
Download Lectures on Biostatistics (1971). Corrected and searchable version of Google books edition
Download review of Lectures on Biostatistics (THES, 1973).
This article has been re-posted on The Winnower, so it now has a digital object identifier: DOI: 10.15200/winn.142935.50603
The latest news: eating red meat doesn’t do any harm. But why isn’t that said clearly? Alarmism makes better news, not only for journalists but for authors and university PR people too.
I’ve already written twice about red meat.
In May 2009 Diet and health. What can you believe: or does bacon kill you? based on the WCRF report (2007).
In March 2012 How big is the risk from eating red meat now? An update.
In the first of these I argued that the evidence produced by the World Cancer Research Fund (WCRF) for a causal relationship was very thin indeed. An update by WCRF in 2010 showed a slightly smaller risk, and weakened yet further the evidence for causality, though that wasn’t reflected in their press announcement.
The 2012 update added observations from two very large cohort studies. The result was that the estimates of risk were less than half as big as in 2009. The relative risk of dying from colorectal cancer was 1.21 (95% Confidence interval 1.04–1.42) with 50 g of red or processed meat per day, whereas in the new study the relative risk for cancer was only 1.10 (1.06-1.14) for a larger ‘dose’, 85 g of red meat. Again this good news was ignored and dire warnings were issued.
This reduction in size of the effect as samples get bigger is exactly what’s expected for spurious correlations, as described by Ioannidis and others. And it seems to have come true. The estimate of the harm done by red meat has vanished entirely in the latest study.
The EPIC study
This is the European Prospective Investigation into Cancer and Nutrition, another prospective cohort study, so it isn’t randomised [read the original paper]. And it was big, 448,568 people from ten different European countries. These people were followed for a median time of 12.7 years, and during follow-up 26,344 of them died.
The thing that was different about this paper was that red meat was found to pose no detectable risk, as judged by all-cause mortality. But this wasn’t even mentioned in the headline conclusions.
Conclusions: The results of our analysis support a moderate positive association between processed meat consumption and mortality, in particular due to cardiovascular diseases, but also to cancer.
To find the result you have to dig into Table 3.
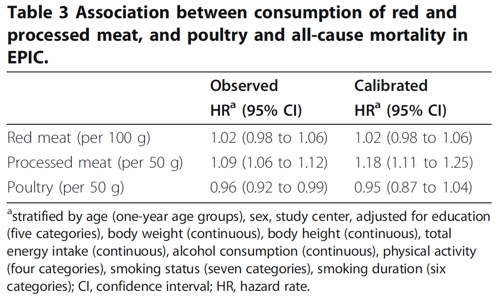
So, by both methods of calculation, the relative risk from eating red meat is negligible (except possibly in the top group, eating more than 160 g (7 oz) per day).
There is still an association between intake of processed meat and all-cause mortality, as in previous studies, though the association of processed meat with all-cause mortality, 1.09, or 1.18 depending on assumptions, is, if anything, smaller than was observed in the 2012 study, in which the relative risk was 1.20 (Table 2).
Assumptions, confounders and corrections.
The lowest meat eaters had only 13% of current smokers, but for the biggest red meat eaters it was 40%, for males. The alcohol consumption was 8.2 g/day for the lowest meat eaters but 23.4 g/day for the highest-meat group (the correlations were a bit smaller for women and also for processed meat eaters).
These two observations necessitate huge corrections to remove the (much bigger) effects of smoking and drinking if we want find the association for meat-eating alone. The main method for doing the correction is to fit the Cox proportional hazards model. This model assumes that there are straight-line relationships between the logarithm of the risk and the amount of each of the risk factors, e.g smoking, drinking, meat-eating and other risk factors. It may also include interactions that are designed to detect whether, for example, the effect of smoking on risk is or isn’t the same for people who drink different amounts.
Usually the straight-line assumption isn’t tested, and the results will depend on which risk factors (and which interactions between them) are included in the calculations. Different assumptions will give different answers. It simply isn’t known how accurate the corrections are when trying to eliminate the big effect of smoking in order to isolate the small effect of meat-eating. And that is before we get to other sorts of correction. For example, the relative risk from processed meat in Table 3, above, was 9% or 18% (1.09, or 1.18) depending on the outcome of a calculation that was intended to increase the accuracy of food intake records ("calibration").
The Conclusions of the new study don’t even mention the new result with red meat. All they mention is the risk from processed meat.
In this population, reduction of processed meat consumption to less than 20 g/day would prevent more than 3% of all deaths. As processed meat consumption is a modifiable risk factor, health promotion activities should include specific advice on lowering processed meat consumption.
