
Download Lectures on Biostatistics (1971). Corrected and searchable version of Google books edition
Download review of Lectures on Biostatistics (THES, 1973).
cold
Which? Magazine (the UK equivalent of Consumer Reports in the USA) has done it again. They published an excellent article, Health products you don’t need. It’s a worthy successor to their recent debunking of “nutritional therapists”. Most of the products in question, apart from Bach Rescue Remedy Spray, were not outright quackery like homeopathy or "detox" products. Rather they were old-fashioned pharmaceutical products that were quite respectable in the 1950s but which have subsequently been found not to work.

These are the things that were looked at.
- Benylin Chesty Coughs (Non-Drowsy)
- Benylin Tickly Coughs (Non-Drowsy)
- Covonia Herbal Mucus
Cough Syrup - Boots Cold and Flu Relief
Tablets - Adios Slimming Tablets
- Bio-Oil
- Seven Seas Jointcare Be Active
- Bach Rescue Remedy
Spray
It’s an interesting and large category, and its one that I grew up with. My first job, in the 1950s was as an apprentice in Timothy Whites & Taylors Homeopathic Chemists in Grange Road, Birkenhead (you can’t have a much humbler start than that). Don’t worry about he homeopathic bit. We had one homeopathic prescription in two years, which was made up with great hilarity. These were the days before the endarkenment.
We did, however, sell a lot of "tonics" and "cough medicines". Two popular brands were Metatone Tonic and Minadex Tonic. I was quite surprised to discover that they are still on sale. Even in the 1950s I was a bit sceptical about what a "tonic" was supposed to achieve. The term soon became extinct as it was slowly realised that no examples existed.
Here is the bad news. It is scarcely an exaggeration to assert the following.
- Nothing is known that alters the time course of a cold.
- There is nothing that you can buy that will suppress a cough*.
- There is no such thing as a "demulcent" or an "expectorant"
- There is no such thing as a "tonic".
- It would be nice if these things existed, but they are figments of the imagination. Nonetheless they sell by the truckload and vast amounts of money are made by selling them.
[*morphine may have a modest effect, but you can’t buy it]
How can this happen? We have the Medicines and Healthcare products Regulatory Agency (MHRA) is the government agency which is responsible for ensuring that medicines and medical devices work, and are acceptably safe.
Demulcents
In the 1950s this was a more or less respectable term. If you google it now, almost all the references come from herbalists, It is, almost entirely, part of the world of quackery. Apart, that is, from the MHRA. And NHS Evidence. It was surprising to find, in a 2009 document from the MHRA
"Simple cough mixtures containing a demulcent, for example glycerin, and syrup can have a soothing effect by coating the throat and relieving the irritation which causes the cough"
No reference is given, and I’m not aware of the slightest reason to think that there is any such effect. Syrup in your respiratory tract is a bit of a disaster.
But the same document says
There are severe limitations to the efficacy studies given that many of the products were first introduced decades ago. There has been no co-ordinated development program to establish efficacy. What trials there are have not been carried out to current standards.
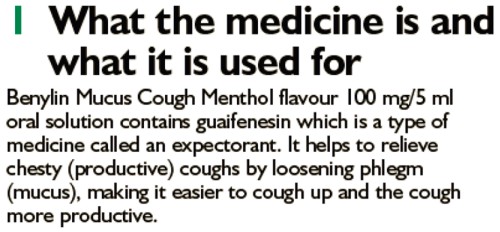
There isn’t much detail about these old ‘remedies’ on the MHRA site. I did find a Publiic Assessment Report for Benylin Mucus Cough Menthol Flavour Oral Solution. The main ingredient is Guaifenesin
The assessment says this.
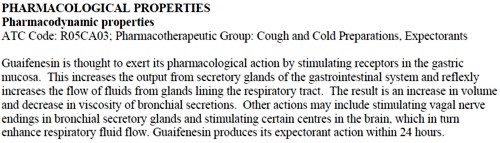
And the approved label says this.
The Public Assessment Report also says
Efficacy
Guaifenesin . . . is a well-established medicinal product with well-known efficacy and safety profiles
This appears to be pure make-believe. There is no credible evidence for any such effect. The report may be dated 2012, but it is a carry-over from a previous age.
In 1976, it was pointed out that none of these things worked (Ziment, 1976), and the situation hasn’t changed. Ziment’s review concludes
"Perhaps this is the one disease that could truly benefit from that oft-touted panacea of therapeutics, the overworked nostrum of materia medica—namely, chicken soup"
A 2012 Cochrane review agrees: "Over-the-counter (OTC) medications for acute cough". This review concludes
"We found no good evidence for or against the effectiveness of over-the-counter (OTC) medications in acute cough, which confirms the findings of two previous reviews (Anonymous 1999; Smith 1993)."
What the MHRA tell me
I was puzzled by the apparently unjustified statements on the MHRA site so I asked them about the eight products that were investigated by Which? magazine (see above). I asked them also about Metatone and Minadex "tonics"
The questions, and the responses can be downloaded here. (I merely asked some reasonable questions, but the MHRA chose to treat them as a request under the Freedom of Information Act).
