the reluctance of advocates of alternative medicine to subject their claims to proper tests. The only interpretation that I can see of this failure is that they themselves believe, deep down, that the tests would be failed. I hope that isn’t the explanation though, because if they were convinced that the tests would fail, it would mean that we are dealing with fraud, not just delusion. Competing interests: None declared |
|||

If you read nothing else on the topic, read Ben Goldacre’s best ever piece, A Kind of Magic? (Guardian, 16 Nov 2007). This started as response to “In defence of homeopathy” in the same newspaper on 13 November. On the same day, the Lancet carried a rather more academic piece by Goldacre “Benefits and Risks of Homeopathy” , The same issue of the Lancet carried a commentary ” Pressure grows against homoeopathy in the UK“, as well as a sadder report, “Homoeopathy booming in India“.
There is going to be plenty of commentary on these pieces. There is one bit of “A Kind of Magic” that is particularly important, and that is about how to do a proper trial. It is one of the most persistent myths of all sorts of quack that, for reasons that are never explained, their particular form of magic is not susceptible to being tested in the normal and well-established way. This is simply not true, and the fact that the myth is repeated again and again is perhaps the best reason to doubt that homeopaths are really genuine in the beliefs that they claim to have. If they were really so confident they would do the tests. But they don’t and won’t. When the government supplied money for doing tests, the money was distributed by a committee of “experts in alternative medicine” (though it beats me how you can be an ‘expert’ in something that isn’t true), all the money was given to projects that were incapable of answering the main question, namely ‘does it work better than placebo?’.
How to do the test
Here is Goldacre’s description of how to do the test. It has been said before, but it must be said again and again. Until homeopaths take this seriously, there is no option but to regard them as frauds.
“You could do a randomised, controlled trial on almost any intervention you wanted to assess: comparing two teaching methods, or two forms of psychotherapy, or two plant-growth boosters – literally anything. The first trial was in the Bible (Daniel 1: 1-16, since you asked) and compared the effect of two different diets on soldiers’ vigour. Doing a trial is not a new or complicated idea, and a pill is the easiest thing to test of all.
Here is a model trial for homeopathy. You take, say, 200 people, and divide them at random into two groups of 100. All of the patients visit their homeopath, they all get a homeopathic prescription at the end (because homeopaths love to prescribe pills even more than doctors) for whatever it is that the homeopath wants to prescribe, and all the patients take their prescription to the homeopathic pharmacy. Every patient can be prescribed something completely different, an “individualised” prescription – it doesn’t matter.
Now here is the twist: one group gets the real homeopathy pills they were prescribed (whatever they were), and the patients in the other group are given fake sugar pills. Crucially, neither the patients, nor the people who meet them in the trial, know who is getting which treatment. ”
Winterson and the Maun Project and AIDS
This particular round of discussion was started by Jeanette Winterson’s “In defence of homeopathy“.
It is an interesting article because, like the whole world of homeopathy, Winterson herself is split between homeopathy as a harmless placebo and homeopathy as a dangerous “treatment” for dangerous diseases. On one hand she claims that she is all for proper anti-retroviral treatment of AIDS, yet at the bottom of the article it says “Jeanette Winterson is donating the fee for this article to the Maun homeopathy project. ” .
“Since 2002, The Maun Homeopathy Clinic has been running free homeopathy outreach clinics in Maun, a fast growing town in the north of Botswana, where over 35% of the people are infected with HIV or AIDS, one of the highest rates in the world.”
Hilary Fairclough, much praised by Winterson for reducing her high temperature with pills that (didn’t contain) any snake venom, describes herself as “clinical director” of the Maun project. She is, of course, qualified in neither science nor medicine, but is registered with the now notorious Society of Homeopaths. The Maun project newsletters have all the usual accounts of amazing cures. They quote
“The homeopaths are so loved here, and at the clinics we see daily miracles.”
Do they really believe in miraculous cures? I’m inexorably reminded of an earlier generation of missionaries who went to Africa, to impose on the poor benighted natives a different brand of irrationality. At least the missionaries did some education too, and didn’t, on the whole, kill people.
The ladies of Devon who contribute their money to this project, rather than proper treatment, are, sadly, contributing to the gentle art of homeopathic killing.
