
Download Lectures on Biostatistics (1971). Corrected and searchable version of Google books edition
Download review of Lectures on Biostatistics (THES, 1973).
subluxation
Almost all the revelations about what’s taught on university courses in alternative medicine have come from post-1992 universities. (For readers not in the UK, post-1992 universities are the many new univerities created in 1992, from former polytechnics etc, and Russell group universities are the "top 20" research-intensive universities)
It is true that all the undergraduate courses are in post-1992 universities, but the advance of quackademia is by no means limited to them. The teaching at St Bartholomew’s Hospital Medical School, one of the oldest, was pretty disgraceful for example, though after protests from their own students, and from me, it is now better, I believe.

Quackery creeps into all universities to varying extents. The good ones (like Southampton) don’t run "BSc" degrees, but it still infiltrates through two main sources,
The first is via their HR departments, which are run by people who tend to be (I quote) "credulous and moronic" when it comes to science.
The other main source is in teaching to medical students. The General Medical Council says that medical students must know something about alterantive medicine and that’s quite right, A lot of their patients will use it. The problem is that the guidance is shockingly vague .
“They must be aware that many patients are interested in and choose to use a range of alternative and complementary therapies. Graduates must be aware of the existence and range of such therapies, why some patients use them, and how these might affect other types of treatment that patients are receiving.” (from Tomorrow’s Doctors, GMC)
In many medical schools, the information that medical students get is quite accurate. At UCL and at King’s (London) I have done some of the familiarisation myself. In other good medical schools, the students get some shocking stuff. St Bartholomew’s Hospital medical School was one example. Edinburgh University was another.
But there is one Russell group university where alternative myths are propagated more than any other that I know about. That is the University of Southampton.
In general, Southampton is a good place, I worked there for three years myself (1972 – 1975). The very first noise spectra I measured were calculated on a PDP computer in their excellent Institute of Sound and Vibration Research, before I wrote my own programs to do it.
But Southanpton also has a The Complementary and Integrated Medicine Research Unit . Oddly the unit’s web site, http://www.cam-research-group.co.uk, is not a university address, and a search of the university’s web site for “Complementary and Integrated Medicine Research Unit” produces no result. Nevertheless the unit is “within the School of Medicine at the University of Southampton”
Notice the usual euphemisms ‘complementary’ and ‘integrated’ in the title: the word ‘alternative’ is never used. This sort of word play is part of the bait and switch approach of alternative medicine.
The unit is quite big: ten research staff, four PhD students and two support staff It is headed by George Lewith.
Teaching about alternative medicine to Southampton medical students.
The whole medical class seems to get quite a lot compared with other places I know about. That’s 250 students (210 on the 5-year course plus another 40 from the 4-year graduate-entry route).
Year 1: Lecture by David Owen on ‘holism’ within the Foundation Course given to all 210 medical students doing the standard (5-year) course.
Year 2: Lecture by Lewith (on complementary medicine, focusing on acupuncture for pain) given within the nervous systems course to the whole medical student year-group (210 students).
Year 3 SBOM (scientific basis of medicine) symposium: The 3-hour session (“Complementary or Alternative Medicine: You Decide”). I’m told that attendance at this symposium is often pretty low, but many do turn up and all of them are officially ‘expected’ to attend.
There is also an optional CAM special study module chosen by 20 students in year 3, but also a small number of medical students (perhaps 2 – 3 each year?) choose to do a BMedSci research project supervised by the CAM research group and involving 16-18 weeks of study from October to May in Year 4. The CAM research group also supervise postgraduate students doing PhD research.
As always, a list of lectures doesn’t tell you much. What we need to know is what’s taught to the students and something about the people who teach it. The other interesting question is how it comes about that alternative medicine has been allowed to become so prominent in a Russell group university. It must have support from on high. In this case it isn’t hard to find out where it comes from. Here are some details.
Year 1 Dr David Owen
David Owen is not part of Lewith’s group, but a member of the Division of Medical Education headed by Dr Faith Hill (of whom, more below). He’s one of the many part-time academics in this area, being also a founder of The Natural Practice .
Owen is an advocate of homeopathy (a past president of the Faculty of Homeopathy). Homeopathy is, of course, the most barmy and discredited of all the popular sorts of alternative medicine. Among those who have discredited it is the head of the alt med unit, George Lewith himself (though oddly he still prescribes it).
And he’s also a member of the British Society of Environmental Medicine (BSEM). That sounds like a very respectable title, but don’t be deceived. It is an organisation that promotes all sorts of seriously fringe ideas. All you have to do is notice that the star speaker at their 2011 conference was none other than used-to-be a doctor, Andrew Wakefield, a man who has been responsible for the death of children from measles by causing an unfounded scare about vaccination on the basis of data that turned out to have been falsified. There is still a letter of support for Wakefield on the BSEM web site.
The BSEM specialises in exaggerated claims about ‘environmental toxins’ and uses phony allergy tests like kinesiology and the Vega test that misdiagnose allergies, but provide en excuse to prescribe expensive but unproven nutritional supplements, or expensive psychobabble like "neuro-linguistic programming".
Other registered "ecological physicians" include the infamous Dr Sarah Myhill, who, in 2010, was the subject of a damning verdict by the GMC, and Southampton’s George Lewith.
If it is wrong to expose medical students to someone who believes that dose-response curves have a negative slope (the smaller the dose the bigger the effect -I know, it’s crazy), then it is downright wicked to expose students to a supporter of Andrew Wakefield.
David Owen’s appearance on Radio Oxford, with the indomitable Andy Lewis appears on his Quackometer blog.
Year 2 Dr George Lewith
Lewith is a mystery wrapped in an enigma. He’s participated in some research that is quite good by the (generally pathetic) standards of the world of alternative medicine.
In 2001 he showed that the Vega test did not work as a method of allergy diagnosis. "Conclusion Electrodermal testing cannot be used to diagnose environmental allergies", published in the BMJ .[download reprint].
In 2003 he published "A randomized, double-blind, placebo-controlled proving trial of Belladonna 30C” [download reprint] that showed homeopathic pills with no active ingredients had no effects: The conclusion was "”Ultramolecular homeopathy has no observable clinical effects" (the word ultramolecular, in this context, means that the belladonna pills contained no belladonna).
In 2010 he again concluded that homeopathic pills were no more than placebos, as described in Despite the spin, Lewith’s paper surely signals the end of homeopathy (again). [download reprint]
What i cannot understand is that, despite his own findings, his private practice continues to prescribe the Vega machine and continues to prescribe homeopathic pills. And he continues to preach this subject to unfortunate medical students.
Lewith is also one of the practitioners recommended by BSEM. He’s a director of the "College of Medicine". And he’s also an advisor to a charity called Yes To Life. (see A thoroughly dangerous charity: YesToLife promotes nonsense cancer treatments).
3rd year Student Selected Unit
The teaching team includes:
- David Owen – Principal Clinical Teaching Fellow SoM, Holistic Physician
- George Lewith – Professor of Health Research and Consultant Physician
- Caroline Eyles – Homeopathic Physician
- Susan Woodhead – Acupuncturist
- Elaine Cooke – Chiropractic Practitioner
- Phine Dahle – Psychotherapist
- Keith Carr – Reiki Master
- Christine Rose – Homeopath and GP
- David Nicolson – Nutritionalist
- Shelley Baker – Aromatherapist
- Cheryl Dunford – Hypnotherapist
- Dedj Leibbrandt – Herbalist
More details of the teaching team here. There is not a single sceptic among them, so the students don’t get a debate, just propaganda.
In this case. there’s no need for the Freedom of Information Act. The handouts. and the powerpoints are on their web site. They seem to be proud of them
Let’s look at some examples
Chiropractic makes an interesting case, because, in the wake of the Singh-BCA libel case, the claims of chiropractors have been scrutinised as never before and most of their claims have turned out to be bogus. There is a close relationship between Lewith’s unit and the Anglo-European Chiropractic College (the 3rd year module includes a visit there). In fact the handout provided for students, Evidence for Chiropractic Care , was written by the College. It’s interesting because it provides no real evidence whatsoever for the effectiveness of chiropractic care. It’s fairly honest in stating that the view at present is that, for low back pain, it isn’t possible to detect any difference between the usefulness of manipulation by a physiotherapist, by an osteopath or by a chiropractor. Of course it does not draw the obvious conclusion that this makes chiropractic and osteopathy entirely redundant -you can get the same result without all the absurd mumbo jumbo that chiropractors and osteopaths love, or their high-pressure salesmanship and superfluous X-rays. Neither does it mention the sad, but entirely possible, outcome that none of the manipulations are effective for low back pain. There is, for example, no mention of the fascinating paper by Artus et al [download reprint]. This paper concludes
"symptoms seem to improve in a similar pattern in clinical trials following a wide
variety of active as well as inactive treatments."
This paper was brought to my attention through the blog run by the exellent physiotherapist, Neil O’Connell. He comments
“If this finding is supported by future studies it might suggest that we can’t even claim victory through the non-specific effects of our interventions such as care, attention and placebo. People enrolled in trials for back pain may improve whatever you do. This is probably explained by the fact that patients enrol in a trial when their pain is at its worst which raises the murky spectre of regression to the mean and the beautiful phenomenon of natural recovery.”
This sort of critical thinking is conspicuously absent from this (and all the other) Southampton handouts. The handout is a superb example of bait and switch: No nonsense about infant colic, innate energy or imaginary subluxations appears in it.
Acupuncture is another interesting case because there is quite a lot of research evidence, in stark contrast to the rest of traditional Chinese medicine, for which there is very little research.
|
There is a powerpoint show by Susan Woodhead (though it is labelled British Acupuncture Council). The message is simple and totally uncritical. It works. |

|
In fact there is now a broad consensus about acupuncture.
