
Download Lectures on Biostatistics (1971). Corrected and searchable version of Google books edition
Download review of Lectures on Biostatistics (THES, 1973).
alternative medicine
This piece is almost identical with today’s Spectator Health article.
This week there has been enormously wide coverage in the press for one of the worst papers on acupuncture that I’ve come across. As so often, the paper showed the opposite of what its title and press release, claimed. For another stunning example of this sleight of hand, try Acupuncturists show that acupuncture doesn’t work, but conclude the opposite: journal fails, published in the British Journal of General Practice).
Presumably the wide coverage was a result of the hyped-up press release issued by the journal, BMJ Acupuncture in Medicine. That is not the British Medical Journal of course, but it is, bafflingly, published by the BMJ Press group, and if you subscribe to press releases from the real BMJ. you also get them from Acupuncture in Medicine. The BMJ group should not be mixing up press releases about real medicine with press releases about quackery. There seems to be something about quackery that’s clickbait for the mainstream media.
As so often, the press release was shockingly misleading: It said
Acupuncture may alleviate babies’ excessive crying Needling twice weekly for 2 weeks reduced crying time significantly
This is totally untrue. Here’s why.
|
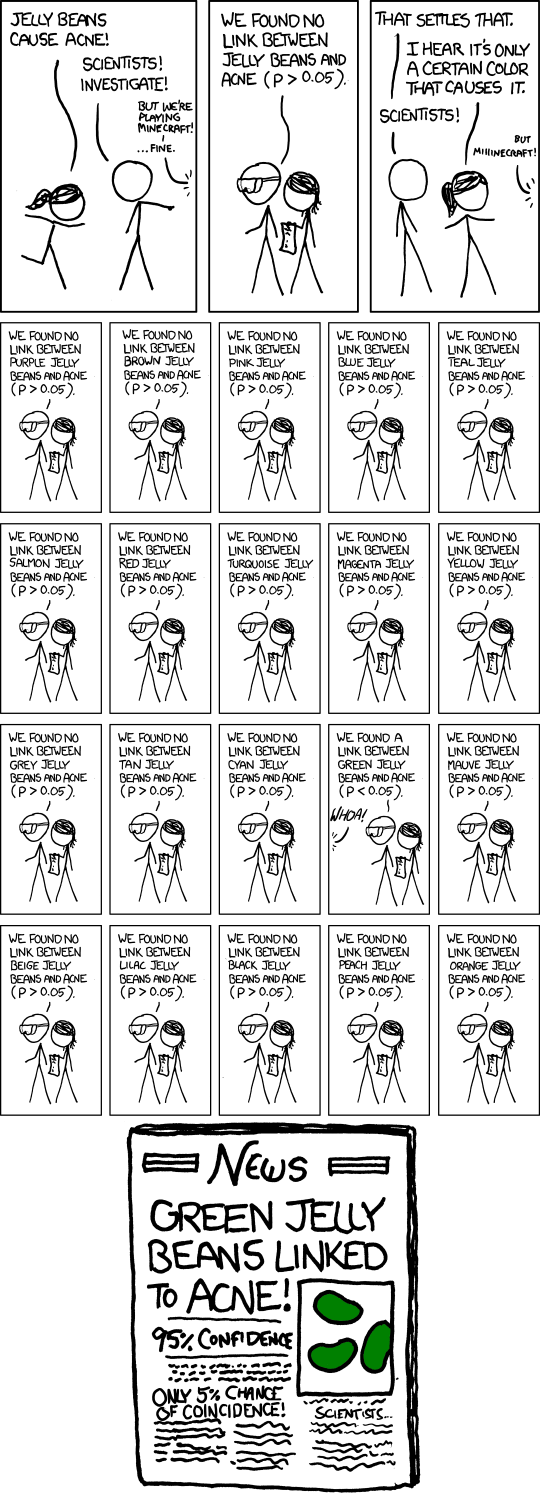
Luckily the Science Media Centre was on the case quickly: read their assessment. The paper made the most elementary of all statistical mistakes. It failed to make allowance for the jelly bean problem. The paper lists 24 different tests of statistical significance and focusses attention on three that happen to give a P value (just) less than 0.05, and so were declared to be "statistically significant". If you do enough tests, some are bound to come out “statistically significant” by chance. They are false postives, and the conclusions are as meaningless as “green jelly beans cause acne” in the cartoon. This is called P-hacking and it’s a well known cause of problems. It was evidently beyond the wit of the referees to notice this naive mistake. It’s very doubtful whether there is anything happening but random variability. And that’s before you even get to the problem of the weakness of the evidence provided by P values close to 0.05. There’s at least a 30% chance of such values being false positives, even if it were not for the jelly bean problem, and a lot more than 30% if the hypothesis being tested is implausible. I leave it to the reader to assess the plausibility of the hypothesis that a good way to stop a baby crying is to stick needles into the poor baby. If you want to know more about P values try Youtube or here, or here. |
|
One of the people asked for an opinion on the paper was George Lewith, the well-known apologist for all things quackish. He described the work as being a "good sized fastidious well conducted study ….. The outcome is clear". Thus showing an ignorance of statistics that would shame an undergraduate.
On the Today Programme, I was interviewed by the formidable John Humphrys, along with the mandatory member of the flat-earth society whom the BBC seems to feel obliged to invite along for "balance". In this case it was professional acupuncturist, Mike Cummings, who is an associate editor of the journal in which the paper appeared. Perhaps he’d read the Science media centre’s assessment before he came on, because he said, quite rightly, that
"in technical terms the study is negative" "the primary outcome did not turn out to be statistically significant"
to which Humphrys retorted, reasonably enough, “So it doesn’t work”. Cummings’ response to this was a lot of bluster about how unfair it was for NICE to expect a treatment to perform better than placebo. It was fascinating to hear Cummings admit that the press release by his own journal was simply wrong.
Listen to the interview here
Another obvious flaw of the study is that the nature of the control group. It is not stated very clearly but it seems that the baby was left alone with the acupuncturist for 10 minutes. A far better control would have been to have the baby cuddled by its mother, or by a nurse. That’s what was used by Olafsdottir et al (2001) in a study that showed cuddling worked just as well as another form of quackery, chiropractic, to stop babies crying.
Manufactured doubt is a potent weapon of the alternative medicine industry. It’s the same tactic as was used by the tobacco industry. You scrape together a few lousy papers like this one and use them to pretend that there’s a controversy. For years the tobacco industry used this tactic to try to persuade people that cigarettes didn’t give you cancer, and that nicotine wasn’t addictive. The main stream media obligingly invite the representatives of the industry who convey to the reader/listener that there is a controversy, when there isn’t.
Acupuncture is no longer controversial. It just doesn’t work -see Acupuncture is a theatrical placebo: the end of a myth. Try to imagine a pill that had been subjected to well over 3000 trials without anyone producing convincing evidence for a clinically useful effect. It would have been abandoned years ago. But by manufacturing doubt, the acupuncture industry has managed to keep its product in the news. Every paper on the subject ends with the words "more research is needed". No it isn’t.
Acupuncture is pre-scientific idea that was moribund everywhere, even in China, until it was revived by Mao Zedong as part of the appalling Great Proletarian Revolution. Now it is big business in China, and 100 percent of the clinical trials that come from China are positive.
if you believe them, you’ll truly believe anything.
Follow-up
29 January 2017
Soon after the Today programme in which we both appeared, the acupuncturist, Mike Cummings, posted his reaction to the programme. I thought it worth posting the original version in full. Its petulance and abusiveness are quite remarkable.
I thank Cummings for giving publicity to the video of our appearance, and for referring to my Wikipedia page. I leave it to the reader to judge my competence, and his, in the statistics of clinical trials. And it’s odd to be described as a "professional blogger" when the 400+ posts on dcscience.net don’t make a penny -in fact they cost me money. In contrast, he is the salaried medical director of the British Medical Acupuncture Society.
It’s very clear that he has no understanding of the error of the transposed conditional, nor even the mulltiple comparison problem (and neither, it seems, does he know the meaning of the word ‘protagonist’).
I ignored his piece, but several friends complained to the BMJ for allowing such abusive material on their blog site. As a result a few changes were made. The “baying mob” is still there, but the Wikipedia link has gone. I thought that readers might be interested to read the original unexpurgated version. It shows, better than I ever could, the weakness of the arguments of the alternative medicine community. To quote Upton Sinclair:
“It is difficult to get a man to understand something, when his salary depends upon his not understanding it.”
It also shows that the BBC still hasn’t learned the lessons in Steve Jones’ excellent “Review of impartiality and accuracy of the BBC’s coverage of science“. Every time I appear in such a programme, they feel obliged to invite a member of the flat earth society to propagate their make-believe.