Referring to Goldacre’s article in the Lancet, Winterson says ” where is the scientific sense is saying that because we don’t understand something, even though we can discern its effects, we have to ignore it, scorn it, or suppress it?”. Needless to say, no pharmacologist has ever said anything of the sort. Quite the opposite. Goldacre comments
“The article does not say that, and I should know, because I wrote it. It is not an act of fusty authority, and I claim none: I look about 12, and I’m only a few years out of medical school. “
Winterson’s article goes on about ” boosting the patient’s immune system so they are better able to fight off the opportunistic viruses that follow behind HIV”.
Sorry, but there is not the slightest reason to think the sugar pills do anything whatsoever to the immune system: that is no more than a ritual form of words, a mantra recited by every homeopath.
Winterson also falls for the latest fashion in homeopathic gobbledygook, to describe it as nanopharmacology. It isn’t nano, it’s zero.
She also gives support, though it is intriguingly ambivalent, to the forthcoming conference of the Society of Homepaths, You can download the flyer for this conference, It defies belief. As well as Winterson’s homeopath, Hilary Fairclough, it features Harry van der Zee and Peter Chappell.
“Harry believes that using the [Chappell’s] PC1 remedy, the AIDS epidemic can be called to a halt, and that homeopaths are the ones that can do it. “
That is a direct claim for a cure. It is as good example as any of the Gentle Art of Homeopathic Killing, in the now immortal words of the quackometer blog.
Peter Chappell’s web site says (no, really, seriously),
“Right now AIDS in Africa could be significantly ameliorated by a simple tune played on the radio across Africa. Or there is a slower solution using pills, and drops that works very well, but is harder to deliver. ”
“The second creative idea is again is implied by those above, and relates to the ability to deliver healing aurally, instead or orally, so healing downloads and ehealing is possible and practical. Instead of taking pills containing resonance information, you listen to a very short piece of music which contains the same information. “
Just beat that, if you can.
You can get free samples here. Try the tuberculosis tune. Sounds like pretty standard 50s or 60s jazz (anyone recognise it?). Don’t be fooled though. It’s explained that
The music is not the download
The music is simply the carrier and alerts you to listen. The download is engrafted on the music by a special process. That is the new technology.
University of Westminster: a new course?
I hope that the University of Westminster is proud of the fact that its degree in homeopathy is recognised by the Society of Homeopaths , who are sponsoring this nonsense. Perhaps the university should consider an advanced third year module in “downloading therapeutic resonance music”.
Read more
Andy Lewis’s quackometer “Will Homeopathy and iTunes Cure AIDS?
Nick Cohen “The cranks who swear by citronella oil”
Jeremy Laurance in the Independent (17 Nov) “Homeopathic treatment of Aids attacked by medics“
| A paper published in the Postgraduate Medical Journal, October 2007, has been reported widely. In the same issue there was a commentary by Edzard Ernst. They show the astonishingly poor evidence than herbal treatments work, despite the fact that they have been around for thousands of years. They looked at 1330 published trials on herbal medicines and found 3 (yes three) that stood up to scrutiny, Of those three, two were negative and one indecisive |  Red clover, Derwentwater. |
A systematic review of randomised clinical trials of individualised herbal medicine in any indication, R. Guo, P. H. Canter, and E. Ernst, Postgrad Med J 83: 633-637 [Get the reprint]
Herbal medicine: buy one get two free, E. Ernst, Postgrad Med J 83: 615-617 [get the reprint]
Grab the reprints before I am told to remove them.
The paper says
“Systematic searches of electronic databases and contacting
experts and professional bodies in the field resulted in the
location of only three randomised clinical trials of individualised
herbal medicine. It should be stressed that professional
bodies representing the interests of different practitioner
factions from around the world were unable to contribute any
more studies than this. In view of the long history and
widespread use of medical herbalism, Chinese herbal medicine
and Ayurvedic herbal medicine in many and diverse indications,
this should be a cause for concern. It indicates that
individualised herbal medicine has an extremely sparse
evidence base and that there is no convincing evidence
supporting its use in any indication.”
The National Institute of Medical Herbalists says
“More and more people are turning to herbal medicine as a kinder alternative to mainstream medicine, with its over reliance on pharmaceutical products.”