(1) Real acupuncture and sham acupuncture have been found to be indistinguishable in many trials. This is the case regardless of whether the sham is a retractable needle (or even a toothpick) in the "right" places, or whether it is real needles inserted in the "wrong" places. The latter finding shows clearly that all that stuff about meridians and flow of Qi is sheer hocus pocus. It dates from a pre-scientific age and it was wrong.
(2) A non-blind comparison of acupuncture versus no acupuncture shows an advantage for acupuncture. But the advantage is usually too small to be of any clinical significance. In all probability it is a placebo effect -it’s hard to imagine a more theatrical event than having someone in a white coat stick long needles into you, like a voodoo doll. Sadly, the placebo effect isn’t big enough to be of much use.
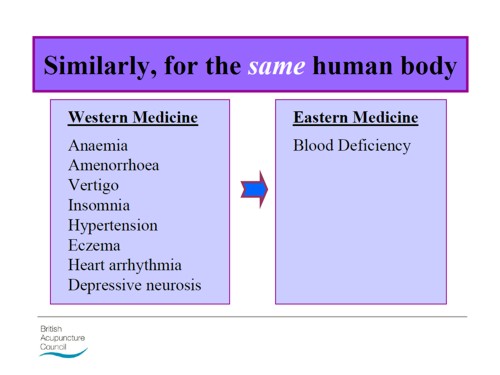
Needless to say, none of this is conveyed to the medical students of Southampton. Instead they are shown crude ancient ideas that date from long before anything was known about physiology as though they were actually true. These folks truly live in some alternative universe. Here are some samples from the acupuncture powerpoint show by Susan Woodhead.
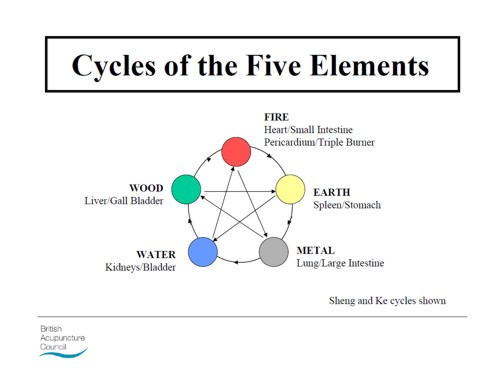
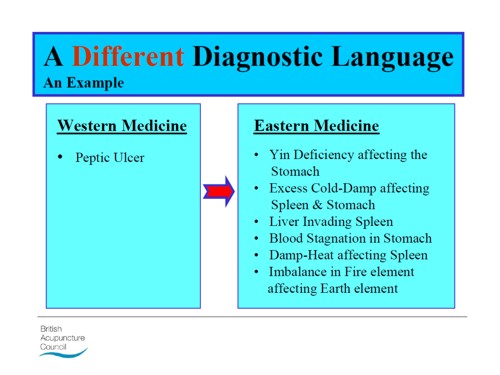
Well this is certainly a "different diagnostic language", but no attempt is made to say which one is right. In the mind of the acupuncurist it seems both are true. It is a characteristic of alternative medicine advocates that they have no difficulty in believing simultaneously several mutually contradictory propositions.
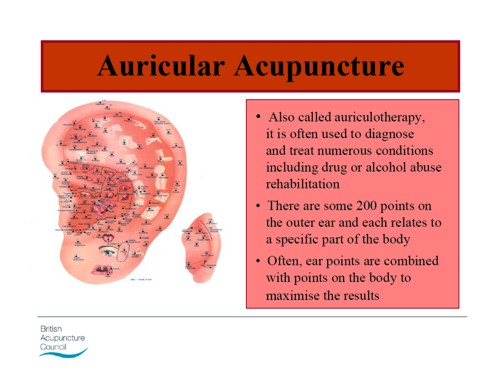
As a final exmple of barminess, just look at the acupuncture points (allegedly) on the ear The fact that it is a favoured by some people in the Pentagon as battlefield acupuncture, is more reminiscent of the mad general, Jack D. Ripper, in Dr Strangelove than it is of science.
There is an equally uncritical handout on acupuncture by Val Hopwood. It’s dated March 2003, a time before some of the most valuable experiments were done.
The handout says "sham acupuncture
is generally less effective than true acupuncture", precisely the opposite of what’s known now. And there are some bits that give you a good laugh, always helpful in teaching. I like
“There is little doubt that an intact functioning nervous system is required for acupuncture to produce
analgesia or, for that matter, any physiological changes”
and
Modern techniques: These include hybrid techniques such as electro-acupuncture . . . and Ryadoraku [sic] therapy and Vega testing.
Vega testing!! That’s been disproved dozens of times (not least by George Lewith). And actually the other made-up nonsense is spelled Ryodoraku.
It’s true that there is a short paragraph at the end of the handout headed "Scientific evaluation of acupuncture" but it doesn’t cite a single reference and reads more like excuses for why acupuncture so often fails when it’s tested properly.
Homeopathy. Finally a bit about that most boring of topics, the laughable medicine that contains no medicine, homeopathy. Caroline Eyles is a member for the Society of Homeopaths, the organisation that did nothing when its members were caught out in the murderous practice of recommending homeopathy for prevention of malaria. The Society of Homeopaths also endorses Jeremy Sherr, a man so crazy that he believes he can cure AIDS and malaria with sugar pills.
The homeopathy handout given to the students has 367 references, but somehow manages to omit the references to their own boss’s work showing that the pills are placebos. The handout has all the sciencey-sounding words, abused by people who don’t understand them.
"The remedy will be particularly effective if matched to the specific/particular characteristics of the individual (the ‘totality’ of the patient) on all levels, including the emotional and mental levels, as well as just the physical symptoms. ‘Resonance’ with the remedy’s curative power will then be at it’s [sic] best."
The handout is totally misleading about the current state of research. It says
"increasing clinical research confirms it’s [sic] clinical effectiveness in treating patients, including babies and animals (where a placebo effect would be hard to justify)."
|
The powerpont show by Caroline Eyles shows all the insight of a mediaeval vitalist |
|
Anyone who has to rely on the utterly discredited Jacques Benveniste as evidence is clearly clutching at straws. What’s more interesting about this slide the admission that "reproducibility is a problem -oops, an issue" and that RCTs (done largely by homeopaths of course) have "various methodological flaws and poor external validity". You’d think that if that was the best that could be produced after 200 yours, they’d shut up shop and get another job. But, like aging vicars who long since stopped believing in god, but are damned if they’ll give up the nice country rectory, they struggle on, sounding increasingly desperate.
How have topics like this become so embedded in a medical course at a Russell group university?
The details above are a bit tedious and repetitive. It’s already established that hardly any alternative medicine works. Don’t take my word for it. Check the web site of the US National Center for Complementary and Alternative Medicine (NCCAM) who, at a cost of over $2 billion have produced nothing useful.
A rather more interesting question is how a good university like Southampton comes to be exposing its medical students to teaching like this. There must be some powerful allies higher up in the university. In this case it’s pretty obvious who thay are.
Professor Stephen Holgate MD DSc CSc FRCP FRCPath FIBiol FBMS FMed Sci CBE has to be the primary suspect, He’s listed as one of Southampton’s Outstanding Academics. His work is nothing to do with alternative medicine but he’s been a long term supporter of the late unlamented Prince of Wales’ Foundation, and he’s now on the advisory board of it’s successor, the so called "College of Medicine" (for more information about that place see the new “College of Medicine” arising from the ashes of the Prince’s Foundation for Integrated Health, and also Don’t be deceived. The new “College of Medicine” is a fraud and delusion ). His description on that site reads thus.
"Stephen Holgate is MRC Clinical Professor of Immunopharmacology at the University of Southampton School of Medicine and Honorary Consultant Physician at Southampton University Hospital Trust. He is also chair of the MRC’s Populations and Systems Medicine Board. Specialising in respiratory medicine, he is the author of over 800 peer-reviewed papers and contributions to scientific journals and editor of major textbooks on asthma and rhinitis. He is Co-Editor of Clinical and Experimental Allergy, Associate Editor of Clinical Science and on the editorial board of 25 other scientific journals."
Clearly a busy man. Personally I’m deeply suspicious of anyone who claims to be the author of over 800 papers. He graduated in medicine in 1971, so that is an average of over 20 papers a year since then, one every two or three weeks. I’d have trouble reading that many, never mind writing them.
Holgate’s long-standing interest in alternative medicine is baffling. He’s published on the topic with George Lewith, who, incidentally, is one of the directors of the "College of Medicine"..
It may be unkind to mention that, for many years now, I’ve been hearing rumours that Holgate is suffering from an unusually bad case of Knight starvation.
The Division of Medical Education appears to be the other big source of support for. anti-scientific medicine. That is very odd, I know, but it was also the medical education people who were responsible for mis-educating medical students at. St. Bartholomew’s and at Edinburgh university. Southampton’s Division of Medical Education has a mind-boggling 60 academic and support staff. Two of them are of particular interest here.
Faith Hill is director of the division. Her profile doesn’t say anything about alternative medicine, but her interest is clear from a 2003 paper, Complementary and alternative medicine: the next generation of health promotion?. The research consisted of reporting anecdotes from interviews of 52 unnamed people (this sort of thing seems to pass for research in the social sciences). It starts badly by misrepresenting the conclusions of the House of Lords report (2000) on CAM. Although it comes to no useful conclusions, it certainly shows a high tolerance of nonsensical treatments.
Chris Stephens is Associate Dean of Medical Education & Student Experience. His sympathy is shown by a paper he wrote In 2001, with David Owen (the homeopath, above) and George Lewith: Can doctors respond to patients’ increasing interest in complementary and alternative medicine?. Two of the conclusions of this paper were as follows.
"Doctors are training in complementary and alternative medicine and report benefits both for their patients and themselves"
Well, no actually. It wasn’t true then, and it’s probably even less true now. There’s now a lot more evidence and most of it shows alternative medicine doesn’t work.