Acupuncture for infantile colic – misdirection in the media or over-reaction from a sceptic blogger?26 Jan, 17 | by Dr Mike Cummings So there has been a big response to this paper press released by BMJ on behalf of the journal Acupuncture in Medicine. The response has been influenced by the usual characters – retired professors who are professional bloggers and vocal critics of anything in the realm of complementary medicine. They thrive on oiling up and flexing their EBM muscles for a baying mob of fellow sceptics (see my ‘stereotypical mental image’ here). Their target in this instant is a relatively small trial on acupuncture for infantile colic.[1] Deserving of being press released by virtue of being the largest to date in the field, but by no means because it gave a definitive answer to the question of the efficacy of acupuncture in the condition. We need to wait for an SR where the data from the 4 trials to date can be combined. So what about the research itself? I have already said that the trial was not definitive, but it was not a bad trial. It suffered from under-recruiting, which meant that it was underpowered in terms of the statistical analysis. But it was prospectively registered, had ethical approval and the protocol was published. Primary and secondary outcomes were clearly defined, and the only change from the published protocol was to combine the two acupuncture groups in an attempt to improve the statistical power because of under recruitment. The fact that this decision was made after the trial had begun means that the results would have to be considered speculative. For this reason the editors of Acupuncture in Medicine insisted on alteration of the language in which the conclusions were framed to reflect this level of uncertainty. DC has focussed on multiple statistical testing and p values. These are important considerations, and we could have insisted on more clarity in the paper. P values are a guide and the 0.05 level commonly adopted must be interpreted appropriately in the circumstances. In this paper there are no definitive conclusions, so the p values recorded are there to guide future hypothesis generation and trial design. There were over 50 p values reported in this paper, so by chance alone you must expect some to be below 0.05. If one is to claim statistical significance of an outcome at the 0.05 level, ie a 1:20 likelihood of the event happening by chance alone, you can only perform the test once. If you perform the test twice you must reduce the p value to 0.025 if you want to claim statistical significance of one or other of the tests. So now we must come to the predefined outcomes. They were clearly stated, and the results of these are the only ones relevant to the conclusions of the paper. The primary outcome was the relative reduction in total crying time (TC) at 2 weeks. There were two significance tests at this point for relative TC. For a statistically significant result, the p values would need to be less than or equal to 0.025 – neither was this low, hence my comment on the Radio 4 Today programme that this was technically a negative trial (more correctly ‘not a positive trial’ – it failed to disprove the null hypothesis ie that the samples were drawn from the same population and the acupuncture intervention did not change the population treated). Finally to the secondary outcome – this was the number of infants in each group who continued to fulfil the criteria for colic at the end of each intervention week. There were four tests of significance so we need to divide 0.05 by 4 to maintain the 1:20 chance of a random event ie only draw conclusions regarding statistical significance if any of the tests resulted in a p value at or below 0.0125. Two of the 4 tests were below this figure, so we say that the result is unlikely to have been chance alone in this case. With hindsight it might have been good to include this explanation in the paper itself, but as editors we must constantly balance how much we push authors to adjust their papers, and in this case the editor focussed on reducing the conclusions to being speculative rather than definitive. A significant result in a secondary outcome leads to a speculative conclusion that acupuncture ‘may’ be an effective treatment option… but further research will be needed etc… Now a final word on the 3000 plus acupuncture trials that DC loves to mention. His point is that there is no consistent evidence for acupuncture after over 3000 RCTs, so it clearly doesn’t work. He first quoted this figure in an editorial after discussing the largest, most statistically reliable meta-analysis to date – the Vickers et al IPDM.[2] DC admits that there is a small effect of acupuncture over sham, but follows the standard EBM mantra that it is too small to be clinically meaningful without ever considering the possibility that sham (gentle acupuncture plus context of acupuncture) can have clinically relevant effects when compared with conventional treatments. Perhaps now the best example of this is a network meta-analysis (NMA) using individual patient data (IPD), which clearly demonstrates benefits of sham acupuncture over usual care (a variety of best standard or usual care) in terms of health-related quality of life (HRQoL).[3] |
30 January 2017
I got an email from the BMJ asking me to take part in a BMJ Head-to-Head debate about acupuncture. I did one of these before, in 2007, but it generated more heat than light (the only good thing to come out of it was the joke about leprechauns). So here is my polite refusal.
|
Hello Thanks for the invitation, Perhaps you should read the piece that I wrote after the Today programme Why don’t you do these Head to Heads about genuine controversies? To do them about homeopathy or acupuncture is to fall for the “manufactured doubt” stratagem that was used so effectively by the tobacco industry to promote smoking. It’s the favourite tool of snake oil salesman too, and th BMJ should see that and not fall for their tricks. Such pieces night be good clickbait, but they are bad medicine and bad ethics. All the best David |
‘We know little about the effect of diet on health. That’s why so much is written about it’. That is the title of a post in which I advocate the view put by John Ioannidis that remarkably little is known about the health effects if individual nutrients. That ignorance has given rise to a vast industry selling advice that has little evidence to support it.
The 2016 Conference of the so-called "College of Medicine" had the title "Food, the Forgotten Medicine". This post gives some background information about some of the speakers at this event. I’m sorry it appears to be too ad hominem, but the only way to judge the meeting is via the track record of the speakers.

Quite a lot has been written here about the "College of Medicine". It is the direct successor of the Prince of Wales’ late, unlamented, Foundation for Integrated Health. But unlike the latter, its name is disguises its promotion of quackery. Originally it was going to be called the “College of Integrated Health”, but that wasn’t sufficently deceptive so the name was dropped.
For the history of the organisation, see
Don’t be deceived. The new “College of Medicine” is a fraud and delusion
The College of Medicine is in the pocket of Crapita Capita. Is Graeme Catto selling out?
The conference programme (download pdf) is a masterpiece of bait and switch. It is a mixture of very respectable people, and outright quacks. The former are invited to give legitimacy to the latter. The names may not be familiar to those who don’t follow the antics of the magic medicine community, so here is a bit of information about some of them.
The introduction to the meeting was by Michael Dixon and Catherine Zollman, both veterans of the Prince of Wales Foundation, and both devoted enthusiasts for magic medicne. Zollman even believes in the battiest of all forms of magic medicine, homeopathy (download pdf), for which she totally misrepresents the evidence. Zollman works now at the Penny Brohn centre in Bristol. She’s also linked to the "Portland Centre for integrative medicine" which is run by Elizabeth Thompson, another advocate of homeopathy. It came into being after NHS Bristol shut down the Bristol Homeopathic Hospital, on the very good grounds that it doesn’t work.
Now, like most magic medicine it is privatised. The Penny Brohn shop will sell you a wide range of expensive and useless "supplements". For example, Biocare Antioxidant capsules at £37 for 90. Biocare make several unjustified claims for their benefits. Among other unnecessary ingredients, they contain a very small amount of green tea. That’s a favourite of "health food addicts", and it was the subject of a recent paper that contains one of the daftest statistical solecisms I’ve ever encountered
"To protect against type II errors, no corrections were applied for multiple comparisons".
If you don’t understand that, try this paper.
The results are almost certainly false positives, despite the fact that it appeared in Lancet Neurology. It’s yet another example of broken peer review.
It’s been know for decades now that “antioxidant” is no more than a marketing term, There is no evidence of benefit and large doses can be harmful. This obviously doesn’t worry the College of Medicine.
Margaret Rayman was the next speaker. She’s a real nutritionist. Mixing the real with the crackpots is a standard bait and switch tactic.
Eleni Tsiompanou, came next. She runs yet another private "wellness" clinic, which makes all the usual exaggerated claims. She seems to have an obsession with Hippocrates (hint: medicine has moved on since then). Dr Eleni’s Joy Biscuits may or may not taste good, but their health-giving properties are make-believe.
Andrew Weil, from the University of Arizona
gave the keynote address. He’s described as "one of the world’s leading authorities on Nutrition and Health". That description alone is sufficient to show the fantasy land in which the College of Medicine exists. He’s a typical supplement salesman, presumably very rich. There is no excuse for not knowing about him. It was 1988 when Arnold Relman (who was editor of the New England Journal of Medicine) wrote A Trip to Stonesville: Some Notes on Andrew Weil, M.D..
“Like so many of the other gurus of alternative medicine, Weil is not bothered by logical contradictions in his argument, or encumbered by a need to search for objective evidence.”
This blog has mentioned his more recent activities, many times.
Alex Richardson, of Oxford Food and Behaviour Research (a charity, not part of the university) is an enthusiast for omega-3, a favourite of the supplement industry, She has published several papers that show little evidence of effectiveness. That looks entirely honest. On the other hand, their News section contains many links to the notorious supplement industry lobby site, Nutraingredients, one of the least reliable sources of information on the web (I get their newsletter, a constant source of hilarity and raised eyebrows). I find this worrying for someone who claims to be evidence-based. I’m told that her charity is funded largely by the supplement industry (though I can’t find any mention of that on the web site).
Stephen Devries was a new name to me. You can infer what he’s like from the fact that he has been endorsed byt Andrew Weil, and that his address is "Institute for Integrative Cardiology" ("Integrative" is the latest euphemism for quackery). Never trust any talk with a title that contains "The truth about". His was called "The scientific truth about fats and sugars," In a video, he claims that diet has been shown to reduce heart disease by 70%. which gives you a good idea of his ability to assess evidence. But the claim doubtless helps to sell his books.
Prof Tim Spector, of Kings College London, was next. As far as I know he’s a perfectly respectable scientist, albeit one with books to sell, But his talk is now online, and it was a bit like a born-again microbiome enthusiast. He seemed to be too impressed by the PREDIMED study, despite it’s statistical unsoundness, which was pointed out by Ioannidis. Little evidence was presented, though at least he was more sensible than the audience about the uselessness of multivitamin tablets.