Wrong. Herbal medicines are pharmaceutical products. They are just unstandardised, and often impure and contaminated, pharmaceutical products.
In the Guardian we find Ann Walker quoted thus.
“Ann Walker, director of the British Herbal Medicines Association, insisted that most herbalists were well-trained and knew when to refer patients. She said herbalists took a three or four-year degree course before accreditation.
She acknowledged the lack of proof of efficacy for individualised herbal medicine. “The evidence is scanty because the studies have only recently been started,” she said. This did not mean there was no efficacy.”
Just a thought: shouldn’t you have some evidence that they work before you start selling them? These things have been around for thousands of years but the “studies have only recently been started”. You couldn’t make it up. You can’t have a high level of training if there is no evidence. The paucity of trials makes it very hard to know how you can fill up a three or four year course with anything but idle speculations. Universities should not being giving degrees in idle speculation.
Quote of the day. . Of all the pathetic defences offered by herbalists, this one, quoted in the Daily Mail, is my favourite.
“Jane Gray, of the National Institute of Medical Herbalists, said: “We would challenge the conclusions reached by this study based on such little data.”
“We want more research, but we’re all in private practice and cannot afford to stop earning to run a trial over several months.”
The fact that there is “so little data” is the conclusion. And perish the thought that a herbalist should “stop earning” just in order to find out whether what they are selling does any good.
The regulation scam
Alison Denham, speaking for the National Institute of Medical Herbalists, is quoted as saying
“But there are certainly issues around the expertise of practitioners which need to be addressed, and we look forward to government regulation which imposes a high standard of training on anyone who wants to register.”
Like all forms of alternative medicine, herbalists are desperate for government “regulation” because they know it gives the appearance of official approval without requiring them to show that they can do the slightest good.
Reports on this paper
The BBC web site: “Tailored herbal medicine ‘futile'”.
The Guardian report, by Sarah Boseley, is pretty good. “Herbalists’ cocktails may do more harm than good, say researchers.”
- Call for individualised remedies to be banned
- Little evidence to support claims of efficacy
The Times has another excellent report by Nigel Hawkes. “High street herbalists can offer no evidence that their remedies work”
The Independent. “Natural medicine on trial: The trouble with herbs. Traditional herbal remedies have never been more fashionable: sales have almost doubled in eight years. There’s just one problem: science suggests that they don’t work.”. This time Jeremy Laurance got the headline right (unlike the acupuncture piece). But where did that list of “Herbal remedies that work” at the end come from? Had he checked the Cochrane Reviews? I think not.
The Daily Mail. “Herb cures that ‘do you more harm than good’ “. Pretty good report. specially for the Daily Mail.
The Scotsman. “A natural cure?” Lyndsay Moss. Sadly, and unusually, this is the only really poor report. Just look at the end of it.
Postscript
On Saturday morning (6 October) I did an interview on the Dublin radio station, Newstalk. The host, Brendan O’Brien spoke also to Mary Plunkett, from the Professional Register of Traditional Chinese Medicine. She assured us that that, although there may be no evidence that it works published in the West, there were lots written in Chinese. What a pity that I had not yet read Ben Goldacre’s column, on this week’s bad news for herbalists. He cited a reference that was new to me.
You can read the abstract here. [download pdf]. The paper, by Vickers, Niraj, Goyal, Harland and Rees (1998, Controlled Clinical Trials, 19, 159-166) has the title “Do Certain Countries Produce Only Positive Results? A Systematic Review of Controlled Trials”. The conclusion is riveting.
“In the study of acupuncture trials, 252 of 1085 abstracts met the inclusion criteria. Research conducted in certain countries was uniformly favorable to acupuncture; all trials originating in China, Japan, Hong Kong, and Taiwan were positive, as were 10 out of 11 of those published in Russia/USSR. In studies that examined interventions other than acupuncture, 405 of 1100 abstracts met the inclusion criteria. Of trials published in England, 75% gave the test treatment as superior to control. The results for China, Japan, Russia/USSR, and Taiwan were 99%, 89%, 97%, and 95%, respectively. No trial published in China or Russia/USSR found a test treatment to be ineffective.”