"Doctors need to address training in and practice of complementary and alternative medicine within their own organisations"
Yes they certainly need to do that.
And the first thing that Drs Hill and Stephens should do is look a bit more closely about what’s taught in their own university, I hope that this post helps them,
Follow-up
4 July 2011. A correspondent has just pointed out that Chris Stephens is a member of the General Chiropractic Council. The GCC is a truly pathetic pseudo-regulator. In the wake of the Simon Singh affair it has been kept busy fending off well-justified complaints against untrue claims made by chiropractors. The GCC is a sad joke, but it’s even sadder to see a Dean of Medical Education at the University of Southampton being involved with an organisation that has treated little matters of truth with such disdain.
A rather unkind tweet from (ex)-chiropractor @RichardLanigan.
“Chris is just another light weight academic who likes being on committees. Regulatory bodies are full of them”


Snow on December 18th Roaring fire
Lindy contributes acute comments regularly here. She is also an accomplished musician. She has kindly allowed me to post here four of her re-written carols.
Adam lay ybounden | Hark the Herald | Holly and the Ivy | Merry Gentlemen
Adam lay ybounden
The Middle English dialect is not easy to follow. In fact Wikipedia reveals that it is oit even standard Middle English, but Macaronic English. The original words are reproduced in the right hand column. The original, sung by choir of King’s College Chapel, is on YouTube.
| Atoms lay y’bounden In primordial soup; Six billion years did pass A’fore they could regroup. For first had bin a big bang The universe was shook; Though through milennia For god it was mistook. Then particles of light did shine, ema- -nating from the sun. Out of soup arose archaea And so life was begun. Thanks be to the man This mystery did solve; Through him we celebrate how we Did from the bugs evolve. |
Adam lay ybounden, Bounden in a bond: Four thousand winter Thought he not too long. And all was for an apple, An appil that he took, As clerkè finden Written in their book. Ne had the apple taken been, The appil taken been, Ne had never our lady Abeen heavenè queen. Blessèd be the time That appil taken was, Therefore we moun singen, Deo gracias! . |
Hark the Herald Angels sing.
This version is for Simon Singh. If you haven’t yet signed the new peition, please do it here.
Mark this very dang’rous thing,
Story is of Simon Singh.
He got chiropractors riled,
“Sod it! We have been defiled!
Ployful all ye woosters rise,
Join us to defend our lies,
With us loudly please proclaim,
Subluxations are our game”
Christ, they all with one accord
Took young Simon off to court.
“We’ll put you before a judge,
Since we always bear a grudge
‘Gainst all those who say our modus
Operandi is all bogus;
Mark the words of justice Eady,
Gave his ruling oh so speedy.
Mark the case of Simon Singh
With support the web does ring.
Ditch draconian libel laws,
Without which they’d have no cause
To sue those who would speak freely,
Truth, opinion-and reason really
Should prevail o’er all such things,
Surely he his case must win.
The Holly and the Ivy
Dedicated to the Prince of Wales, certain vice-chancellors and other champions of the endarkenment.
The folly and the lies, see
How they’ve become full-blown;
The braying of th’quackti’tioner Roy-
Al, th’enlightenment has flown.
Refrain: For deriding all the data
(Such stunning stuff we hear)!
The displaying of such cherry pick-
-Ing, beats bringing in Chi square.
The folly hears no critics
It makes you quite struck dumb,
Just put a poison substance in,
And dilute to kingdom come.
For deriding all the data etc.
The folly so does blossom,
Beguiles you with its charm,
Just make some movements with your wrist
And it will do no harm.
For deriding all the data etc.
The folly’s given credence
If you are qualified
With a BSc in pseudosci-
-Ence, th’endarkenment is nigh!
For deriding all the data etc.
The folly bears a burden
Now it has fallen down;
F.O.I requests and publicity
Have giv’n D.C. the crown.
For deriding all the data etc.
The folly is so fickle,
How did they have the gall
To tell us how their remedies
Were here to treat us all?
For deriding all the data etc.
The folly and the lies, see
How they must surely fail
We’ll drink a toast to good evidence
And let real science prevail!
Alternative refrain:
Oh the rising of the Reiki,
Of acupuncture too,
All Rolfering* and Tuina-ish,
They all amount to woo.
*The names Rolf and Roger seem remarkably similar in some circumstances so I get a little confused.
Merry gentlemen.
Here is Lindy’s version of "god rest ye merry gentleman", composed in the wake of the admission by the Professional Standards director of Boots the Chemists that they sell homeopathic pills despite being aware of the fact that there is no reason to think they work.
I arrest you merry gentlemen,
Please kindly step this way.
For you are selling sugar pills
For which the people pay;
We’re from the Trading Standards and through courts we’ll find a way
To stop your profit-making ploy, Profiting ploy,
We’ll stop your profiteering ploy”!
The chemists calmly did defend
Themselves though they were riled;
“The people do demand these pills
Because they’re not defiled
With molecules (nor ‘owt at all), despite the claims so wild;
We’ll continue our profiteering ploy, Profiting ploy,
We’ll continue our profiteering ploy”.
So Trading Standards did respond
“We understand your aim
To make more money, though if you
Persist with bogus claim
To cure disease with sugar pills,
We’ll put you all to shame!
We are stopping your profiteering ploy, Profiting ploy,
We are stopping your profiteering ploy”.
“You breach the regulations by selling pills, you see,
Which claim to contain ‘aqua’ (dilute to 30C),
Or ‘dolphin song’ or ‘canine testes’ – even ‘ATP’!
So you’ll stop all this profiteering ploy, profiting ploy,
So you’ll stop all this profiteering ploy”.
The Dept of Health bangs on and on
About a patient’s choice,
But all good people must condemn
These lies with one great voice.
We dream of days when fibs are gone and we can all rejoice
‘Cos they’ve stopped all their profiteering ploy, Profiting ploy,
‘Cos they’ve stopped all their profiteering ploy
Chiropractors are getting very touchy indeed, all over the world. And no wonder, because their claims are being exposed as baseless as never before, in the wake of their attempts to stifle criticism by legal action..
In March, Shaun Holt appeared on Breakfast TV in New Zealand. Holt has done a lot of good work on TV in debunking some of the preposterous claims made by quacks. See him on YouTube.
This time he talked about chiropractic. Here is the video.
One could argue that he was over generous to chiropractic, especially when talking about their effectiveness in treating low back pain. He said, quite rightly, that chiropractors are no better than physiotherapists at treating low back pain.
But a recent trial suggests that neither are much good. “A randomised controlled trial of spinal manipulative therapy in acute low back pain” (Juni et al., 2009 in the BMJ; see also coverage in Pulse). This trial compared standard care with standard care plus spinal manipulative therapy (SMT). The results were negative, despite the fact that this sort of A + B vs B design is inherently biassed in favour of the treatment (see A trial design that generates only ”positive” results, Ernst & Lee 2008, Postgrad Med J.).
"SMT was performed by a specialist in manual medicine, chiropractice and rheumatology (GH), a specialist in physical medicine (DV) or an osteopath (RvB), all proficient in SMT."
"Conclusions: SMT is unlikely to result in relevant early pain reduction in patients with acute low back pain."
Admittedly, the trial was quite small (104 patients, 52 in each group) so it will need to be confirmed. but the result is entirely in line with what we knew already.
It also adds to the evidence that the recommendation by NICE of SMT by chiropractors constitutes their biggest failure ever to assess evidence properly. If NICE don’t amend this advice soon, they are in danger of damaging their hitherto excellent record.
Despite the moderate tone and accuracy of what Holt said on TV, the New Zealand Chiropractors’ Association made a formal complaint. That is what they like to do, as I learned recently, to my cost. It is so much easier than producing evidence.
Quite absurdly the New Zealand Broadcasting Standards Authority (BSA) has upheld some of the complaints. Their judgement can be read here.
The BSA consists of four people, two lawyers and two journalists. So not a trace of scientific expertise among them. Having people like that judging the claims of chiropractors makes as much sense as having them judged by Mr Justice Eady. They seem to be the sort of people who think that if there is a disagreement, the truth must lie half-way between the opposing views.
One of the BSA members, Tapu Misa, has used her newspaper column to quote approvingly the views of the notorious Dr Mercola web site on flu prevention “Your best defence, it says, is to eat right, get lots of sleep, avoid sugar and stress, load up on garlic, Vitamin D and krill oil”. (Snake oil is said to be good too.) There are some odd attitudes to science in some of her other columns too (e.g. here and here). Not quite the person to be judging the evidence for and against chiropractic, I think.
In fact the TV show in question was more than fair to chiropractors. It adopted the media’s usual interpretation of fair and balanced: equal time for the flat earthers. A Chiropractor was invited to reply to Holt’s piece. Here he is.
The chiropractor, Doug Blackbourn, started very plausibly, though a tendency to omit every third syllable made transcription hard work. He established that if you cut yourself you get better (without any help). He established that nerves run down the spinal cord. So far, so good. But then he quickly moved on to the usual flights of fancy.
"We have two premises. The body heals itself and the nervous system runs the body. Now the nervous system runs the body, travels down through the spinal cord so chiropractic is not based on the belief that, you know, energy flows, it’s based on the fact that your nervous system runs the body and [inaudible] affects the overall health of the body"
This statement is totally vague. It has nothing whatsoever to do with the main question, can chiropractors do anything useful. It is sheer flannel.
We’re seeing people, heck, diabetes. I had a quadriplegic come in one time for adjustment, we’ve got stroke people, we’ve got all sorts of conditions. We’re not treating the condition, We’re allowing, checking the spine to see if there’s any interference there that will slow the body down"
“Interference”? “slowing the body down”? These are utterly meaningless phrases that simply serve to distract from the only question that matters.