Simon Mills talked on “Herbs and spices. Using Mother Nature’s pharmacy to maintain health and cure illness”. He’s a herbalist who has featured here many times. I can recommend especially his video about Hot and Cold herbs as a superb example of fantasy science.
Annie Anderson, is Professor of Public Health Nutrition and
Founder of the Scottish Cancer Prevention Network. She’s a respectable nutritionist and public health person, albeit with their customary disregard of problems of causality.
Patrick Holden is chair of the Sustainable Food Trust. He promotes "organic farming". Much though I dislike the cruelty of factory farms, the "organic" industry is largely a way of making food more expensive with no health benefits.
The Michael Pittilo 2016 Student Essay Prize was awarded after lunch. Pittilo has featured frequently on this blog as a result of his execrable promotion of quackery -see, in particular, A very bad report: gamma minus for the vice-chancellor.
Nutritional advice for patients with cancer. This discussion involved three people.
Professor Robert Thomas, Consultant Oncologist, Addenbrookes and Bedford Hospitals, Dr Clare Shaw, Consultant Dietitian, Royal Marsden Hospital and Dr Catherine Zollman, GP and Clinical Lead, Penny Brohn UK.
Robert Thomas came to my attention when I noticed that he, as a regular cancer consultant had spoken at a meeting of the quack charity, “YestoLife”. When I saw he was scheduled tp speak at another quack conference. After I’d written to him to point out the track records of some of the people at the meeting, he withdrew from one of them. See The exploitation of cancer patients is wicked. Carrot juice for lunch, then die destitute. The influence seems to have been temporary though. He continues to lend respectability to many dodgy meetings. He edits the Cancernet web site. This site lends credence to bizarre treatments like homeopathy and crystal healing. It used to sell hair mineral analysis, a well-known phony diagnostic method the main purpose of which is to sell you expensive “supplements”. They still sell the “Cancer Risk Nutritional Profile”. for £295.00, despite the fact that it provides no proven benefits.
Robert Thomas designed a food "supplement", Pomi-T: capsules that contain Pomegranate, Green tea, Broccoli and Curcumin. Oddly, he seems still to subscribe to the antioxidant myth. Even the supplement industry admits that that’s a lost cause, but that doesn’t stop its use in marketing. The one randomised trial of these pills for prostate cancer was inconclusive. Prostate Cancer UK says "We would not encourage any man with prostate cancer to start taking Pomi-T food supplements on the basis of this research". Nevertheless it’s promoted on Cancernet.co.uk and widely sold. The Pomi-T site boasts about the (inconclusive) trial, but says "Pomi-T® is not a medicinal product".
There was a cookery demonstration by Dale Pinnock "The medicinal chef" The programme does not tell us whether he made is signature dish "the Famous Flu Fighting Soup". Needless to say, there isn’t the slightest reason to believe that his soup has the slightest effect on flu.
In summary, the whole meeting was devoted to exaggerating vastly the effect of particular foods. It also acted as advertising for people with something to sell. Much of it was outright quackery, with a leavening of more respectable people, a standard part of the bait-and-switch methods used by all quacks in their attempts to make themselves sound respectable. I find it impossible to tell how much the participants actually believe what they say, and how much it’s a simple commercial drive.
The thing that really worries me is why someone like Phil Hammond supports this sort of thing by chairing their meetings (as he did for the "College of Medicine’s" direct predecessor, the Prince’s Foundation for Integrated Health. His defence of the NHS has made him something of a hero to me. He assured me that he’d asked people to stick to evidence. In that he clearly failed. I guess they must pay well.
Follow-up
This is my version of a post which I was asked to write for the Independent. It’s been published, though so many changes were made by the editor that I’m posting the original here (below).
Superstition is rife in all sports. Mostly it does no harm, and it might even have a placebo effect that’s sufficient to make a difference of 0.01%. That might just get you a medal. But what does matter is that superstition has given rise to an army of charlatans who are only to willing to sell their magic medicine to athletes, most of whom are not nearly as rich as Phelps.
So much has been said about cupping during the last week
that it’s hard to say much that’s original. Yesterday I did six radio interviews and two for TV, and today Associated Press TV came to film a piece about it. Everyone else must have been on holiday. The only one I’ve checked was the piece on the BBC News channel. That one didn’t seem to go too badly, so it’s here
BBC news coverage
It starts with the usual lengthy, but uninformative, pictures of someone being cupped, The cupper in this case was actually a chiropractor, Rizwhan Suleman. Chiropractic is, of course a totally different form of alternative medicine and its value has been totally discredited in the wake of the Simon Singh case. It’s not unusual for people to sell different therapies with conflicting beliefs. Truth is irrelevant. Once you’ve believed one impossible thing, it seems that the next ones become quite easy.
The presenter, Victoria Derbyshire, gave me a fair chance to debunk it afterwards.
Nevertheless, the programme suffered from the usual pretence that there is a controversy about the medical value of cupping. There isn’t. But despite Steve Jones’ excellent report to the BBC Trust, the media insist on giving equal time to flat-earth advocates. The report, (Review of impartiality and accuracy of the BBC’s coverage of science) was no doubt commissioned with good intentions, but it’s been largely ignored.
Still worse, the BBC News Channel, when it repeated the item (its cycle time is quite short) showed only Rizwhan Suleman and cut out my comments altogether. This is not false balance. It’s no balance whatsoever. A formal complaint has been sent. It is not the job of the BBC to provide free advertising to quacks.
After this, a friend drew my attention to a much worse programme on the subject.
The Jeremy Vine show on BBC Radio 2, at 12.00 on August 10th, 2016. This was presented by Vanessa Feltz. It was beyond appalling. There was absolutely zero attempt at balance, false or otherwise. The guest was described as being am "expert" on cupping. He was Yusef Noden, of the London Hijama Clinic, who "trained and qualified with the Hijama & Prophetic Medicine Institute". No doubt he’s a nice bloke, but he really could use a first year course in physiology. His words were pure make-believe. His repeated statements about "withdrawing toxins" are well know to be absolutely untrue. It was embarrassing to listen to. If you really want to hear it, here is an audio recording.
The Jeremy Vine show
This programme is one of the worst cases I’ve heard of the BBC mis-educating the public by providing free advertising for quite outrageous quackery. Another complaint will be submitted. The only form of opposition was a few callers who pointed out the nonsense, mixed with callers who endorsed it. That is not, by any stretch of the imagination, fair and balanced.
It’s interesting that, although cupping is often associated with Traditional Chinese Medicine, neither of the proponents in these two shows was Chinese, but rather they were Muslim. This should not be surprising as neither cupping nor acupuncture are exclusively Chinese. Similar myths have arisen in many places. My first encounter with this particular branch of magic medicine was when I was asked to make a podcast for “Things Unseen”, in which I debated with a Muslim hijama practitioner and an Indian Ayurvedic practitioner. It’s even harder to talk sense to practitioners of magic medicine who believe that god is on their side, as well as believing that selling nonsense is a good way to make a living.
An excellent history of the complex emergence of similar myths in different parts of the world has been published by Ben Kavoussi, under the title "Acupuncture is astrology with needles".
Now the original version of my blog for the Independent.
Cupping: Michael Phelps and Gwyneth Paltrow may be believers, but the truth behind it is what really sucks
The sight of Olympic swimmer, Michael Phelps, with bruises on his body caused by cupping resulted in something of a media feeding-frenzy this week. He’s a great athlete so cupping must be responsible for his performance, right? Just as cupping must be responsible for the complexion of an earlier enthusiast, Gwyneth Paltrow.
The main thing in common between Phelps and Paltrow is that they both have a great deal of money, and neither has much interest in how you distinguish truth from myth. They can afford to indulge any whim, however silly.
And cupping is pretty silly. It’s a pre-scientific medical practice that started in a time when there was no understanding of physiology, much like bloodletting. Indeed one version does involve a bit of bloodletting. Perhaps bloodletting is the best argument against the belief that it’s ancient wisdom, so it must work. It was a standard part of medical treatment for hundreds of years, and killed countless people.
It is desperately implausible that putting suction cups on your skin would benefit anything, so it’s not surprising that there is no worthwhile empirical evidence that it does. The Chinese version of cupping is related to acupuncture and, unlike cupping, acupuncture has been very thoroughly tested. Over 3000 trials have failed to show any benefit that’s big enough to benefit patients. Acupuncture is no more than a theatrical placebo. And even its placebo effects are too small to be useful.
At least it’s likely that cupping usually does no lasting damage.. We don’t know for sure because in the world of alternative medicine there is no system for recording bad effects (and there is a vested interest in not reporting them). In extreme cases, it can leave holes in your skin that pose a serious danger of infection, but most people probably end up with just broken capillaries and bruises. Why would anyone want that?
The answer to that question seems to be a mixture of wishful thinking about the benefits and vastly exaggerated claims made by the people who sell the product.