Well, you would save that number of lives if, and only if, the processed meat was the cause of death. Too many epidemiologists, the authors pay lip service to the problem of causality in the introduction, but then go on to assume it in the conclusions. In fact the problem of causality isn’t even metnioned anywhere in either the 2012 study, or the new 2013 EPIC trial.
So is the risk of processed meat still real? Of course I can’t answer that. All that can be said is that it’s quite small, and as sample sizes get bigger, estimates of the risk are getting smaller. It wouldn’t be surprising if the risk from processed meat were eventually found not to exist, just as has happened for red (unprocessed) meat
The Japanese study
Last year there was another cohort study, with 51,683 Japanese. The results were even more (non-) dramatic [Nagao et al, 2012] than in the EPIC trial. This is how they summarise the results for the relative risks (with 95% confidence intervals).
"…for the highest versus lowest quintiles of meat consumption (77.6 versus 10.4 g/day) among men were 0.66 (0.45 — 0.97) for ischemic heart disease, 1.10 (0.84 — 1.43) for stroke and 1.00 (0.84 — 1.20) for total cardiovascular disease. The corresponding HRs (59.9 versus 7.5 g/day) among women were 1.22 (0.81 — 1.83), 0.91 (0.70 — 1.19) and 1.07 (0.90 — 1.28). The associations were similar when the consumptions of red meat, poultry, processed meat and liver were examined separately.
CONCLUSION: Moderate meat consumption, up to about 100 g/day, was not associated with increased mortality from ischemic heart disease, stroke or total cardiovascular disease among either gender."
In this study, the more meat (red or processed) you eat, the lower your risk of ischaemic heart disease (with the possible exception of overweight women). The risk of dying from any cardiovascular disease was unrelated to the amount of meat eaten (relative risk 1.0) whether processed meat or not.
Of course it’s possible that things which risky for Japanese people differ from those that are risky for Europeans. It’s also possible that even processed meat isn’t bad for you.
The carnitine study
The latest meat study to hit the headlines didn’t actually look at the effects of meat at all, though you wouldn’t guess that from the pictures of sausages in the headlines (not just in newspapers, but also in NHS Choices). The paper [reprint] was about carnitine, a substance that occurs particularly in beef, with lower amounts in pork and bacon, and in many other foods. The paper showed that bacteria in the gut can convert carnitine to a potentially toxic substance, trimethylamine oxide (TMAO). That harms blood vessels (at least in mice). But to show an effect in human subjects they were given an amount of carnitine equivalent to over 1 lb of steak, hardly normal, even in the USA.
The summary of the paper says it is an attempt to explain "the well-established link between high levels of red meat consumption and CVD [cardiovascular disease] risk". As we have just seen, it seems likely that this risk is far from being “well-established”. There is little or no such risk to explain.
It would be useful to have a diagnostic marker for heart disease, but this paper doesn’t show that carnitine or TMAO) is useful for that. It might also be noted that the authors have a maze of financial interests.
Competing financial interests Z.W. and B.S.L. are named as co-inventors on pending patents held by the Cleveland Clinic relating to cardiovascular diagnostics and have the right to receive royalty payments for inventions or discoveries related to cardiovascular diagnostics from Liposciences. W.H.W.T. received research grant support from Abbott Laboratories and served as a consultant for Medtronic and St. Jude Medical. S.L.H. and J.D.S. are named as co-inventors on pending and issued patents held by the Cleveland Clinic relating to cardiovascular diagnostics and therapeutics patents. S.L.H. has been paid as a consultant or speaker by the following companies: Cleveland Heart Lab., Esperion, Liposciences, Merck & Co. and Pfizer. He has received research funds from Abbott, Cleveland Heart Lab., Esperion and Liposciences and has the right to receive royalty payments for inventions or discoveries related to cardiovascular diagnostics from Abbott Laboratories, Cleveland Heart Lab., Frantz Biomarkers, Liposciences and Siemens.
The practical significance of this work was summed up the dietitian par excellence, Catherine Collins, on the BBC’s Inside Health programme.
Listen to Catherine Collins on carnitine.
She points out that the paper didn’t mean that we should change what we already think is a sensible diet.
At most, it suggests that it’s not a good idea to eat 1 lb steaks very day.
And the paper does suggest that it’s not sensible to take the carnitine supplements that are pushed by every gym. According to NIH
"twenty years of research finds no consistent evidence that carnitine supplements can improve exercise or physical performance in healthy subjects".
Carnitine supplements are a scam. And they could be dangerous.
Follow-up
Another blog on this topic, one from Cancer Research UK also fails to discuss the problem of causality. Neither does it go into the nature (and fallibility) of the corrections for counfounders like smoking and alcohol,. Nevertheless that, and an earlier post on Food and cancer: why media reports are often misleading, are a good deal more realistic than most newspaper reports.