"Chiropractice is the most safest [sic] profession to go to to get your spine adjusted"
Hmm I thought it was the only job that uses the word ‘adjustment’.
Worst of all was his response to a question about asthma.
Presenter: "So chiropractors are not out there claiming they will cure asthma for example?". Chiropractor: "No"
This is simply untrue, both in New Zealand and in the UK. For a start, just look at what Blackbourn’s own web site says about asthma.
"The challenge, of course, with allergy and asthma medication is there is no end-point. There is no cure. Asthma and allergies, for the most part, are lifelong conditions requiring lifelong medication. Might there be a better way, an alternative solution?
“Alternative” is the key word. Medical treatment is designed to combat symptoms, and is successful to a certain extent with allergies and asthma. Underlying causes are not addressed, however, and symptoms continue year after year. What else might be done?
Enter chiropractic care. Chiropractic health care, with its unique comprehensive approach, is able to offer positive benefit to a variety of conditions and ailments. In the case of allergies and asthma, these “hypersensitivity conditions” may respond well to therapy designed to normalize the body’s flow of nerve signals. To use a metaphor, chiropractic treatment removes roadblocks to the body’s natural healing abilities. Restoring these imbalances may help reduce such hypersensitivity reactions."
Blackbourn’s web site describes him thus
"As a Doctor of Chiropractic, Dr. Doug Blackbourn . . ."
But the qualifications of “Dr” Blackbourn are B.App.Sc (Chiro) M.N.Z.C.A , the same as those of “Dr” Brian Kelly.
After a performance like this, perhaps someone should submit a complaint to the New Zealand Broadcasting Standards Authority.
After all, I notice that they have dismissed complaints from one chiropractor, Sean Parker, after a TV programme looked at the business practices of his private chiropractic practice, The Spinal Health Foundation. Perhaps the BSA understands business better than it understands science.
Follow-up
Is chiropractic crumbling in New Zealand? The New Zealand College of Chiropractic featured in my editorial in the New Zealand Medical Journal, and in the fallout from that article, It’s principle, “Dr” Brian Kelly (B App Sci (Chiro)) seems to be getting desperate. His college is now canvassing for recruits in Canada. They are promised all the woo.
- Subluxation centered techniques – Gonstead, Toggle Recoil, Thompson, Diversified
- Traditional philosophy featuring vitalism and innate healing – congruent curriculum
Perhaps Canada is a good place to recruit, gven the $500 million class action being brought against chiropractors in Canada, after Sandra Nette became tetraplegic immediately after a chiropractor manipulated her neck, Canadian chiropractors must be looking for somewhere to hide.
Stuff and Nonsense. jdc described this story at the time the complaint was lodged.
Shaun Holt’s own blog follows the action.
New Zealand Doctor covers the story.
Bay of Plenty Times “Bay researcher slams television complaint ruling“
This is another short interruption in the epic self-destruction of chiropractors. In a sense it is more serious. One expects quacks to advocate quackery. What you don’t expect is that the National Institute of Clinical Excellence (NICE) will endorse it. Neither do you expect the Medicines and Healthcare products Regulatory Agency (MHRA) to betray its mandate to make sure that medicines work.
The saga of the NICE low back pain guidance has been the subject of a deluge of criticism, It seems doubtful that the guidance can survive, not least because of its absurd endorsement of chiropractic, at a time when chiropractic is undergoing self-immolation as a consequence of the persecution of Simon Singh by the British Chiropractic Association (see here, and here, and here, and here and thousands of other sites).
The other betrayal has come to the for after the MHRA approved highly misleading labelling of a homeopathic preparation. At the time,
in 2006, when the principle was approved by the MHRA, just about every scientific organisation, even the Royal Society, condemned the action. What was discouraging that the clinical organisations all stayed silent. It is still a mystery why the MHRA made this enormous mistake, Some said that European regulations required it, but that is quite untrue, as Les Rose has shown. It appears to have been the result of a pusillanimous MHRA bowing to pressure from a deeply unscientific Department of Health (a letter from Caroline Flint at the time borders on the surreal).
On 20 May 2009, the British Medical Journal printed an article Drugs agency grants its first licence to homoeopathic product by Deborah Cohen (available free). The comments were mostly highly critical of the MHRA. The BMJ asked, as it does from time to time, for my comment to be converted to a letter
for the print edition. That isn’t freely available, so here it is.
|
Published 9 June 2009, doi:10.1136/bmj.b2333 LettersHomoeopathic product licenceMHRA label seems to be illegalThe strap line for the Medicines and Healthcare products Regulatory Agency (MHRA) is “We enhance and safeguard the health of the public by ensuring that medicines and medical devices work and are acceptably safe.” Yet the MHRA has made mockery of its own aims by ignoring the bit about “ensuring that medicines work” and allowing Arnica 30C pills to be labelled: “a homoeopathic medicinal product used within the homoeopathic tradition for the symptomatic relief of sprains, muscular aches, and bruising or swelling after contusions.”1 This label should be illegal anyway because the pills contain no trace of the ingredient on the label, but this deceit has been allowed through a legal loophole for a long time now. If you sold strawberry jam that contained not a trace of strawberry you’d be in trouble. But I can see no legal loophole that allows the manufacturers of Arnica 30C to evade the provisions of the Consumer Protection from Unfair Trading Regulations 2008. One of the 31 commercial practices which are in all circumstances considered unfair is “falsely claiming that a product is able to cure illnesses, dysfunction, or malformations.” The consumer protection laws apply to the way that “the average consumer” will interpret the label. The average consumer is unlikely to know that “used within the homoeopathic tradition” is a form of weasel words that actually means “there isn’t a jot of evidence that the medicine works.” Since there is not the slightest evidence that Arnica 30C pills provide symptomatic relief of sprains, etc, the labelling that the MHRA has approved seems to be illegal. The MHRA is not selling anything itself, so I presume that it won’t find itself in court, but anyone who follows its advice could well do so. Cite this as: BMJ 2009;338:b2333 David Colquhoun, research professor1 University College London, London WC1E 6BT Competing interests: None declared. References |
It is, I suppose, just a sign of the chaos that reigns in the multiple agencies and quangos responsible for ‘regulation’ that one arm of government proposes action that a different branch would consider illegal. That is an inevitable consequence of trying to regulate something without first deciding whether it is nonsense or not. The Department of Health appears to be quite incapable of grasping this simple and obvious fact.
Follow-up
Health: best treatments. The Guardian seems to the be picking up BMJ stories and ran this one.
That isn’t my title. It is the title of a post by Richard Lanigan, with whom I’ve been corresponding. He has a major grudge against the General Chiropractic Council. And in particular he is disaffected about the GCC’s chair, Peter Dixon, about whom he has written a lot, I can’t judge the details of his complaints, but they are laid out in detail on his blog, http://chiropracticlive.com/
Particular interest attaches to his recent revelation of a letter that was sent on July 8th to its members by the McTimoney Chiropractic Association. The McTimoney sect of chiropractic are the ‘true believers’ in the most mystical codswallop aspects of the subject. Oddly enough their College has been validated by the University of Wales, I’ve put in a Freedom of Information Act reguest to the University of Wales to see how that happened. Watch this space.
My interpretation of this letter is that it is as near as you can get to an admission, by chiropractors themselves, that many chiropractors make claims that are against the law. And worse still, that the McTimoney Chiropractic Assocation is well aware of that.
News travels fasts in the blogosphere. This item has already appeared today on The Quackometer, The Lay Scientist and Gimpy and on Zeno’s blog. Let’s hope that the news spreads far and wide.
|
Date: 8 June 2009 09:12:18 BDT Subject: FURTHER URGENT ACTION REQUIRED! Dear Member If you are reading this, we assume you have also read the urgent email we sent you last Friday. If you did not read it, READ IT VERY CAREFULLY NOW and – this is most important – ACT ON IT. This is not scaremongering. We judge this to be a real threat to you and your practice. Because of what we consider to be a witch hunt against chiropractors, we are now issuing the following advice: The target of the campaigners is now any claims for treatment that cannot be substantiated with chiropractic research. The safest thing for everyone to do is as follows.
When you have done that, please let us know preferably by email or by phone. This will save our valuable time chasing you to see whether it has been done.
CHECK ALL ENTRIES CAREFULLY AND IF IN DOUBT, CONTACT THE RELEVANT PROVIDER TO REMOVE YOUR INFORMATION. CHECK OUR PREVIOUS EMAILS FOR SPECIFIC ADVICE AND KEY WORDS TO AVOID. KEEP A LOG OF YOUR ACTIONS.
5. Be wary of ‘mystery shopper’ phone calls and ‘drop ins’ to your practice, especially if they start asking about your care of children, or whiplash, or your evidence base for practice. IF YOU DO NOT FOLLOW THIS ADVICE, YOU MAY BE AT RISK FROM PROSECUTION. IF YOU DO NOT FOLLOW THIS ADVICE, THE MCA MAY NOT BE ABLE TO ASSIST YOU WITH ANY PROCEEDINGS. Although this advice may seem extreme or alarmist, its purpose is to protect you. The campaigners have a target of making a complaint against every chiropractor in the UK who they perceive to be in breach of the GCC’s CoP, the Advertising Standards Code and/or Trading Standards. We have discovered that complaints against more than 500 individual chiropractors have been sent to the GCC in the last 24 hours. Whatever you do, do not ignore this email and make yourself one of the victims. Some of our members have not followed our earlier advice and now have complaints made against them. We do not want that to happen to you. Even if you do not have a website, you are still at risk. Our latest information suggests that this group are now going through Yellow Pages entries. Be in no doubt, their intention is to scrutinise every single chiropractor in the UK. The MCA Executive has worked tirelessly over the last week keeping abreast of development and contacting at risk members. We have decided that this is our best course of action to protect you and the Association at this time of heightened tension. This advice is given to you solely to protect you from what we believe is a concerted campaign, and does not imply any wrongdoing on your part or the part of the Association. We believe that our best course of action is simply to withdraw from the battleground until this latest wave of targeting is over. Finally, we strongly suggest you do NOT discuss this with others, especially patients, Firstly it would not be ethical to burden patients with this, though if they ask we hope you now have information with which you can respond. Most importantly, this email and all correspondence from the MCA is confidential advice to MCA members alone, and should not be shared with anyone else. Please be aware that the office phone lines are likely to be busy, so, if you need our help, please send an email to the office and we will get back to you as soon as we can. Yours, Berni Martin MCA Chair. Best wishes, Nicki Nicki Choules-Rowe Administrative Officer – Executive Liaison McTimoney Chiropractic Association Crowmarsh Gifford Wallingford OX10 8DJ Tel : 01491 829494 |

Follow-up
The deleted pages are here. Thanks again to quackometer, here is where you can see the pages that might have been taken down as a result of McTimoney’s letter. I hope they won’t grumble. Really, they sjould never have put them up if they weren’t true, should they?.