The first five items all have full marketing authorisation, as do Metatone and Minadex "tonics".
"Metatone (PL-02855/0017), Covonia Herbal Mucus Cough Syrup, Cold and Flu Relief Tablets and Adios Tablets originally held Product Licences of Right. These products were on the market before the Medicines Act 1968 came into force in 1971. These licences were reviewed in the 1980s to ensure that the products were safe, of suitable quality and have evidence of efficacy. Because of the length of time that the products had been on the market they were considered to have well established use and original clinical data to today’s standards was not necessarily available."
The MHRA tell me that they have no copies of the reviews conducted in the 1980s, apart from one. They sent a scanned copy of the August 1988 expert review of Covania syrup (the ingredients have changed since than).
The document is like an antique. It simply repeats the old myths. The names of the "expert reviewers" have been hidden. Given the quality of the review, perhaps that isn’t surprising, but the MHRA should not be so secretive.
There is no such thing as a "tonic", so I asked the MHRA about that too.
Q.5 Can you tell me what criteria the MHRA uses when allowing a product to be advertised as a "tonic"?
R.5 The MHRA assesses proposed product names on a case by case basis. On the basis of the well established use of Minadex Tonic it was decided that the use of the word tonic in the product name was acceptable. For the same reason, it was accepted that Metatone could be referred to as a tonic in the Product Information Leaflet and product labels
In other words, we let them get away with it because it’s old.
I had always understood that when the MHRA grants "Marketing authorisation", that meant there was some guarantee that the product worked. You’d infer that from the MHRA’s own definition.(my emphasis)
"Medicines which meet the standards of safety, quality and efficacy are granted a marketing authorisation (previously a product licence),"
Sadly, it seems that this isn’t true, at least for old-established products, those that were on the market before the Medicines Act (1968) came into force in 1971.
Conclusion
Although old products which were on the market before 1971 were supposed to be reviewed for efficacy and safety. This hasn’t been done efficiently. The make-believe has simply been perpetuated. I have no objection to people buying benylin etc, but they should not have full marketing authorisation and they should be labelled accurately so that it is clear that there is very little evidence that they’ll do you much good. The MHRA has let down the public, just as it did when it allowed misleading labels on homeopathic and herbal potions.
Postscript
After writing this, I discovered a very recent paper about guaifenesin (Seagrave et al, 2012), This paper shows some effects on mucus secretion in cultured human cells (not in humans) with prolonged exposure to concentrations of 30 and 100 µM. This is an order of magnitude greater than the peak blood concentration (7 µM. = 1.4 µg/ml) that is achieved (transiently) in man (Maynard & Bruce, 1970). This is not mentioned in the paper. I’m sure that has nothing to do with what we read at the end of the paper.
Competing interest
JS has received research funds from Reckitt Benckiser. HHA is a consultant to Reckitt Benckiser and is the co-author of a Mucinex sustained-release guaifenesin) patent. DBH has received research funds and consultancy payments from Reckitt Benckiser. DFR has received consultancy payments from Reckitt Benckiser. GS is an employee of Reckitt Benckiser and is also a co-author of a Mucinex (sustained-release guaifenfesin) patent.Acknowledgements
This study was funded by Reckitt Benckiser Healthcare International Ltd. Assistance with manuscript submission was provided by Elements Communications Ltd, supported by Reckitt Benckiser Healthcare International Ltd.
On 15 October 2010, Reckitt Benckiser was fined £10.2 m by the Office of Fair Trading after the company admitted anti-competitive behaviour.
Follow-up
Shortly after this post went up. I was attacked on twitter by @iHealthP. That’s a company, http://www.ihealthpartnership.com (the tweeter declined to reveal their identity). It started thus.
Your article asserts that “There is nothing that will suppress a cough.” This is bollocks, pure & simple.
The interchange was one of those less pleasant Twitter moments (I’ve Storifed some of it in case anyone is interested). The discussion did throw up a few useful references though. @LeCanardNoir pointed out a 2007 paper which concludes
"Clearly the widespread notion that codeine is an effective cough suppressant is not supported by the available evidence."
One of the papers cited by @iHealthP in support of his/her contention that pholcodine and codeine work was Recommendations for the management of cough in adults (from the British Thoracic Society Cough Guideline Group). This paper actually concludes
“There are no effective treatments controlling the cough response per se with an acceptable therapeutic ratio.”
That, of course, is exactly what I said.
There was, however, one reference produced by @iHealthP for which I’m grateful. It doesn’t concern over-the-counter cough treatments (which is what this post is about), but morphine. It does, though, produce some evidence that morphine does work to some extent as a cough suppressant. Amazingly this "well-known truth" was not demonstrated until 2006. The paper, Opiate Therapy in Chronic Cough, by Morice et al., 2006. shows a convincing effect of morphine (5 or 10 mg twice a day) on chronic cough. The main caveat lies in the reported side effects: constipation (40%) and drowsiness (25%). Obvious side-effects can make the trial non-blind. In any case, none of this is relevant to the present post (though I altered the blog to refer to it).