One of the effects of this affair has been the posting of some critical examinations of some of the writings of Dr Ann Walker. I make no comment. The links are here.
This item appeared originally on the old IMPROBABLE SCIENCE page
The reversal of UCL’s request to remove this page from UCL’s server was, in large part, the result of the power of the blogosphere. Here are some of the things that did the trick.
“Moved to tears by the beauty of blogs”. Goldacre wraps up the affair in the Guardian, and on badscience.net (“Stifling Debate – When Bloggers Attack”).
He gives links to the close examination of the work of Dr Ann Walker that that is now appearing.
“UCL have just issued a smashing statement on Prof Colquhoun’s de-excommunication.” Comment from badscience.
This episode seems to have sparked a close inspection of some of the claims made by Ann Walker. Here are some examples.
“Dr Ann Walker and Her Neanderthal Theories”. An analysis of Walker’s theory about the Neanderthal diet, on the quackometer blog. Goldacre comments
“In one piece, Walker promotes the idea that neanderthals were not a distinct kind of human, but degenerate and malnourished versions of ordinary humans: buy pills or regress to a sub-human state, seems to be Walker’s message. Yikes.”
“Ann Walker festival: “There is no convincing evidence that Ginkgo biloba is efficacious for dementia and cognitive impairment” ” Holfordwatch takes a cool look at more claims by Ann Walker.
“Red Clover comments leave a bitter aftertaste” Click here
“The War Against Gobbledygook” Comment from Astrophysicists.
“UCL Makes good” Comment from the University of Minnesota
University Diaries. A US Professor of English reproduced Ben Goldacre’s first
article.
“Science bloggers unite” Comment from a Yale neurologist.
“The Guardian: a quackbuster . . . “ Comment from MIT (and it’s on the MIT server).
“UCL change tack: Colquhoun is back” The Sceptical Preacher speaks
Freedom of speech and litigious herbalists
Announcement 13 June 2007. UCL restores
DC’s IMPROBABLE SCIENCE page.
After taking legal advice, the provost and I have agreed a joint statememt.
Read it on the UCL web site.
“ . . . the Provost and Professor Colquhoun have taken advice from
a senior defamation Queen’s Counsel, and we are pleased to announce that Professor Colquhoun’s website – with some modifications effected by him on counsel’s advice – will shortly be restored to UCL’s servers.”
I am grateful to UCL for its legal support, and I’m very grateful too for the enormous support I’ve had from many people, especially since Ben Goldacre mentioned the site move. Now all I need is a bit of help to get it into a more convenient format. The page will stay at its present address until there is time to sort things out. For some of the fallout from these events, click here. The name of the page has been changed from quack.html to improbable.html on the advice of lawyers, but the old addresses still work.
Announcement 30 May 2007.
My item about claims made for alleged benefits of the red clover and other herbs has resulted in complaints being made to the provost of UCL (Malcolm Grant), and to Chair of Council (Lord Woolf). The complaints have come from Alan Lakin, husband of Ann Walker. I have received no complaints from them myself.
In the six or years that I have been running this attempt to improve public understanding of science, I am aware of only two serious complaints being made, and as far as I know, this is the first to reach the level of the provost. This one resulted in a request to remove of this page from the UCL server, but that is now reversed.
This is a slightly modified version of some thoughts from the old improbable science page, where they formed part of the review of a BBC2 series on alternative medicine. It has been moved to the new blog because of the comments posted here.
Evolution of plants
Plants didn’t evolve for our benefit. Natural selection ensures that plants, like every other living thing, evolve in a way that maximises their own chance of survival. To ensure that, plants should be as toxic as possible to anything that might eat them. The more harm a plant does to humans, the better its chance of survival. It is sheer luck that some of the toxic principles evolved by plants occasionally turn out to be useful.
| Memo to: The members of the Kansas Board of Education From: God Re: Your decision to eliminate the teaching of evolution as science Thank you for your support. Much obliged. Now, go forth and multiply. Beget many children. And yea, your children shall beget children. And their children shall beget children, and their children’s children after them. And in time the genes that made you such pinheads will be eliminated through natural selection. Because that is how it works.’ . . . ; By Gene Weingarten, Washington Post Staff Writer. Saturday, August 14, 1999; Page C01 |
Naturalness
Here are some products of nature. That doesn’t mean they are good for you.