Two days ago I wrote NICE falls for Bait and Switch by acupuncturists and chiropractors: it has let down the public and itself
Now the official ‘guidance’ is out, and it is indeed quite as bad as the draft.
The relevant bits now read thus.
- Offer one of the following treatment options, taking into account patient preference: an exercise programme, a course of manual therapy or a course of acupuncture. Consider offering another of these options if the chosen treatment does not result in satisfactory improvement.
- Consider offering a structured exercise programme tailored to the person:
- This should comprise of up to a maximum of 8 sessions over a period of up to 12 weeks.
- Offer a group supervised exercise programme, in a group of up to 10 people.
- A one-to-one supervised exercise programme may be offered if a group programme is not suitable for a particular person.
- Consider offering a course of manual therapy, including spinal manipulation, comprising up to a maximum of nine sessions over a period of up to 12 weeks
- Consider offering a course of acupuncture needling comprising up to a maximum of 10 sessions over a period of up to 12 weeks.
The summary guidance still doesn’t mention chiropractic explicitly, just a coy reference to “spinal manipulation”. At a time when the British Chiropractic Association is busy trying to suppress free speech via the law courts, I guess it isn’t surprising that they don’t like to use the word.
The bias in the recommendations is perhaps not surprising because the guidance development group had a heavy representation from alternative medicine advocates, and of people with a record of what, is, in my view, excessive tolerance of mumbo-jumbo.
Royal College of General Practitioners (RCGP) played a large part in writing the guidance. That is an organisation thar has steadfastly refused to make any sort of sensible statement of policy about magic medicine. It isn’t long since I was told by a senior person at the RCGP that there was nothing odd about neuro-linguistic programming. That does not bode well.
Professor Martin Underwood, Professor of Primary Care Research Warwick Medical School, University of Warwick. Underwood chaired the guidance development group. Martin Underwood is also a GP in Coventry See also the British Osteopathic Association. Underwood was lead author of the BEAM trial (download reprint). It is well worth reading the comments on this trial too. It was a randomised trial (though not, of course, blind).
|
Our main aim was to estimate, for patients consulting their general practitioner with back pain, the effectiveness of adding the following to best care in general practice: a class based exercise programme (“back to fitness”), a package of treatment by a spinal manipulator (chiropractor, osteopath, or physiotherapist), or manipulation followed by exercise Conclusions |
In other words, none of them worked very well. The paper failed to distinguish between manipulation by physiotherapists, chiropractors and osteopaths and so missed a valuable chance to find out whether there is an advantage to employing people from alternative medicine (the very problem that this NICE guidance should have dealt with)
Steve Vogel, another member of the guidance development group, is an osteopath. Osteopathy has cast off its shady origins better than chiropractic, but it remains a largely evidence-free zone, and is still usually classified as alternative medicine.
Peter Dixon DC FCC FBCA is chairman of the General Chiropractic Council and founder of Peter Dixon Associates. They run six chiropractic clinics. The claims made by these clinics on their web site are mostly related to musculo-skeletal conditions (not, all spine-related however). But they also include
“Chiropractic is also suitable for relieving the symptoms of stress, and optimizing the way the body works is one of the best ways of enhancing health and wellbeing.”
I wonder how they could justify that claim? Then we get
A chiropractor is always willing to discuss individual conditions or answer questions in order to assess whether chiropractic may be of benefit.
Thanks for the invitation. I accepted it. After the first two phone calls, I had learned all I needed.
The first of Peter Dixon’s clinics that I called, was asked about my son who was suffeiing from perpetual colic. I asked for advice. I was put through to the chiropractor. Here are some extracts from the conversation.
“I think now it’s termed irritable baby syndrome. . . . . We’ve found chiropractic is very effective for colic . . . . £50 up to 3/4 hour which would involve taking a case history, examining the baby, with regard to seeing how the joints in the spine work because often colic is down to, er um, faulty movement patterns in the spine. We deal with an awful lot of things to do with the frame -how the spine moves -and it’s often problems with the way that the bones of the spine move in infants and babies that is the underlying cause in colicky symptoms. . . usually on the whole, I’ve shot myself in the foot by saying this in the past, if there are -um when I say back problems they’re usually temporary issues -when they are there the response for most babies is quite quick . . . it depends on how it’s related to what’s gone on in the birth process -there is usually some traumatic cause and it usually sets up a problem in the upper neck or the mid-back and that will drive those colic symptoms. . . . Yes it’s quite a straightforward thing we just check the baby’s spine and see if it’s problem we can deal with or not.”
Yes, I think you just shot yourself in the foot again. I have no idea in what fraction of cases a chiropractor would fail to claim that it was a case that they could deal with. At least that possibility was envisaged. But when I asked where he’d refer me to in such case I was told it might be a result of bottle feeding -“what they consume”. So I expect it would have been sent to some sort of “nutritional therapist” who would have used one of their usual battery of unreliable tests for food allergies.
I tried a second clinic in Peter Dixon’s empire and asked if chiropractic could help with asthma.”It can do, depending on what type of asthma you have". After some questions I was asked
“Do you have any general aches and pains otherwise, any tension .problems round the rib cage or thoracic spine . . . There are two things we’d look as chiropractors as to whether we could help or not and that would include the tension round the rib cage -in any type of asthma you’ll become tight round the rib cage and merely by keeping that area loose you’d help to stop the asthma from becoming quite as bad. And the second part is we’d look at the neck area with you to see if there is any restriction there -which houses the nerve supply to the lungs which can be indicated in some asthma cases also.”
I was invited to come for a free screen, so I asked if it usually worked quickly, “It depends what the problem is but you’d need a course I suspect”. £45 for the first appointment then £28 per session. “In most cases you’d need to look at a six to eight session course”.
Would anyone with experience of crying babies or of asthma like to comment on these proposed treatments? They are not my idea of evidence-based treatments and I find it quite surprising that someone who sponsors them is thought appropriate to write guidance for NICE.
This sort of ‘sting’ always makes me feel a bit uneasy, but it seems to be the only way to find out what actually goes on. And what goes on has all the appearance of classic bait and switch. You go in for your backache, and before you know where you are you are being sold a course of treatment to stop your baby crying.
Media follow-up after the NICE announcement
Sadly, I heard that the Today programme (my favourite news programme) was pretty wet. if only their science reporting was as good as their politics reporting.
The 27th May was certainly pretty busy for me, Apart from a couple of local paper interviews, this is what happened,
Sky News TV. Richard Suchet and two cameraman came to UCL and filmed a lot of stuff out of which a 20 second clip was used. And then they grumble that they don’t make money.
BBC TV 6 o’clock News. Similar, but at least only two people this time. Both TV stations spent ages showing pictures of people having needles pushed into them and very little time discussing the problems. A pathetically bad attempt at science reporting. Radio, on the whole, did much better
BBC Three Counties Radio (09.20) Host Ronnie Barbour, The daytime talk shows may be appalling to some of us, but the hosts did a far better job of airing the problems than TV [download the mp3].
Radio 5 Live Victoria Derbyshire [download the mp3]
BBC Radio Sheffield (12.05) was the best talk show by far. First speaker was Steve Vogel, the osteopath from the guidance development group. Although invited by the rather sensible host, Rony, to respond to the idea that a secondary consequence of the guidance would be to introduce hocus-pocus, he steadfastly refused to answer the question. At the end a rather sensible GP summed up the view from the coalface. [play the mp3]
Radio 4 PM programme This excellent early evening news programme is run by Eddie Mair. It was the best interview yet. The other side was put by Martin Underwood, chair of the guidance development group [play the mp3]
Underwood said “the evidence shows that it [acupuncture] works”. I disagree. The evidence shows that acupuncture, in a non-blind comparison with no acupuncture shows a small, variable additional effect that doesn’t last and is of marginal clinical significance, That is not what I call “works”. Underwood then indulges in the subgroup analysis fallacy by asserting that a few people get a large benefit from acupuncture. Or perhaps a few people just happen to get better that day. I was not convinced.
More 4 News TV 20.20 was an interview, with the other side being put by my old friend, George Lewith.
During the introduction, an acupuncturist. Lisa Sherman, ‘explained’ acupuncture in the usual sort of utterly meaningless words that illustrate perfectly the problem.
George Lewith said that “we don’t have a good pretend form of acupuncture”. “We don’t have a good placebo and we can demonstrate that acupuncture is literally twice as effective as conventional care”. The first is simply nonsense: huge efforts have gone into developing good controls in acupuncture studies (see, for example, Barker Bausell’s book, Snake Oil Science). And I hope that George will send the references for his “twice as effective” claim. It seems to me to be nothing short of preposterous.
My conclusions
So what went wrong?