It’s typical that the sales people can’t even agree on what the benefits are alleged to be. If selling to athletes, the claim may be that it relieves pain, or that it aids recovery, or that it increases performance. Exactly the same cupping methods are sold to celebs with the claim that their beauty will be improved because cupping will “boost your immune system”. This claim is universal in the world of make-believe medicine, when the salespeople can think of nothing else. There is no surer sign of quackery. It means nothing whatsoever. No procedure is known to boost your immune system. And even if anything did, it would be more likely to cause inflammation and blood clots than to help you run faster or improve your complexion.
It’s certainly most unlikely that sucking up bits of skin into evacuated jars would have any noticeable effect on blood flow in underlying muscles, and so increase your performance. The salespeople would undoubtedly benefit from a first year physiology course.
Needless to say, they haven’t tried to actually measuring blood flow, or performance. To do that might reduce sales. As Kate Carter said recently “Eating jam out of those jars would probably have a more significant physical impact”.
The problem with all sports medicine is that tiny effects could make a difference. When three hour endurance events end with a second or so separating the winner from the rest, that is an effect of less than 0.01%. Such tiny effects will never be detectable experimentally. That leaves the door open to every charlatan to sell miracle treatments that might just work. If, like steroids, they do work, there is a good chance that they’ll harm your health in the long run.
You might be better off eating the jam.
Here is a very small selection of the many excellent accounts of cupping on the web.
There have been many good blogs. The mainstream media have, on the whole, been dire. Here are three that I like,
|
In July 2016, Orac posted in ScienceBlogs. "What’s the harm? Cupping edition". He used his expertise as a surgeon to explain the appalling wounds that can be produced by excessive cupping. |
 Photo from news,com.au |
Timothy Caulfield, wrote "Olympic debunk!". He’s Chair in Health Law and Policy at the University of Alberta, and the author of Is Gwyneth Paltrow Wrong about Everything.
“The Olympics are a wonderful celebration of athletic performance. But they have also become an international festival of sports pseudoscience. It will take an Olympic–sized effort to fight this bunk and bring a win to the side of evidence-based practice.”
Jennifer Raff wrote Pseudoscience is common among elite athletes outside of the Olympics too…and it makes me furious. She works on the genomes of modern and ancient people at the University of Kansas, and, as though that were not a full-time job for most people, she writes blogs, books and she’s also "training (and occasionally competing) in Muay Thai, boxing, BJJ, and MMA".
"I’m completely unsurprised to find that pseudoscience is common among the elite athletes competing in the Olympics. I’ve seen similar things rampant in the combat sports world as well."
What she writes makes perfect sense. Just don’t bother with the comments section which is littered with Trump-like post-factual comments from anonymous conspiracy theorists.
Follow-up
|
“Statistical regression to the mean predicts that patients selected for abnormalcy will, on the average, tend to improve. We argue that most improvements attributed to the placebo effect are actually instances of statistical regression.”
“Thus, we urge caution in interpreting patient improvements as causal effects of our actions and should avoid the conceit of assuming that our personal presence has strong healing powers.” |
In 1955, Henry Beecher published "The Powerful Placebo". I was in my second undergraduate year when it appeared. And for many decades after that I took it literally, They looked at 15 studies and found that an average 35% of them got "satisfactory relief" when given a placebo. This number got embedded in pharmacological folk-lore. He also mentioned that the relief provided by placebo was greatest in patients who were most ill.
Consider the common experiment in which a new treatment is compared with a placebo, in a double-blind randomised controlled trial (RCT). It’s common to call the responses measured in the placebo group the placebo response. But that is very misleading, and here’s why.
The responses seen in the group of patients that are treated with placebo arise from two quite different processes. One is the genuine psychosomatic placebo effect. This effect gives genuine (though small) benefit to the patient. The other contribution comes from the get-better-anyway effect. This is a statistical artefact and it provides no benefit whatsoever to patients. There is now increasing evidence that the latter effect is much bigger than the former.
How can you distinguish between real placebo effects and get-better-anyway effect?
The only way to measure the size of genuine placebo effects is to compare in an RCT the effect of a dummy treatment with the effect of no treatment at all. Most trials don’t have a no-treatment arm, but enough do that estimates can be made. For example, a Cochrane review by Hróbjartsson & Gøtzsche (2010) looked at a wide variety of clinical conditions. Their conclusion was:
“We did not find that placebo interventions have important clinical effects in general. However, in certain settings placebo interventions can influence patient-reported outcomes, especially pain and nausea, though it is difficult to distinguish patient-reported effects of placebo from biased reporting.”
In some cases, the placebo effect is barely there at all. In a non-blind comparison of acupuncture and no acupuncture, the responses were essentially indistinguishable (despite what the authors and the journal said). See "Acupuncturists show that acupuncture doesn’t work, but conclude the opposite"
So the placebo effect, though a real phenomenon, seems to be quite small. In most cases it is so small that it would be barely perceptible to most patients. Most of the reason why so many people think that medicines work when they don’t isn’t a result of the placebo response, but it’s the result of a statistical artefact.
Regression to the mean is a potent source of deception
The get-better-anyway effect has a technical name, regression to the mean. It has been understood since Francis Galton described it in 1886 (see Senn, 2011 for the history). It is a statistical phenomenon, and it can be treated mathematically (see references, below). But when you think about it, it’s simply common sense.
You tend to go for treatment when your condition is bad, and when you are at your worst, then a bit later you’re likely to be better, The great biologist, Peter Medawar comments thus.
|
"If a person is (a) poorly, (b) receives treatment intended to make him better, and (c) gets better, then no power of reasoning known to medical science can convince him that it may not have been the treatment that restored his health"
(Medawar, P.B. (1969:19). The Art of the Soluble: Creativity and originality in science. Penguin Books: Harmondsworth). |
This is illustrated beautifully by measurements made by McGorry et al., (2001). Patients with low back pain recorded their pain (on a 10 point scale) every day for 5 months (they were allowed to take analgesics ad lib).
The results for four patients are shown in their Figure 2. On average they stay fairly constant over five months, but they fluctuate enormously, with different patterns for each patient. Painful episodes that last for 2 to 9 days are interspersed with periods of lower pain or none at all. It is very obvious that if these patients had gone for treatment at the peak of their pain, then a while later they would feel better, even if they were not actually treated. And if they had been treated, the treatment would have been declared a success, despite the fact that the patient derived no benefit whatsoever from it. This entirely artefactual benefit would be the biggest for the patients that fluctuate the most (e.g this in panels a and d of the Figure).
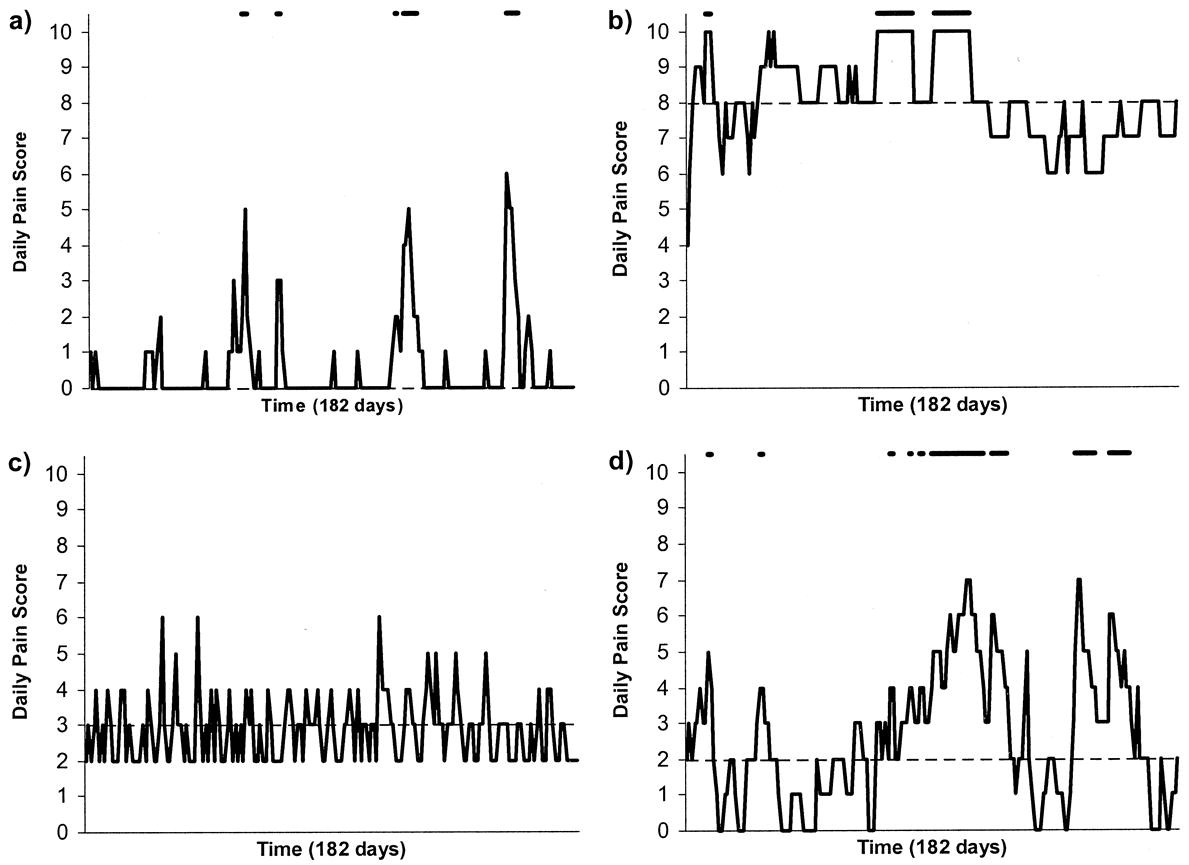
Figure 2 from McGorry et al, 2000. Examples of daily pain scores over a 6-month period for four participants. Note: Dashes of different lengths at the top of a figure designate an episode and its duration.