Lead, uranium, radon, arsenic, thallium, strychnine, cyanide (in Sorghum and Prunus species), Stinging nettles, poison ivy, yew, deadly nightshade, castor beans (ricin), tobacco, curare, foxglove, fly agaric, (muscarine), death cap (amanita phalloides), . . ..
Foxgloves, heart failure and biological standardisation
Here is a bit of relevant pharmacological history.
The 24th edition of Martindale’s Extra Pharmacopoeia (1958) describes Digitalis Leaf (B.P., I.P.), also known as Digit. Fol.; Digitalis; Foxglove Leaf; Feuille de Digitale; Fingerhutblatt; Hoja de digital.
| It was defined as “the dried leaves of Digitalis purpurea (Scrophulariaceae).”At that time it was sometimes prescribed as Prepared Digitalis (BP), which is “Digitalis leaf reduced to powder, no part being rejected, and biologically assayed the strength being stated in units per g. For therapeutic purposes it must be adjusted to contain 10 units in 1 g.”Sometimes foxglove leaf was prescribed as Tincture of Digitalis (B.P., I.P.). “It may be made from unstandardised leaf, the tincture being subsequently biologically assayed, or it may be made from prepared digitalis, using a quantity containing 1000 units per litre, by percolation or maceration, with alcohol (70 %). It contains 1 unit per ml. I.P. allows also 1 unit per g. Dose: 0.3 to 1 ml. (5 to 15 minims). ” |
 |
Although these preparations are now totally defunct, they were still better than the sort of thing that is now advocated by herbalists. Why? They were better because they were standardised.
Foxglove leaves contain several chemical compunds that are useful in certain forms of hear failure. But the margin of safety is quite low. Take a bit too much and it kills you not cures you. One batch of foxglove leaves will contain different amounts of active compounds from the last batch, and that endangered patients.
From the 1930s onwards, pharmacologists developed methods of biological assay that overcame this problem. An international
standard digitalis leaf sample was established. Every new batch had to be assayed against this standard, and diluted to a fixed level of biological activity. This ensured that each batch of digitalis powder had the same biological potency as the last batch. It was a great pharmacological advance in its time. But of course it did involve the use of animals for the biological assay.
All this was solved when the active principles were purified from the foxglove leaves. There was no longer any need to uses animals for biological assays. The right amount of pure digoxin or digitoxin could be weighed out.
Fortunately herbalists are not allowed to prescribe anything as potentially dangerous as digitalis. But in general herbalists are happy to use pre-1930, unstandardised plant extracts.
I can think of no case in which there is the slightest reason to think that the mixture of chemicals in the plant is any better than the purified active principles. Of course there could be such cases of synergy. But that is just idle speculation.
No surprise there then, because idle speculation is the stuff of alternative medicine. It’s a great deal easier than making the effort to find out what works, and probably more lucrative too.
On 21 November, 2005, Dr David Spence appeared on the BBC’s Today Programme. He was being interviewed about a report that, he said, provided evidence for the effectiveness of homeopathy. In fact it does nothing of the sort.
Dr Spence’s paper was published in the Journal of Alternative and Complementary Medicine. It is not really research at all. They simply asked 6544 patients who had had homeopathic treatment whether they felt better or not. Half the patients (50.7%) said they were ‘better’ ot ‘much better’. A further 20% said they were ‘slightly better’. The patients who had homeopathic treatment were not compared with anything whatsoever!
This is reported in a straighforward way. What is quite ludicrous is the stated conclusion of the paper:
“The study results show that homeopathic treatment is a valuable intervention”.
It is obvious that there is not the slightest reason to attribute the answers given by patients to the fact that they had been given homeopathic treatment. That would be the crudest form of post hoc ergo propter hoc error. It does not even show that the homeopathic treatment was producing a placebo effect.
Papers like this do not add to human knowledge, they detract from it. By reverting to pre-enlightment forms of argument, they mislead rather than enlighten. To make matters worse, this work was done at public expense, by the Directorate of Homeopathic Medicine, United Bristol Healthcare, National Health Service Trust, Bristol, United Kingdom.