Another well-reasoned scrutiny of a supposedly ‘strong’ study. But the Koeth paper (PMID:23563705) raises more questions than are answered in their push to persuade us that TMAO derived from meat carnitine is an independent biomarker of cardiovascular risk.
First – dietary manipulation aside – was subject selection. Not unsurprisingly only one vegan could be found to participate in this research, but at least we can accurately define their dietary preferences as a “person who does not eat or use any animal or fish products”.
However it’s a different story when it comes to defining the ‘vegetarian’ participants. Vegetarianism in general avoids foodstuffs that involve animal sacrifice. Beyond this basic definition actual practices are highly variable. You may be a lacto-vegetarian (who will take cheese, milk, yoghurt); an ovo-vegetarian (who will eat eggs); a combined vegetarian (lacto-ovo vegetarian) or a vegetarian that eats fish (pescetarian). So herin lies the problem. The authors studiously fail to define the ‘shade’ of vegetarianism their subjects were following, a major oversight and one that would have confounded TMAO measurements if their subjects ate fish or eggs as part of their usual vegetarian diet.
We know that whilst freshwater fish like trout possess negligable TMAO, seawater fish contain a lot – significantly more than meat, gram for gram. TMAO is colourless and odourless, but once a fish has been caught and stored this substance is gradually broken down by bacteria on the fish surface into volatile TMA, the chemical we characterise as smelling ‘fishy’. Interestingly, fresh fish doesn’t smell of much, but keep it a couple of days and bacterial decay yields TMA from TMAO to give fish its taste. Leave it a bit longer, and the concentration of TMA rises so much that we consider the fish to be ‘off’.
http://bit.ly/13UsY9f lists the TMA content of fish.
According to these authors, carnitine – converted to TMAO in our gut – is a heart disease risk. If that were so then fish, which contains a massive amount of TMAO compared to red meat, would prove really harmful to us. Yet we have medical research confirmation for almost three decades that eating fish, at least once a week, appears to protect against both heart failure (PMID:23489806) and heart disease (PMID:21914258) in these population studies.
So – if TMAO really was a problem from meat or fish intake – why should fish prove protective for us, heart wise, when it contains more TMAO than red meat? The answer seems to suggest that for all the hype, TMAO is not a good, independent marker of cardiovascular disease risk.
Of greater interest, given the claims made, is lack of clarification of the dietary patterns of their vegetarian ‘control’ panel? Perhaps they never ate fish or eggs – that would have been a good control group to compare meat eaters with. But if the vegetarians DID eat seafish their dietary TMAO intake would have potentially exceeded the amount converted from carnitine in the meat-eaters at baseline, and should have reflected in raised blood levels – unless of course, fish eating veggies exploit their different gut bacteria groups to rid themselves of TMAO before it hits the plasma. That would be intriguing, but the studious nature of avoiding clarification of their veggie subjects makes me think that there may have been some issue with vegetarian categories, selection and inclusion in the trial that could raise more questions than are answered.
Secondly, the study included several women. Not particularly useful for this study. Delicately, I limit comment to informing readers that blood levels of TMA/TMAO vary naturally according to stage of the menstrual cycle (PMID:17257434). Including premenopausal female veggies in this study to measure TMAO was not really a good idea, unless you kept an eye on their calendar when measuring blood levels.
But what about other potential risks from food? These same authors published work similar to this study two years ago (PMCID:PMC3086762), extending their original hypothesis on carnitine to include other dietary componants – lecithin, betaine and choline – as equally risky, given their ability to be similarly metabolised by bowel bacteria into TMAO. The only problem with this? Cruciferous vegetables, eggs, beans, peanuts, soybean and soya products all belong to this group of choline containing foods which the authors imply could prove a cardiac risk – yet again, we know that this group of foods are cardioprotective (http://bit.ly/YtrXgE) rather than a cardiac risk.
It’s a pity that the media has the attention span of a gnat, as no doubt there are many people out there who now believe that ‘red meat = heart disease”. I’d recommend that that we continue to eat red meat a couple of times a week if we want to, after all, its an excellent source of protein and the dietary iron is readily absorbed, compared to vegetable iron sources. Not only that, but preventing iron deficiency anaemia is one way of ensuring you maintain endurance to perform your cardiovascular fitness routine, not easy to achieve if you’re anaemic, so easily made breathless, less stamina etc
Finally, we eat foods combined in a meal (the ‘food matrix’) rather than single foods. This natural ‘food combining’ is nature’s way of ensuring all the important nutrients and substances derived from food are available to us. Very few of us would sit down to a meal of meat and carnitine supplement, so unless you do, you can, from evidence derived by small clinical studies and large population reviews, that we can safely ignore this information.