The effect is illustrated well by an analysis of 118 trials of treatments for non-specific low back pain (NSLBP), by Artus et al., (2010). The time course of pain (rated on a 100 point visual analogue pain scale) is shown in their Figure 2. There is a modest improvement in pain over a few weeks, but this happens regardless of what treatment is given, including no treatment whatsoever.
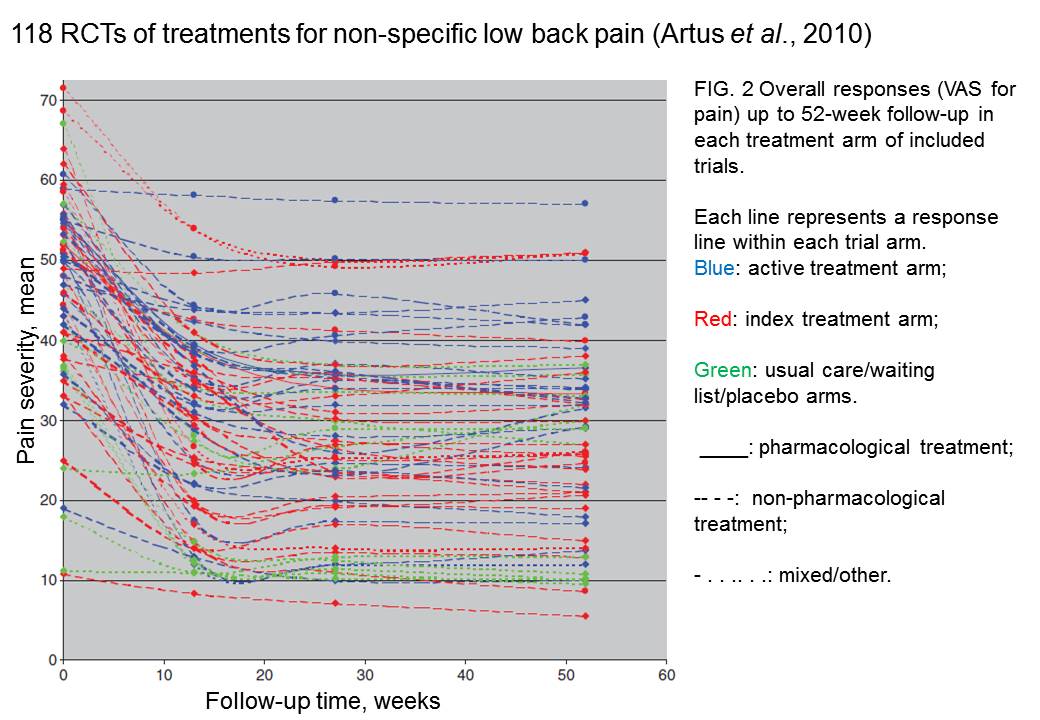
FIG. 2 Overall responses (VAS for pain) up to 52-week follow-up in each treatment arm of included trials. Each line represents a response line within each trial arm. Red: index treatment arm; Blue: active treatment arm; Green: usual care/waiting list/placebo arms. ____: pharmacological treatment; – – – -: non-pharmacological treatment; . . .. . .: mixed/other.
The authors comment
"symptoms seem to improve in a similar pattern in clinical trials following a wide variety of active as well as inactive treatments.", and "The common pattern of responses could, for a large part, be explained by the natural history of NSLBP".
In other words, none of the treatments work.
This paper was brought to my attention through the blog run by the excellent physiotherapist, Neil O’Connell. He comments
"If this finding is supported by future studies it might suggest that we can’t even claim victory through the non-specific effects of our interventions such as care, attention and placebo. People enrolled in trials for back pain may improve whatever you do. This is probably explained by the fact that patients enrol in a trial when their pain is at its worst which raises the murky spectre of regression to the mean and the beautiful phenomenon of natural recovery."
O’Connell has discussed the matter in recent paper, O’Connell (2015), from the point of view of manipulative therapies. That’s an area where there has been resistance to doing proper RCTs, with many people saying that it’s better to look at “real world” outcomes. This usually means that you look at how a patient changes after treatment. The hazards of this procedure are obvious from Artus et al.,Fig 2, above. It maximises the risk of being deceived by regression to the mean. As O’Connell commented
"Within-patient change in outcome might tell us how much an individual’s condition improved, but it does not tell us how much of this improvement was due to treatment."
In order to eliminate this effect it’s essential to do a proper RCT with control and treatment groups tested in parallel. When that’s done the control group shows the same regression to the mean as the treatment group. and any additional response in the latter can confidently attributed to the treatment. Anything short of that is whistling in the wind.
Needless to say, the suboptimal methods are most popular in areas where real effectiveness is small or non-existent. This, sad to say, includes low back pain. It also includes just about every treatment that comes under the heading of alternative medicine. Although these problems have been understood for over a century, it remains true that
|
"It is difficult to get a man to understand something, when his salary depends upon his not understanding it."
Upton Sinclair (1935) |
Responders and non-responders?
One excuse that’s commonly used when a treatment shows only a small effect in proper RCTs is to assert that the treatment actually has a good effect, but only in a subgroup of patients ("responders") while others don’t respond at all ("non-responders"). For example, this argument is often used in studies of anti-depressants and of manipulative therapies. And it’s universal in alternative medicine.
There’s a striking similarity between the narrative used by homeopaths and those who are struggling to treat depression. The pill may not work for many weeks. If the first sort of pill doesn’t work try another sort. You may get worse before you get better. One is reminded, inexorably, of Voltaire’s aphorism "The art of medicine consists in amusing the patient while nature cures the disease".
There is only a handful of cases in which a clear distinction can be made between responders and non-responders. Most often what’s observed is a smear of different responses to the same treatment -and the greater the variability, the greater is the chance of being deceived by regression to the mean.
For example, Thase et al., (2011) looked at responses to escitalopram, an SSRI antidepressant. They attempted to divide patients into responders and non-responders. An example (Fig 1a in their paper) is shown.
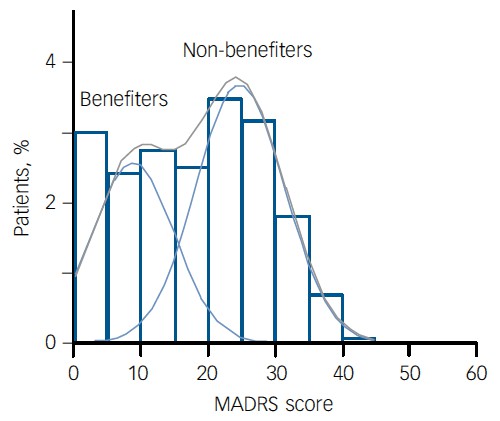
The evidence for such a bimodal distribution is certainly very far from obvious. The observations are just smeared out. Nonetheless, the authors conclude
"Our findings indicate that what appears to be a modest effect in the grouped data – on the boundary of clinical significance, as suggested above – is actually a very large effect for a subset of patients who benefited more from escitalopram than from placebo treatment. "
I guess that interpretation could be right, but it seems more likely to be a marketing tool. Before you read the paper, check the authors’ conflicts of interest.
The bottom line is that analyses that divide patients into responders and non-responders are reliable only if that can be done before the trial starts. Retrospective analyses are unreliable and unconvincing.
Some more reading
Senn, 2011 provides an excellent introduction (and some interesting history). The subtitle is
"Here Stephen Senn examines one of Galton’s most important statistical legacies – one that is at once so trivial that it is blindingly obvious, and so deep that many scientists spend their whole career being fooled by it."
The examples in this paper are extended in Senn (2009), “Three things that every medical writer should know about statistics”. The three things are regression to the mean, the error of the transposed conditional and individual response.
You can read slightly more technical accounts of regression to the mean in McDonald & Mazzuca (1983) "How much of the placebo effect is statistical regression" (two quotations from this paper opened this post), and in Stephen Senn (2015) "Mastering variation: variance components and personalised medicine". In 1988 Senn published some corrections to the maths in McDonald (1983).
The trials that were used by Hróbjartsson & Gøtzsche (2010) to investigate the comparison between placebo and no treatment were looked at again by Howick et al., (2013), who found that in many of them the difference between treatment and placebo was also small. Most of the treatments did not work very well.
Regression to the mean is not just a medical deceiver: it’s everywhere
Although this post has concentrated on deception in medicine, it’s worth noting that the phenomenon of regression to the mean can cause wrong inferences in almost any area where you look at change from baseline. A classical example concern concerns the effectiveness of speed cameras. They tend to be installed after a spate of accidents, and if the accident rate is particularly high in one year it is likely to be lower the next year, regardless of whether a camera had been installed or not. To find the true reduction in accidents caused by installation of speed cameras, you would need to choose several similar sites and allocate them at random to have a camera or no camera. As in clinical trials. looking at the change from baseline can be very deceptive.