One problem could be regarded as medical arrogance. The fact is that the problem of low back pain has not been solved, either by drugs or anything else. It is a failure of medicine (and of pharmacology). That should be the premise of all discussions, and it smacks of arrogance not to tell people straight out. Of course there are some cases when causes can be identified, and perhaps remedied, usually by surgery, but these are the exceptions not the rule.
One consequence of the inability of medicine to help much is that patients get desperate, and willing to try anything. And of course if they happen to have a remission, that is attributed to the treatment, however preposterous that treatment may have been. Conditions like back pain that come and go unpredictable are a gift for quacks.
Another consequence, for researchers rather than patients, is to clutch at straws. Even small and inconsistent effects are seized on as ‘successes’. This phenomenon seems to be part of the reason for the NICE guidance. Another reason is, almost certainly, the grinding of axes by some of the people who wrote it.
What should be done now?
Professor Sir Michael Rawlins is a sensible chap. He cares about evidence, But it does seem that in this case, he might have taken his eye off the ball, for once. In my opinion, he should restore the reputation of NICE by withdrawing this guidance and starting again.
Follow-up
An interesting document has come my way. It shows the responses of the guidance group to the consultation on the draft guidance. Many people made comments not unlike mone, but they were all brushed aside in a way that looks to me rather partisan. The document appears to have vanished from NICE’s web site, but you can download it here.
Friday 29th May. The Times prints a letter from two consultants in pain medicine, Joan Hestor and Stephen Ward. It says, inter alia
“As experienced pain specialists we feel that NICE has lost its way in publishing these guidelines.”
“We are saddened that NICE has chosen to ignore our important role and promote seemingly unworkable and for the most part clinically ineffective treatments”
Friday 29th May. NICE has had a good reputation in the USA for its important, and usually high-quality, attempts to assess what works and what doesn’t. That makes it all the sadder to see it condemned already from the USA for its latest effort. The excellent Yale neurologist, Steven Novella, has written about it on his Neurologica blog.
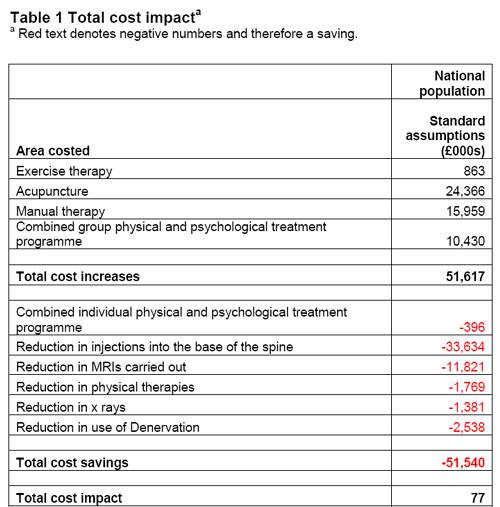
Friday 29th May. A correspondent points out that the costings of the guidance can be found on the NICE web site. Table 1 has a strong air of make-believe.
The Daily Mail (29 May 2009). Their article quotes serious criticisms of NICE.
Dr Ron Cooper, past chairman of the group and a consultant pain specialist in Northern Ireland, said: ‘I have never known so many pain medicine specialists to be so furious. More patients will end up having more expensive surgery, which is unnecessary, risky and has worse results.
‘NICE made it difficult for us to submit evidence to a committee on which there was not one experienced pain physician.
‘The guidelines will make us the laughing stock of Europe, Australia and the U.S. where pain specialists will continue to have full access to a wide range of treatments.’
Chirowatch suspended. 30 May 2009. The invaluable chiro-watch site, http://www.chirowatch.com, run by Dr Canadian physician, Dr Tom Polevoy, has been “suspended”. In fact the whole of his domain, healthwatcher.net, has been disabled. It seems that this was the result of a legal threat to his ISP, not by chiropractors this time, but by William O’Neill of the Canadian Cancer Research Group, which is far from being what the respectable-sounding title suggests, according to Dr Stephen Barrett. The site will be back soon, I’m told. Meanwhile you can read the suspended page here, and the only result of their hamfisted bullying will be to vastly increase the number of people who read it. You can read lots more at Quackwatch’s chirobase and at ebm-first.
A new blog, Not as NICE as you think appeared on May 30th. It is written by a pain physician, Stephen Ward. and is devoted to pointing out the serious problems raised by NICE’s guidance. It starts with the (very critical) World Institute of Pain Press Release.
British Medical Journal has more flak for the NICE guidelines
And the BMJ has published a letter signed by 50 consultants in pain medicine, NICE guidelines on low back pain are flawed.(this will probably appear as a letter in the print edition of the BMJ).
First the MHRA lets down the public by allowing deceptive labelling of sugar pills (see here, and this this blog). Now it is the turn of NICE to betray its own principles.
The National Institute for Health and Clinical Excellence (NICE) describes its job thus
“NICE is an independent organisation responsible for providing national guidance on promoting good health and preventing and treating ill health.”
Its Guidance document on Low Back Pain will be published on Wednesday 27 May 2009, but the newspapers have already started to comment, presumably on the assumption that it will have changed little from the Draft Guidance of September 2008. These comments may have to be changed as soon as the final version becomes available.
The draft guidance, though mostly sensible, has two recommendations that I believe to be wrong and dangerous. The recommendations include (page 7) these three.
- Consider offering a course of manual therapy including spinal manipulation of up to 9 sessions over up to 12 weeks.
- Consider offering a course of acupuncture needling comprising up to 10 sessions over a period of up to 12 weeks.
- Consider offering a structured exercise programme tailored to the individual.
All three of this options are accompanied by a footnote that reads thus.
“A choice of any of these therapies may be offered, taking into account patient preference.”
On the face if it, this might seem quite reasonable. All three choices seem to be about as effective (or ineffective) as each other, so why not let patients choose between them?
Actually there are very good reasons, but NICE does not seem to have thought about them. In the past I have had a high opinion of NICE but it seems that even they are now getting bogged down in the morass of political correctness and officialdom that is the curse of the Department of Health. It is yet another example of DC’s rule number one.
Never trust anyone who uses the word ‘stakeholder’.
They do use it, often.
So what is so wrong?
For a start, I take it that the reference to “spinal manipulation” in the first recommendation is a rather cowardly allusion to chiropractic. Why not say so, if that’s whar you mean? Chiropractic is mentioned in the rest of the report but the word doesn’t seem to occur in the recommendations. Is NICE perhaps nervous that it would reduce the credibility of the report if the word chiropractic were said out loud?
Well, they have a point, I suppose. It would.
That aside, here’s what’s wrong.
The Evidence
I take as my premise that the evidence says that no manipulative therapy has any great advantage over the others. They are all more or less equally effective. Perhaps I should say, more or less equally ineffective, because anyone who claims to have the answer to low back pain is clearly deluded (and I should know: nobody has fixed mine yet). So for effectiveness there are no good grounds to choose between exercise, physiotherapy, acupuncture or chiropractic. There is, though, an enormous cultural difference. Acupuncture and chiropractic are firmly in the realm of alternative medicine. They both invoke all sorts of new-age nonsense for which there isn’t the slightest good evidence. That may not poison your body, but it certainly poisons your mind.
Acupuncturists talk about about “Qi”, “meridians”, “energy flows”. The fact that “sham” and “real” acupuncture consistently come out indistinguishable is surely all the evidence one needs to dismiss such nonsense. Indeed there is a small group of medical acupuncturists who do dismiss it. Most don’t. As always in irrational subjects, acupuncture is riven by internecine strife between groups who differ in the extent of their mystical tendencies,
Chiropractors talk of “subluxations”, an entirely imaginary phenomenon (but a cause of much unnecessary exposure to X-rays). Many talk of quasi-religious things like “innate energy”. And Chiropractic is even more riven by competing factions than acupuncture. See, for example, Chiropractic wars Part 3: internecine conflict.
The bait and switch trick
This is the basic trick used by ‘alternative therapists’ to gain respectability.
There is a superb essay on it by the excellent Yale neurologist Steven Novella: The Bait and Switch of Unscientific Medicine. The trick is to offer some limited and reasonable treatment (like back manipulation for low back pain). This, it seems, is sufficient to satisfy NICE. But then, once you are in the showroom, you can be exposed to all sorts of other nonsense about “subluxations” or “Qi”. Still worse, you will also be exposed to the claims of many chiropractors and acupuncturists to be able to cure all manner of conditions other than back pain. But don’t even dare to suggest that manipulation of the spine is not a cure for colic or asthma or you may find yourself sued for defamation. The shameful legal action of the British Chiropractic Association against Simon Singh (follow it here) led to an addition to DC’s Patients’ Guide to Magic Medicine.
(In the face of such tragic behaviour, one has to be able to laugh).
Libel: A very expensive remedy, to be used only when you have no evidence. Appeals to alternative practitioners because truth is irrelevant.
NICE seems to have fallen for the bait and switch trick, hook line and sinker.
The neglected consequences
Once again, we see the consequences of paying insufficient attention to the Dilemmas of Alternative Medicine.
The lying dilemma
If acupuncture is recommended we will have acupuncturists telling patients about utterly imaginary things like “Qi” and “meridians”. And we will have chiropractors telling them about subluxations and innate energy. It is my opinion that these things are simply make-believe (and that is also the view of a minority of acupuncturist and chiropractors). That means that you have to decide whether the supposed benefits of the manipulation are sufficient to counterbalance the deception of patients.
Some people might think that it was worth it (though not me). What is unforgivable is not to consider even the question. The NICE guidance says not a word about this dilemma. Why not?
The training dilemma
The training dilemma is even more serious. Once some form of alternative medicine has successfully worked the Bait and Switch trick and gained a toehold in the NHS, there will be an army of box-ticking HR zombies employed to ensure that they have been properly trained in “subluxations” or “Qi”. There will be quangos set up to issue National Occupational Standards in “subluxations” or “Qi”. Skills for Health will issue “competences” in “subluxations” or “Qi” (actually they already do). There will be courses set up to teach about “subluxations” or “Qi”, some even in ‘universities’ (there already are).