What on earth is a respectable hospital and medical school, like those in Bristol, wasting money with this sort of mediaeval hindrance to medical knowledge? We are truly living in an age of delusions.
Download the paper and see for yourself [ Spence DS, Thompson EA, Barron SJ. J Altern Complement Med. 2005, 11, 793-8. pdf file, 74 kb].
The Daily Telegraph recently published two reports about acupuncture. One said it worked. The other said it didn’t work. Needle cure effect ‘is not all in the mind’ By Catriona Davies, starts
Acupuncture has a genuine ability to relieve pain, scientists have found.
The other report was
Doubt cast on needle therapy for migraine By Nic Fleming, Health Correspondent, starts
Acupuncture is no better at reducing migraines than fake treatment, researchers say today.
A study involving more than 300 patients found the healing method did reduce headaches, but only by the same amount as placing needles at non-acupuncture points.
Unfortunately the Daily Telegraph‘s reporters did nothing to help the confused reader. No comment was made on the apparent contradiction. In this particular case, there is an obvious explanation.
The first (favourable) article was said to be published in Nature, though in fact it was published in Neuroimage (Pariente J., White P., Frackowiak , Richard S. J. & Lewith G. Neuroimage, 25. 1161 – 1167, 2005). Presumably the reporter had picked it up from a rather uncritical synopsis on the news site, nature.com. It was conducted on 14 patients with painful osteoarthritis. Contrary to the first line of the Telegraph‘s report (“Acupuncture has a genuine ability to relieve pain”), the work did not measure pain at all. In fact the summary of the paper says
“The three interventions, all of which were sub-optimal acupuncture treatment, did not modify the patient’s pain.”
What the paper actually did was to use positron emission tomography (PET) to measure ‘activation’ of certain parts of the brain when needles were inserted. Some parts were activated more by having acupuncture needles piercing ths body than by ‘stage-dagger’ needles which retracted and did not pierce the body. I have no criticism of these findings: my purpose here is to explore the apparent contradiction between this trial and another.
The second, unfavourable, report was of a much bigger study, 302 patients with migraine headaches. It was published by Linde et al. (Journal of the American Medical Association. 2005 293(17):2118-25). This study concluded
“Acupuncture was no more effective than sham acupuncture in reducing migraine headaches although both interventions were more effective than a waiting list control. ”
These two studies were on quite different conditions, used different methods, and very different numbers of patients. But suppose we take them at face value, are they not contradictory? No, not necessarily, because they used quite different sorts of control group.
The study that was reported as showing that acupuncture worked compared patients that had real acupuncture with patients who had treatment with “stage dagger” needles that appeared to pierce the skin but did not.
The study that was reported as showing that acupuncture did not work (Linde et al.) used a different sort of control group, acupuncture needles that pierced the skin but were inserted in the wrong places (as defined by the ‘principles’ of acupuncturists). No difference was found between ‘real acupuncture’ and control.
There is nothing incompatible about these two studies if one adopts the view that piercing the skin with a needle can produce a physiological response that makes the patient feel that other sorts of pain are less painful, but that it does not matter where the skin is pierced. The latter hypothesis means, of course, that all talk about “meridians”` and “energy flow” that acupuncturists use, is no more than mumbo jumbo.
Dr Lewith is quoted as saying, of the negative study, “This is a badly conceived study that just adds more confusion to the debate because it uses non-site specific acupuncture as a control.” Quite on the contrary, the Linde study seems more interesting to me, because it unveils the mumbo jumbo of meridians (at least for the particular points used in this study). Dr Lewith may find this conclusion unpalatable, but it is the obvious implication of this pair of studies.
Another study confirms that the principles of acupuncture are nonsense
A trial by Melchart and colleagues on 270 patients shows conclusively that acupuncture can indeed produce amelioration of tension-type headache when compared with no treatment, BUT the relief is produced whether or not needles are inserted at ‘acupuncture points’. Very similar results were found with ‘superficial needling at non-acupuncture points’. British Medical Journal, 15 August 2005. Yet again it is shown that the mumbo-jumbo of meridians and magic points is nonsense. Yet again, that is a good reason why universities cannot be expected to train acupuncturists. Our business is to minimise mumbo-jumbo, not to propagate it.