Statistical postscript
Lastly, remember that it you avoid all of these hazards of interpretation, and your test of significance gives P = 0.047. that does not mean you have discovered something. There is still a risk of at least 30% that your ‘positive’ result is a false positive. This is explained in Colquhoun (2014),"An investigation of the false discovery rate and the misinterpretation of p-values". I’ve suggested that one way to solve this problem is to use different words to describe P values: something like this.
|
P > 0.05 very weak evidence
P = 0.05 weak evidence: worth another look P = 0.01 moderate evidence for a real effect P = 0.001 strong evidence for real effect |
But notice that if your hypothesis is implausible, even these criteria are too weak. For example, if the treatment and placebo are identical (as would be the case if the treatment were a homeopathic pill) then it follows that 100% of positive tests are false positives.
Follow-up
12 December 2015
It’s worth mentioning that the question of responders versus non-responders is closely-related to the classical topic of bioassays that use quantal responses. In that field it was assumed that each participant had an individual effective dose (IED). That’s reasonable for the old-fashioned LD50 toxicity test: every animal will die after a sufficiently big dose. It’s less obviously right for ED50 (effective dose in 50% of individuals). The distribution of IEDs is critical, but it has very rarely been determined. The cumulative form of this distribution is what determines the shape of the dose-response curve for fraction of responders as a function of dose. Linearisation of this curve, by means of the probit transformation used to be a staple of biological assay. This topic is discussed in Chapter 10 of Lectures on Biostatistics. And you can read some of the history on my blog about Some pharmacological history: an exam from 1959.
It makes a nice change to be able to compliment an official government report.
|
Ever since the House of Lords report in 2000, the government has been vacillating about what should be done about herbalists. At the moment both western herbalists and traditional Chinese medicine (TCM) are essentially unregulated. Many (but not all) herbalists have been pushing for statutory regulation, which they see as government endorsement. It would give them a status like the General Medical Council. |
|
A new report has ruled out this possibility, for very good reasons [download local copy].
Back story (abridged!)
My involvement began with the publication in 2008 of a report on the Regulation of Practitioners of Acupuncture, Herbal Medicine, Traditional Chinese Medicine . That led to my post, A very bad report: gamma minus for the vice-chancellor. The report was chaired by the late Professor Michael Pittilo BSc PhD CBiol FIBiol FIBMS FRSH FLS FRSA, Principal and Vice-Chancellor of The Robert Gordon University, Aberdeen. The membership of the group consisted entirely of quacks and the vice -chancellor’s university ran a course in homeopathy (now closed).
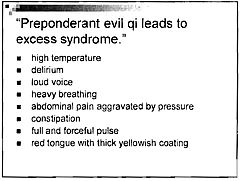
The Pittilo report recommended statutory regulation and "The threshold entry route to the register will normally be through a Bachelor degree with Honours". It ignored entirely the little problem that you can’t run a BSc degree in a subject that’s almost entirely devoid of evidence. It said, for example that acupuncturists must understand " yin/yang, 5 elements/phases, eight principles, cyclical rhythms, qi ,blood and body fluids". But of course there is nothing to "understand"! They are all pre-scientific myths. This “training dilemma” was pointed out in one of my earliest posts, You’d think it was obvious, but nonetheless the then Labour government seemed to take this absurd report seriously.
In 2009 a consultation was held on the Pittilo report. I and many of my friends spent a lot of time pointing out the obvious. Eventually the problem was again kicked into the long grass.
The THR scheme
Meanwhile European regulations caused the creation of the Traditional Herbal Registration (THR) scheme. It’s run by the Medicines and Healthcare products Regulatory Authority (MHRA). This makes it legal to put totally misleading claims on labels of herbal concoctions, as long as they are registered with THR, They also get an impressive-looking certification mark. All that’s needed to get THR registration is that the ‘medicines’ are not obviously toxic and they have been in use for 30 years. There is no need to supply any information whatsoever about whether they work or not. This appears to contradict directly the MHRA’s brief:
"”We enhance and safeguard the health of the public by ensuring that medicines and medical devices work and are acceptably safe."
After much effort, I elicited an admission from the MHRA that there was no reason to think that any herbal concoctions were effective, and that there was nothing to prevent them from adding a statement to say so on the label. They just chose not to do so. That’s totally irresponsible in my opinion. See Why does the MHRA refuse to label herbal products honestly? Kent Woods and Richard Woodfield tell me. Over 300 herbal products have been registered under the THR scheme (a small percentage of the number of products being used). So far only one product of Tibetan medicine and one traditional Chinese medicine have been registered under THR. These are the only ones that can be sold legally now, because no herbs whatsoever have achieved full marketing authorisation -that requires good evidence of efficacy and that doesn’t exist for any herb.
The current report
Eventually, in early 2014, the Tory-led government set up yet another body, "Herbal Medicines and Practitioners Working Group " (HMPWG). My heart sank when I saw its membership (Annex A.2). The vice-chair was none other that the notorious David Tredinnick MP (Con, Bosworth). It was stuffed with people who had vested interests. I wrote to the chair and to the few members with scientific credentials to put my views to them.
But my fears were unfounded, because the report of the HMPWG was not written by the group, but by its chair only. David Walker is deputy chief medical officer and he had clearly listened. Here are some quotations.
The good thing about the European laws is that
"This legislation effectively banned the importation and sale of large-scale manufactured herbal medicine products. This step severely limited the scope of some herbal practitioners to continue practising, particularly those from the Traditional Chinese Medicine (TCM) and Ayurvedic traditions."
The biggest loophole is that
"At present under UK law it is permitted for a herbal practitioner to see individual patients, offer diagnoses and prepare herbal treatments on their own premises, as long as these preparations do not contain banned or restricted substances. This is unchanged by the Traditional Herbal Medicinal Products Directive. "
Walker recognised frankly that there is essentially no good evidence that any herb, western or Chinese, works well enough to make an acceptable treatment. And importantly he, unlike Pittilo, realised that this precludes statutory regulation.
"There are a small number of studies indicating benefit from herbal medicine in a limited range of conditions but the majority of herbal medicine practice is not supported by good quality evidence. A great deal of international, primary research is of poor quality. "
"ts. Herbal medicine practice is therefore currently based upon traditional practice rather than science. It is difficult to differentiate good practice from poor practice on the basis of this evidence in a way that could establish standards for statutory regulation"
The second problem was the harms done by herbs. Herbalists, western and Chinese, have no satisfactory way of reporting side effects
" . . . there is very limited understanding of the risks to patient safety from herbal medicines and herbal practice. A review of safety data was commissioned from HMAC as part of this review. This review identified many anecdotal reports and case studies but little systematically collected data. Most herbal medicine products have not been through the rigorous licensing process that is required of conventional pharmaceutical products to establish their safety and efficacy. Indeed, only a small proportion have even been subject to the less rigorous Traditional Herbal Registration (THR) process. "
"The anecdotal evidence of risk to patients from herbal products in the safety review highlighted the prominence of manufactured herbal medicines in the high profile serious incidents which have been reported in recent years. Many of these reports relate to harm thought to be caused by industrially manufactured herbal products which contained either dangerous herbs, the wrong constituents, toxic contaminants or adulterants. All such industrially manufactured products are now only available under European regulations if their safety is assured through MHRA licensing or THR
accreditation; and specific dangerous herbs have been banned under UK law. This has weakened the case for introduction of statutory regulation as a further safety measure. "
Then Walker identified correctly the training dilemma. Although it seems obvious, this is a big advance for a government document. Degrees that teach nonsense are not good training: they are miseducation.
"The third issue is the identification of educational standards for training practitioners and the benchmarking of standards for accrediting practitioners. With no good data on efficacy or safety, it is difficult for practitioners and patients to understand or quantify the potential benefits and risks of a proposed therapeutic intervention. Training programmes could accredit knowledge and skills in some areas including pharmacology and physiology, professional ethics and infection control but without a credible evidence base relating to the safety and effectiveness of herbal medicine it is hard to see how they could form the basis of accreditation in this field of practice.
There are a number of educational university programmes offering courses in herbal medicine although the number has declined in recent years. Some of these courses are accredited by practitioner organisations which is a potential governance risk as the accreditation may be based on benchmarks established by tradition and custom rather than science.
"
"The herbal medicine sector is in a dilemma" is Walker’s conclusion.
"Some practitioners would like to continue to practise as
they do now, with no further regulation, and accept that their practice is based on tradition and personal experience rather than empirical science. The logical consequence of adopting this form of practice is that we should take a precautionary approach in order to ensure public safety. The public should be protected through consumer legislation to prevent false claims, restricting the use of herbal products which are known to be hazardous to health"
The problem with this is, if course, is that although there is plenty of law, it’s rarely enforced : see Most alternative medicine is illegal Trading Standards very rarely enforce the Consumer Protection Regulations (2008) but Walker is too diplomatic to mention that fact.