The respectability problem
But worst of all, it will become possible for aupuncturists and chiropractors to claim that they now have official government endorsement from a prestigious evidence-based organisation like NICE for “subluxations” or “Qi”. Of course this isn’t true. In fact the words “subluxations” or “Qi” are not even mentioned in the draft report. That is the root of the problem. They should have been. But omitting stuff like that is how the Bait and Switch trick works.
Alternative medicine advocates crave, above all, respectability and acceptance. It is sad that NICE seems to have given them more credibility and acceptance without having considered properly the secondary consequences of doing so,
How did this failure of NICE happen?
It seems to have been a combination of political correctness, failure to consider secondary consequences, and excessive influence of the people who stand to make money from the acceptance of alternative medicine.
Take, for example, the opinion of the British Pain Society. This organisation encompasses not just doctors. It
includes “doctors, nurses, physiotherapists, scientists, psychologists, occupational therapists and other healthcare professionals actively engaged in the diagnosis and treatment of pain and in pain research for the benefit of patients”. Nevertheless, their response to the draft guidelines pointed out that the manipulative therapies as a whole were over-represented.
|
Manipulation The guidelines assess 9 large groups of interventions of which manual therapies are only one part. The full GDG members panel of 13 individuals included two proponents of spinal manipulation/mobilisation (P Dixon and S Vogel). In addition, the chair of the panel (M Underwood) is the lead author of the UKBEAM trial on which the positive recommendation for |
It seems that the Pain Society were quite right.
LBC 97.3 Breakfast Show (25 May 2009) had a quick discussion on acupuncture (play mp3 file). After I had my say, the other side was put by Rosey Grandage. She has (among other jobs) a private acupuncture practice so she is not quite as unbiassed as me). As usual, she misrepresents the evidence by failing to distinguish between blind and non-blind studies. She also misrepresented what I said by implying that I was advocating drugs. That was not my point and I did not mention drugs (they, like all treatments, have pretty limited effectiveness, and they have side effects too). She said “there is very good evidence to show they (‘Qi’ and ‘meridians’] exist”. That is simply untrue.
There can’t be a better demonstration of the consequences of falling for bait and switch than the defence mounted by Rosey Grandage. NICE may not mention “Qi” and “meridians”; but the people they want to allow into the NHS have no such compunctions.
I first came across Rosey Grandage when I discovered her contribution to the Open University/BBC course K221. That has been dealt with elsewhere. A lot more information about acupuncture has appeared since then. She doesn’t seem to have noticed it. Has she not seen the Nordic Cochrane Centre report? Nor read Barker Bausell, or Singh & Ernst? Has she any interest in evidence that might reduce her income? Probably not.
Where to find out more
An excellent review of chiropractic can be found at the Layscience site. It was written by the indefatigable ‘Blue Wode’ who has provided enormous amounts of information at the admirable ebm-first site (I am authorised to reveal that ‘Blue Wode’ is the author of that site). There you will also find much fascinating information about both acupuncture and about chiropractic.
I’m grateful to ‘Blue Wode’ for some of the references used here.
Follow-up
Shortly after I published my editorial in the New Zealand Medical Journal, Dr Who?, I was delighted to get a letter from someone who had trained in chiropractic and seen it all from the inside.
Sadly this wonderful letter had to be removed within a few weeks of posting it because its author was threatened and bullied by chiropractors. Its author is too young and too vulnerable to risk his future career. As a result of this shameful and vindictive treatment, I was asked to remove the letter and did so immediately. Other copies on the web have now vanished too.
The experiences described in the letter justified much of what I said in the editorial, and in some ways went further. This letter doubtless contributed to dropping of the threatened legal action by chiropractors against the Journal and against me. The letter was posted originally on 21 August 2008, with the permission of its author. See also the follow-up in Chiropractic wars. Part 3: internecine conflict.
Now I have been sent a much more anonymous version, and it is a great pleasure to post this inside information.
| David
I must begin by stating my background in relation to chiropractic. I am a graduate of a chiropractic college and have practiced for several years. I have elected not to register or practice again and have returned to study to begin a new career. Prior to studying chiropractic, I gained undergraduate and postgraduate qualifications in science. First I would like to address your comment about the validity of a qualification from a private chiropractic college, especially in relation to the difference between studying there and studying at a university. A major difference is the education and experience of faculty. At the time I was there, most of the faculty at my college had only undergraduate qualifications (I would suggest that the American DC degree is of undergraduate level as it is the primary qualifying degree for chiropractic in the US and Canada -it is not the equivalent of a doctorate in a British or Australasian university) and have not published in peer-reviewed journals. This is quite different to my experience of universities where the all of the faculty usually have at least a PhD and are actively involved in research. The content of the chiropractic curriculum was voluminous. It included basic sciences, chiropractic subjects and social sciences. The college I attended did not have any laboratory facilities so the experience of learning science from a textbook was quite different to the way I had been taught at university, where each subject had a significant laboratory program that had to be passed separately to pass the subject. As chiropractic is a clinical discipline, the course contained subjects in common with a medical degree. Sadly, the attitude towards medicine and the medical profession was not always the most constructive. For example, I can recall a noticeboard where newspaper clippings of media reports of medical misadventure and adverse effects of pharmaceuticals were posted regularly. Clinical experience was gained by a 2 year internship in the school health centre concurrent with the last 2 years of academic study; so it was not a full-time internship. The requirements for passing this component of the course were complex but centred around seeing a number of patients, a number of visits, performing a number of various kinds of x-rays and reading a number of x-ray films. Every student was responsible for finding all of their own patients to meet the requirements. The result of this was a clinical experience that was quite narrow for most people. This would seem to be quite different to the hospital internship of a medical degree, the clinical internship of a dental degree or the range of placements in a physiotherapy degree in terms of the breadth of experience of different kinds of patients of different ages and states of health. For people who are not aware, there are a range of ideas within chiropractic about what it is and what it is for. The “wellness”, subluxation-based kind of chiropractic is taught by a minority of schools and is what chiropractors call a “philosophical view”. It advocates that chiropractic care be independent from symptoms or treatment and be a regular part of peoples’ lives. The expectation is that healthy, asymptomatic people will be “adjusted” on a regular basis to keep them free from “vertebral subluxation”. To that end, the training at schools that teach this approach is adequate (and probably even excessive). The issue that you wrote about related to the use of the title “doctor” by chiropractors in New Zealand. In licensing chiropractors and allowing them the use of the title “Dr” in front of their names (provided that the title is qualified by the word “chiropractor”) governments have awarded chiropractors with recognition and prestige that has usually been associated with a level of academic achievement or with a medical qualification. It indicates that the bearer of the title can be trusted to give credible advice within their area of expertise. The issue may seem benign, but in allowing chiropractors to use the title, people who would not normally feel safe to submit to the treatment of an alternative health practitioner, choose to try chiropractic. I make this point because at its core, chiropractic is quite different to medicine, dentistry and physiotherapy. A chiropractic office often looks like a lot like a doctor’s surgery. The layout is similar (with waiting rooms and consultation rooms; there are things like stethoscopes and x-ray machines and there are often informative and education posters and brochures. In many cases, the title “doctor” is used in I have found that some people believe chiropractors are medical doctors. Some even believe that chiropractic is a kind of medical speciality. I have seen patients who choose chiropractic as their primary health care and come to a chiropractic office as their first port of call when they are unwell. I Two practices are of particular concern in some chiropractic offices and in my view; these alone should be sufficient reason to prevent chiropractors from calling themselves “doctor”. The first is the systematic and deliberate erosion of a person’s confidence in the medical system. Many offices have anti medical literature in their libraries. Chiropractors are sometimes taught practices to subvert medical credibility. See http://chirobase.org/20PB/top7.html for an example. The second is a subset of the first but is particularly damaging. It is active opposition to vaccination. At chiropractic school, I was taught anti-vaccination information in my paediatrics course. I have seen books written by chiropractors opposing vaccination and I have seen many offices with anti vaccination leaflets and books in abundance. Now I am all for informed choice but this type of material is rarely accurate or balanced. People are being encouraged not to vaccinate their children by professionals who they believe to be a reliable and prestigious source of information. Although it may sound paternalistic to people who have not had the privilege of clinical practice (albeit in a profession I no longer agree with), it made me realise several things. The first is that people who are unwell are vulnerable. The second is that there are people who trust “medical” advice unquestioningly. I believe we should be very careful about who we title as a credible source of advice about health care. Legislation treads a fine line between limiting personal freedom and protecting people from harm. Aside from the qualification being inconsistent with the academic level that is usually required to use the title “Doctor”, the greatest danger, in my opinion, is that the legal recognition and permission to use the title has allowed chiropractors to assume the mantle of a doctor. In the guise of this respectability, some chiropractors are deliberately eroding confidence in doctors and denying children (and possibly populations) the protection of vaccination. David, thank you for having the courage to question the use of the title “doctor” by chiropractors. Historically (and in your case), chiropractors fight their battles through litigation so it takes personal courage and integrity to do so. |
All I can say is, don’t thank me. It doesn’t take much courage at my age. It takes a lot at yours and the world should be grateful to you.
Replies from chiropractors in the NZMJ
The New Zealand Medical Journal, very properly, allowed right of reply to chiropractore. This week’s issue contains three letters, one of which is from Paul Kelly. It is signed “Dr Brian Kelly B App Sci (Chiro), President, New Zealand College of Chiropractic”. This is not quite the same as appears on his College’s web site which shows the president’s welcome.

It seems that Kelly has not been quite so careful about use of his title on the web site because (as of 21 August) the signature on his address looks like this.