Is a future test for TMAO really necessary to determine dietary risk? Even if TMAO was a risk factor (but I don’t believe it is), rather than buy in an expensive test, just ask yourself -‘Do I eat a large-ish portion of red meat 3 or more times a week?’ If your answer is ‘usually, yes’ then consider a couple of fish, egg, or meat-free days to ensure dietary variety within a broad palette of nutrient and non-nutritive beneficial food substances for a long and healthy life.
@RD_UK
Thank you very much for indeed for your excellent comment. I can only apologise for having missed the fact that sea fish contain large amounts of TMA.
Neither had I noticed that already in 2011, the carnitine hypothesis had been debunked and that account has now been updated in a masterly way by Chris Masterjohn. You’ll find a lot more detail there and I thank Gary Taubes for drawing my attention to it.
One lesson one can draw from this concerns the fallibility of the editors of “high impact” journals. The carnitine paper was published in Nature Medicine. The editors and reviewers for that journal were, it seems, also unaware of some basic facts that have been known for some years.
[…] great scientist/blogger David Colquhoun has published his own analysis of the work which I would highly commend to you to […]
I came here via the Guardian Article (which is obviously complete nonsense). However, I don’t think that one can dismiss the link completely. There are several potential mechanistic links which are outlined in the IARC summary, in particular:
– the effect of haem on the epithelium
– the formation of nitrosamines
Especially the latter seems to me quite convincing because processed meat has everything required to form nitrosamines – nitrite and amino groups – and the acid is added in the stomach. There are several studies showing this in humans and rats – but there doesn’t seem to be anyone following this up anymore; perhaps it has become unfashionable?
It’s a shame that fundamental work is misused in such a way – no sensible person would support a meat ban.
@RedMeatCancer
Thanks for the comment. The reason for this post was to point out that there is no detectable association between red meat intake in the huge EPIC survey. A non-zero association is hard to interpret causally as explained in earlier posts. On the other hand zero association (as observed) is much easier to interpret: it means that there is, almost certainly, no effect to explain.
The only endpoint worth considering is getting cancer, or all-cause mortality. Studies of mechanism become interesting only if there is an association with one of them. Since there isn’t, there is nothing to explain.
Plausibility arguments, based on surrogate outcomes in non-humans are notoriously unreliable. It’s always possible to invent more-or-less plausible arguments for almost any effect.
Thank you for your quick reply. But IARC seems to believe that there is an association – and after all they conducted a fairly in-depth review of the evidence. Wouldn’t even a small effect have a huge impact on the population? If I increase the efficiency of a subroutine by 0.5%, it can speed up a programme quite a lot when it is called many times.
I don’t quite understand why studies of mechanism are not interesting if there is no association – surely this is part of fundamental research, isn’t it? I’m confused here because I don’t have the impression that those who claim there is an association (such as for example IARC) don’t appear to me like scaremongers or ignorants. I have read the Lancet summary, and it seems to me reasonably well argued. I can’t obviously interpret the scientific background, but it’s difficult to see why they should get it so wrong.
Official organisations are very slow to change their minds when new evidence comes along. I expect IARC will catch up eventually. Apart from slowness, I suspect that another problem is that they tend to be dominated by nutritionists. They have a vested interest in finding effects, however tiny. And they are reluctant to change the authoritative advice that they gave earlier was wrong. I prefer to interpret the data for myself, which I’ve done in three posts. Please also read the references to Ioannidis’ work.
Concerning studies of mechanism, your question is easy to answer. If there is a effect, then it’s important to investigate the mechanism of that effect. But if there is no effect it makes no sense to look for a mechanism. A mechanism for what?
Thanks – but I don’t have the impression the working group is dominated by nutritionists, there are epidemiologists and toxicologists as well (at least based on those found easily).
I’m no expert, but wouldn’t one want to have nutritionists involved when assessing the impact of food on health? They should be those with the relevant expertise to important aspects of this link – as one would like to have toxicologists, biochemists, statisticians etc.
So I find it difficult to understand why such a group of apparently esteemed scientists (and experts in the field) should get it so wrong – whereas you as a non-expert do not (I hope this is not impertinent – it is really an honest question).
inglés (EE.UU.)
Good morning, thank you very much for all that you contribute and your work. I wished to ask your opinion regarding Cochrane’s current saturated fat reviews which seems to reinforce the view to be cautious about red meat. The recent AHA or ESC guideline reinforces the position of more than just a position of caution.
I fear that Cochrane reviews have a tendency to use bad papers and come up with over-optimistic conclusions. The conclusions may say ‘based on poor quality evidence’ but that bit gets ignored and only the over-optimistic conclusion is cited. In other words, garbage in, garbage out.