"The herbals sector must recognise that its overall approach (including the rationale for use of products and methods of treatment, education and training, and interaction with the NHS) needs to be more science and evidence based if in order to be established as a profession on the same basis as other groups that are statutorily regulated."
So what happens next?
In the short term nothing will happen.
The main mistake has been avoided: there wil be no statutory regulation.
The other options are (a) do nothing, or (b) go for accreditation of a voluntary register (AR) by the Professional Standards Authority for Health and Social Care (PSA). Walker ends up recommending the latter, but only after a lot more work (see pages 28-29 of report). Of particular interest is recommendation 5.
"As a first step it would be helpful for the sector organisations to develop an umbrella voluntary register that could support the development of standards and begin to collaborate on the collection of safety data and the establishment of an academic infrastructure to develop training and research. This voluntary register could in due course seek accreditation from the Professional Standards Authority for Health and Social Care (PSA)."
So it looks as though nothing will happen for a long time, and herbalists and TCM may end up with the utterly ineffectual PSA. After all, the PSA have accredited voluntary registers of homeopaths, so clearly nothing is too delusional for them. It’s very obvious that, unlike Walker, the PSA are quite happy to ignore the training dilemma.
Omissions from the report
Good though this report is, by Department of Health standards, it omits some important points.
Endangered species and animal cruelty aren’t mentioned in the report. Traditional Chinese medicine, and its variants, are responsible for the near-extinction of rhinoceros, tiger and other species because of the superstitious belief that they have medicinal value. It’s not uncommon to find animal parts in Chinese medicines sold in the UK despite it being illegal
And the unspeakably cruel practice of farming bears to collect bile is a direct consequence of TCM.

A bile bear in a “crush cage” on Huizhou Farm, China (Wikipedia)
Statutory regulation of Chiropractors
The same arguments used in Walker’s report to deny statutory regulation of herbalism, would undoubtedly lead to denial of statutory regulation of chiropractors. The General Chiropractic Council was established in 1994, and has a status that’s the same as the General Medical Council. That was a bad mistake. The GCC has not protected the public, in fact it has acted as an advertising agency for chiropractic quackery.
Perhaps Prof. Walker should be asked to review the matter.
Follow-up
You can also read minutes of the HMPWG meetings (and here). But, as usual, all the interesting controversies have been sanitised.
Edzard Ernst has also commented on this topic: Once again: the regulation of nonsense will generate nonsense – the case of UK herbalists.
|
Maurice Nathan Saatchi, Baron Saatchi is an advertising man who, with his brother, Charles Saatchi ("‘why tell the truth when a good lie will do?), became very rich by advertising cigarettes and the Conservative party. After his second wife died of cancer he introduced a private members bill in the House of Lords in 2012. The Medical Innovation Bill came back to the Lords for its second reading on 24 October 2014. |
 |
The debate was deeply depressing: very pompous and mostly totally uninformed. You would never have guessed that the vast majority of those who understand the problem are against the bill. The Bill has failed to win the support of The British Medical Association, The Motor Neurone Disease Association, the Royal College of Physicians, the Royal College of Surgeons, the Medical Research Society, the Royal College of Radiologists, The Medical Defence Union, the Academy of Medical Sciences, the Royal College of Pathologists, the Royal College of General Practitioners, the Academy for Healthcare Science, the Wellcome Trust, Action Against Medical Accidents, and patient advocacy charities Health Watch and the Nightingale Collaboration, and others. Conservative MP Sarah Wollaston, a former GP, has “very serious concerns” about it.
Grief is not a good basis for legislation. In the Daily Telegraph, Lord Saatchi attributes the lack of a "cure for cancer" to fear of litigation.
“Any deviation by a doctor is likely to result in a verdict of guilt for medical negligence. The law defines medical negligence as deviation from that standard procedure. But as innovation is deviation, non-deviation is non-innovation. This is why there is no cure for cancer.”
This statement is utterly bizarre. Evidently Lord Saatchi knows much more about how to sell cigarettes than he does about how to discover new drugs. The reason there is no cure is that it’s a very difficult problem. It has nothing to do with litigation
Almost every medical organisation, and many lawyers, have pointed out the flaws in his ideas,. But slick, and often mendacious, advertising of his cure has deceived many of our scientifically-illiterate parliamentarians, and the bill is making progress
Lord Saatchi’s Bill would allow uncontrolled testing of treatments on any patient. It is not limited to cancer, nor to terminally ill patients (though some amendments, yet to be accepted, might change that). This sort of uncontrolled experimentation is likely to impede advances in treatment rather than to help them. And the vagueness of the wording of the bill could lead to an increase in litigation, rather than the intended decrease.
It is no coincidence that the legion of cancer quacks is in favour of the bill. It opens the door to their nonsense. Big pharma is likely to benefit too, because they will be able to sell improperly tested drugs with little or no effectiveness and immunity from prosecution if they do harm.
For more information about the Bill, see the excellent site, Stop the Saatchi Bill. There are sections on Dispelling Myths, on Professional Concerns, and on the many good articles and blogs that have pointed out the many problems with the bill.
Two recent articles are well worth reading
Saatchi’s ‘Medical Innovation Bill’ will benefit lawyers and charlatans, not patients, by neurologist David Nicholl. And it’s particularly interesting that the Telegraph’s arch-conservative, Peter Oborne has come out strongly against the bill, in The ‘Saatchi Bill’ is dangerous and will bring nothing but harm. I can’t agree with his opening words ("Lord Saatchi is rightly regarded as a national treasure. In his early days he was the advertising genius who played a fundamental role in selling the Thatcherite message"), but I agree entirely with
“The PR campaign distorts the facts, exploiting ignorance and desperation to plant false hope in the rich soil of multiple fallacies.”
“Quacks will be given free rein. No “treatment” is so loopy (or potentially dangerous) that the Saatchi Bill won’t protect doctors who prescribe or administer it from prosecution.”
“The propagation of falsehoods and fallacies surrounding and arising from this Bill will have a corrosive effect on medical ethics and society as a whole.”
Lord Saatchi, who proposed the bill said “To prevent more needless cancer deaths, doctors must be free to innovate”. This statement shows he has no idea of the efforts that go into cancer research. We are doing our best, but it is a very hard problem. In some areas (like breast cancer) there have been big advances. In others areas (e.g. pancreatic or ovarian cancer) there has not yet been any perceptible progress. It will take many more years of hard scientific work. Individual doctors tinkering with speculative untested treatments will not solve the problem.
- The only people who will benefit from the bill will be lawyers, quacks and big pharma.
- “Innovation” is undefined –the bill is based on the myth that there exists a miraculous cure waiting to be found. Sadly, the probability of this happening is vanishingly small.
- To some extent, medicine is victim of its own hype. The public feels it has a right to demand the latest miracle cure. Too often, they don’t exist.
- There is no need for the bill because doctors can already prescribe whatever they want. The Medical Defence Union says it has no reason to think that doctors are deterred from innovating by the fear of litigation.
- The bill won’t help to discover new cures –in fact it is more likely to hinder it, especially if it deters people from joining properly organised clinical trials. The bill will generate many separate anecdotes which may or may not be published. That’s the worst possible way to do research.
- The bill removes protections from patients and is more likely to increase litigation than reduce it.
- Anyone unlucky enough to get cancer is immediately a target for a legion of quacks trying to sell you crazy “treatments”. There is nothing to stop even the lunatic fringe of alternative medicine, homeopaths, promoting their sugar pills. There are, disgracefully, several hundred homeopaths with medical degrees –all a quack has to do is to ask another quack doctor to endorse their daft ideas.
- For untested treatments there is, by definition, no reason to think they’ll do more good than harm. The cancer surgeon, Michael Baum said, rightly, that in cases of terminal cancer "there will be many patients we can’t help. but none we can’t harm".
As a result of tweeting about the bill, I got a call on 21 October from RT TV (UK) asking me speak on the Saatchi Bill. That was a pleasure. Here it is (done from home, on Skype).
And on the day of the Lords debate (24 October 2014) I was asked to talk again about the Saatchi Bill, on the flagship Radio 4 morning news programme, Today. It was only a 3 minute interview with Mishal Husain, but it was unopposed so I managed to get in the main points.
![]() Click to play interview
Click to play interview
This is the Today Programme studio.

The BBC doesn’t pay you, but it’s good at driving you to/from the studio, though the cars are unnecessarily posh. On the way home, I had my first ever ride in an all-electric Tesla. It does 0 – 60 in 4.2 seconds but costs £50k -more than twice the price of a Prius.

|

|
Follow-up
25 October 2014 A summary of the misunderstandings in yesterday’s House of Lords debate: What the Lords Missed.
The consistent failure of ‘regulators’ to do their job has been a constant theme on this blog. There is a synopsis of dozens of them at Regulation of alternative medicine: why it doesn’t work, and never can. And it isn’t only quackery where this happens. The ineptitude (and extravagance) of the Quality Assurance Agency (QAA) was revealed starkly when the University of Wales’ accreditation of external degrees was revealed (by me and by BBC TV Wales, not by the QAA) to be so bad that the University had to shut down.