“Dr Brian Kelly, President”. That does seem a bit careless, given that his usage of “Dr” was pointed out in my original editorial, published on 25th July.
Replies to these letters appeared in the September 5th issue of NZMJ.
The publication of Gilbey’s paper and my editorial in the New Zealand Medical Journal (NZMJ) led to a threat of legal action by the NZ Chiropractors’ Association Inc for alleged defamation. After publishing a defiant editorial, the editor of the NZMJ offered chiropractors the chance to put their case.
In the last issue of NZMJ (22 Aug 2008) three letters appeared. One was from Brian Kelly, (President, New Zealand College of Chiropractic) [download letter]. One was from Karl Bale (CEO/Registrar, Chiropractic Board New Zealand) [download letter], and one was from Simon Roughan (Registered Chiropractor and Acting President of the New Zealand Chiropractors’ Association) [download letter].
In the current issue (5 September 2008) Gilbey, Ernst and I responded.{download Gilbey response] [download Ernst response].
Here’s mine. The printed version differs in minor ways [download pdf]
| I’m grateful for the opportunity to reply to the defences of chiropractic from Kelly1, Roughan2 and Bale3 in your last issue.
I’d like first to deal with the minor matter of titles, before getting on to the more important question of vidence. I notice that Brian Kelly signs his letter “Dr Brian Kelly B App Sci (Chiro)” in his letter to NZMJ. He seems to be a bit less careful in his use of titles on his own school’s web site where his president’s welcome4 is signed simply “Dr Brian Kelly”, a title he adopts in at least three other places. Karl Bale3 (CEO/Registrar, Chiropractic Board New Zealand) points out that “Failure to qualify the use of the title ‘Doctor’ may contravene the provisions of the Medical Practitioners Act 1995”. One wonders whether Bale has done anything to stop Kelly’s apparent breaches of this rule? This example makes on wonder whether the Chiropractic Board take its responsibilities seriously? It seems often to be the case that ‘voluntary self-regulation’ doesn’t work, because there are too many vested interests. Karl Bale points out that some ruthless sales methods characteristic of chiropractic are also contrary to the Chiropractic Board’s code of ethics. One would hope their well-known antipathy to vaccination and to medicine as a whole were also considered unethical. These practices seem to continue so the the code of ethics It seems to me quite remarkable that none of the letters mentions the ‘subluxation’ that lies at the heart of their subject6. Could that be because they are reluctant to admit openly that it is a mere metaphysical concept, that no one can see or define? It is sad that so many patients are subjected to X-rays in search of this phantom idea. It is this metaphysical nature of chiropractic that separates it quite clearly from science. Brian Kelly says “How can any reader take seriously, anything suggested by a writer who opines that a 19th Century journalist possessed superior “intellectual standards” to “the UK’s Department of Health” and “several university vice chancellors”. The views of the Davenport Leader on chiropractic were mild compared with those of the great H.L. Mencken (1924)7 who wrote “This preposterous quackery flourishes lushly in the back reaches of the Republic, and begins to conquer the less civilized folk of the big cities….” The problem is that the Department of Health is full of arts graduates who may be very good at classics but can’t understand the nature of evidence. And the UK has one vice-chancellor, a geomorphologist, who defends a course in his university that teaches that “amethysts emit high yin energy”8 I’ll admit, though, that perhaps ‘intellect’ is not what’s deficient in this case, but rather honesty. Your correspondents seem to confuse the duration of a course with its intellectual content. You can study homeopathy for years too, but after all that they are still treating sick people with medicines that contain no medicine. Anyone who works in a university knows that you can easily get accreditation for anything whatsoever if you choose the right people to sit on the committee. I have seen only too many of these worthless pieces of paper. “Amethysts emit high yin energy”8 was part of an accredited course (at the University of Westminster) too. Need I say more? Now to the real heart of the problem, namely the question of evidence. Brian Kelly says that the book by Singh and Ernst9 shows “extreme bias”, but what that book actually shows is an extremely scrupulous regard for evidence, Ernst is in a better position to do this than just about anyone else. He has qualified and practised both regular and alternative medicine, and he was appointed to his present position, as professor of complementary and alternative medicine to assess the evidence. Perhaps most importantly of all, his position allows him to do that assessment with complete lack of bias because, unlike Kelly, his livelihood does not depend on any particular outcome of the assessment. I’m afraid that what Kelly describes as “extreme bias” is simply a display of pique because it has turned out that when all the evidence is examined dispassionately, the outcome is not what chiropractors hoped. The fact of the matter is that when you look at all of the evidence, as Singh & Ernst do, it is perfectly clear that chiropractic is at best no better than conventional treatments even for back pain. For all other conditions its benefits fail to outweigh its risks – contrary to the many claims by chiropractors. Both the New Zealand and the UK governments have got themselves into an impossible position by giving official recognition to chiropractic before the evidence was in. Since the conventional manipulative treatments are cheaper, and may be well be safer, and because they involve no quasi-religious ideas like “subluxation” or “innate intelligence”, the only reasonable conclusion is that there is no need for chiropractic to exist at all. They do nothing they do that could not be done as well by medical practitioners and physiotherapists. What will governments do about that, I wonder? David Colquhoun 1. Kelly, B. New Zealand College of Chiropractic response to 2. Roughan, S. Setting the record straight: New Zealand Chiropractors’ Association response letter. NZMJ 22 3. Bale, 4. http://www.nzchiro.co.nz/about_president.php 6. http://www.chirobase.org/01General/chirosub.html 7. http://www.geocities.com/healthbase/mencken_chiro.html 8. http://dcscience.net/?p=227 9. Singh S, Ernst E. Trick or Treatment. Bantam Press; 2008 |
The wars within chiropractic
Although the chiropractors seem to be rather upset by the criticisms that have been levelled against them, the most interesting war is not between chiropractors and people who think that medicine should not be based on metaphysics. It’s the war within chiropractic itself.
The internecine wars within chiropractic have been going almost from the day it was invented. The (ex-)insider’s view gives us a rare insight into what chiropractic schools actually do. Now support has come from a rather unexpected quarter. An article by five chiropractors has just appeared by Murphy et al. (Chiropractic & Osteopathy, 2008, 16:10).
Although the authors declare that they have “a financial interest in the success” of chiropractic, the changes that they propose are so drastic that, if implemented, tthey would leave little left to distinguish chiropractic from, say, physiotherapy. The authors ask the very pertinent question, ‘why is it that podiatry (chiropody in the UK) is well accepted and chiropractic remains on the controversial fringe of medicine?.. Here are some quotations.
“It is also vital that those chiropractors who dogmatically oppose common public health practices, such as immunization [15] and public water fluoridation, cease such unfounded activity.”
“We are concerned that the common perception (which is well supported, in our experience) that chiropractors are only interested in “selling” a lifetime of chiropractic visits may be one of the primary factors behind our low standing in the minds of members of the public [2].”
“One of the problems that we encounter frequently in our interaction with chiropractic educational institutions is the perpetuation of dogma and unfounded claims. Examples include the concept of spinal subluxation as the cause of a variety of internal diseases and the metaphysical, pseudo-religious idea of “innate intelligence” flowing through spinal nerves, with spinal subluxations impeding this flow. These concepts are lacking in a scientific foundation [27] [28] [29] and should not be permitted to be taught at our chiropractic institutions as part of the standard curriculum. Much of what is passed off as “chiropractic philosophy” is simply dogma [30], or untested (and, in some cases, untestable) theories [27] which have no place in an institution of higher learning, except perhaps in an historical context.”
“The Council on Chiropractic Education requirement of 250 adjustments forces interns to use manipulation on patients whether they need it or not, and the radiographic requirement forces interns to take radiographs on patients whether they need them or not.”
“They [podiatrists] did not invent a “lesion” and a “philosophy” and try to force it on the public. They certainly did not claim that all disease arose from the foot, without any evidence to support this notion. The podiatric medical profession simply did what credible and authoritative professions do [32] – they provided society with services that people actually wanted and needed.”
“In the beginning, DD Palmer invented a lesion, and a theory behind this lesion, and developed a profession of individuals who would become champions of that lesion. This is not what credible professions do.”
“In the interim it [chiropractic] has seen its market share dwindle from 10% of the population [4] to 7.5% [3] [42]. Even amongst patients with back pain, the proportion of patients seeing chiropractors dropped significantly between 1987 and 1997, a period of time in which the proportion seeing both medical doctors and physical therapists increased [43].”
“When an individual consults a member of any of the medical professions, it is reasonably expected that the advice and treatment that he or she receives is based in science, not metaphysics or pseudoscience.”
“The chiropractic profession has an obligation to actively divorce itself from metaphysical explanations of health and disease as well as to actively regulate itself in refusing to tolerate fraud, abuse and quackery, which are more rampant in our profession than in other healthcare professions [46].”
“Podiatric medicine is a science-based profession dedicated to the diagnosis and treatment of foot disorders. Foot reflexology is a metaphysically-based group consisting of non-physicians who believe that many physical disorders arise from the foot. Podiatrists have rejected foot reflexology as an unproven and unscientific practice, and do not consider it part of mainstream podiatric practice.”
“We must finally come to the painful realization that the chiropractic concept of spinal subluxation as the cause of “dis-ease” within the human body is an untested hypothesis [27]. It is an albatross around our collective necks that impedes progress.”
All this, remember, comes from five chiropractors. That looks like all out war between their view of chiropractic and that taught in New Zealand College of Chiropractic, and, in the UK by the three chiropractic colleges in the UK.
Follow-up
A report in the New Zealand Herald (18 September 2008) is rather relevant to all this.
Chiropractor to apologise after patient has stroke
A chiropractor has been recommended to apologise to a woman patient who suffered a stroke after he treated her.
The case report is here.
The Advertising Standards Authority has had a bit to say about chiropractors too.