Here is another example that you couldn’t make up.
|
|
|
Yes, the Professional Standards Authority (PSA) has agreed to accredit that bad-joke pseudo-regulator, the Complementary & Natural Healthcare Council (CNHC, more commonly known as Ofquack)
Ofquack was created at the instigation of HRH the Prince of Wales, at public expense, as a means of protecting the delusional beliefs of quacks from criticism. I worked for them for a while, and know from the inside that their regulation is a bad joke.
When complaints were made about untrue claims made by ‘reflexologists’, the complaints were upheld but they didn’t even reach the Conduct and Competence committee, on the grounds that the reflexologists really believed the falsehoods that they’d been taught. Therefore, by the Humpty Dumpty logic of the CNHC, their fitness to practise was not affected by their untrue claims. You can read the account of this bizarre incident by the person who submitted the complaints, Simon Perry.
In fact in the whole history of the CNHC, it has received a large number of complaints, but only one has ever been considered by their Conduct and Competence Committee. The rest have been dismissed before they were considered properly. That alone makes their claim to be a regulator seem ridiculous.
The CNHC did tell its registrants to stop making unjustified claims, but it has been utterly ineffective in enforcing that ruling. In May 2013, another 100 complaints were submitted and no doubt they will be brushed aside too: see Endemic problems with CNHC registrants..
As I said at the time
It will be fascinating to see how the CNHC tries to escape from the grave that it has dug for itself.
If the CNHC implements properly its own code of conduct, few people will sign up and the CNHC will die. If it fails to implement its own code of conduct it would be shown to be a dishonest sham.
In February of this year (2013), I visited the PSA with colleagues from the Nightingale Collaboration. We were received cordially enough, but they seemed to be bureaucrats with no real understanding of science. We tried to explain to them the fundamental dilemma of the regulation of quacks, namely that no amount of training will help when the training teaches things that aren’t true. They were made aware of all of the problems described above. But despite that, they ended up endorsing the CNHC.
How on earth did the PSA manage to approve an obviously ineffective ‘regulator’?
The job of the PSA is said to be “. . . protecting users of health and social care services and the public”. They (or at least their predecessor, the CHRE), certainly didn’t do that during the saga of the General Chiropractic Council.
The betrayal of reason is catalogued in a PSA document [get local copy]. Here is some nerdy detail.
It is too tedious to go through the whole document, so I’ll deal with only two of its many obvious flaws, the sections that deal with the evidence base, and with training.
The criteria for accreditation state
Standard 6: the organisation demonstrates that there is a defined knowledge base underpinning the health and social care occupations covered by its register or, alternatively, how it is actively developing one. The organisation makes the defined knowledge base or its development explicit to the public.
The Professional Standards Authority recognises that not all disciplines are underpinned by evidence of proven therapeutic value. Some disciplines are subject to controlled randomized trials, others are based on qualitative evidence. Some rely on anecdotes. Nevertheless, these disciplines are legal and the public choose to use them. The Authority requires organisations to make the knowledge base/its development clear to the public so that they may make informed decisions.
Since all 15 occupations that are “regulated” by the CNHC fall into the last category. they “rely on anecdotes”, you would imagine the fact that “The Authority requires organisations to make the knowledge base/its development clear to the public” would mean that the CNHC was required to make a clear statement that reiki, reflexology etc are based solely on anecdote. Of course the CNHC does no such thing. For example, the CNHC’s official definition of reflexology says
Reflexology is a complementary therapy based on the belief that there are reflex areas in the feet and hands which are believed to correspond to all organs and parts of the body
There is, of course, not the slightest reason to think such connections exist, but the CNHC gives no hint whatsoever of that inconvenient fact. The word “anecdote” is used by the PSA but occurs nowhere on the CNHC’s web site.
It is very clear that the CNHC fails standard 6.
But the PSA managed to summon up the following weasel words to get around this glaring failure:
“The professional associations (that verify eligibility for CNHC registration) were actively involved in defining the knowledge base for each of the 15 professions. The Panel further noted that Skills for Health has lead responsibility for writing and reviewing the National Occupational Standards (NOS) for the occupations CNHC registers and that all NOS have to meet the quality criteria set by the UK Commission for Employment and Skills (UKCES), who are responsible for the approval of all NOS across all industry sectors. The Panel considered evidence provided and noted that the applicant demonstrated that there is a defined knowledge base underpinning the occupations covered by its registers. The knowledge base was explicit to the public”.
The PSA, rather than engaging their own brains, simply defer to two other joke organisations, Skills for Health and National Occupational Standards. But it is quite obvious that for things like reiki, reflexology and craniosacral therapy, the “knowledge base” consists entirely of made-up nonsense. Any fool can see that (but not, it seems, the PSA).
Skills for Health lists made-up, HR style, “competencies” for everything under the sun. When I got them to admit that their efforts on distance-healing etc had been drafted by the Prince of Wales’ Foundation, the conversation with Skills for Health became surreal (recorded in January 2008)
DC. Well yes the Prince of Wales would like that. His views on medicine are well known, and they are nothing if not bizarre. Haha are you going to have competencies in talking to trees perhaps?
“You’d have to talk to LANTRA, the land-based organisation for that.”
DC. I’m sorry, I have to talk to whom?
“LANTRA which is the sector council for the land-based industries uh, sector, not with us sorry . . . areas such as horticulture etc.”
DC. We are talking about medicine aren’t we? Not horticulture.
“You just gave me an example of talking to trees, that’s outside our remit ”
You couldn’t make it up, but it’s true. And the Professional Standards Authority rely on what these jokers say.
The current Skills for Health entry for reflexology says
“Reflexology is the study and practice of treating reflex points and areas in the feet and hands that relate to corresponding parts of the body. Using precise hand and finger techniques a reflexologist can improve circulation, induce relaxation and enable homeostasis. These three outcomes can activate the body’s own healing systems to heal and prevent ill health.”
This is crass, made-up nonsense. Of course there are no connections between “areas in the feet and hands that relate to corresponding parts of the body” and no reason to think that reflexology is anything more than foot massage. That a very expensive body, paid for by you and me, can propagate such preposterous nonsense is worrying. That the PSA should rely on them is even more worrying.
National Occupational Standards is yet another organisation that is utterly dimwitted about medical matters, but if you look up reflexology you are simply referred to Skills for Health, as above.
UK Commission for Employment and Skills
(UKCES) is a new one on me. The PSA says that “the UK Commission for Employment and Skills (UKCES), who are responsible for the approval of all NOS across all industry sectors” It is only too obvious that the UKCES leadership team have failed utterly to do their job when it comes to made-up medicine. None of them know much about medicine. It’s true that their chairman did once work for SmithKline Beecham, but as a marketer of Lucozade, a job which anyone with much knowledge of science would not find comfortable..
You don’t need to know much medicine to spot junk. I see no excuse for their failure.
The training problem.
The PSA’s criteria for accreditation say
Standard 9: education and training
The organisation:
9a) Sets appropriate educational standards that enable its registrants to practise competently the occupation(s) covered by its register. In setting its standards the organisation takes account of the following factors:
- The nature and extent of risk to service users and the public
- The nature and extent of knowledge, skill and experience required to provide
service users and the public with good quality careand later
9b) Ensures that registrants who assess the health needs of service users and provide any form of care and treatment are equipped to:
- Recognise and interpret clinical signs of impairment
- Recognise where a presenting problem may mask underlying pathologies
- Have sufficient knowledge of human disease and social determinants of health to identify where service users may require referral to another health or social care professional.
Anyone who imagines for a moment that a reflexologist or a craniosacral therapist is competent to diagnose a subarachnoid haemorrhage or malaria must need their head examining. In any case, the CNHC has already admitted that their registrants are taught things that aren’t true, so more training presumably means more inculcation of myths.
So how does the PSA wriggle out of this? Their response started
“The Panel noted that practitioners must meet, as a minimum, the National Occupational Standards for safe and competent practice. This is verified by the professional associations, who have in turn provided written undertakings to CNHC affirming that there are processes in place to verify the training and skills outcomes of their members to the NOS”
Just two problems there. The NOS standards themselves are utterly delusional. And checking them is left to the quacks themselves. To be fair, the PSA weren’t quite happy with this, but after an exchange of letters, minor changes enabled the boxes to be ticked and the PSA said “The Panel was now satisfied from the evidence provided, that this Standard had been
met”.
What’s wrong with regulators?
This saga is typical of many other cases of regulators doing more harm than good. Regulators are sometimes quacks themselves, in which case one isn’t surprised at their failure to regulate.
But organisations like the Professional Standards Authority and Skills for Health are not (mostly) quacks themselves. So how do they end up giving credence to nonsense? I find that very hard to comprehend, but here are a few ideas.
(1) They have little scientific education and are not really capable of critical thought
(2) Perhaps even more important, they lack all curiosity. It isn’t very hard to dig under the carapace of quack organisations, but rather than finding out for themselves, the bureaucrats of the PSA are satisfied by reassuring letters that allow them to tick their boxes and get home.
(3) A third intriguing possibility is that people like the PSA yield to political pressure. The Department of Health is deeply unscientific and clearly has no idea what to do about alternative medicine. They have still done nothing at all about herbal medicine, traditional Chinese medicine or homeopathy, after many years of wavering. My guess is that they see the CNHC as an organisation that gives the appearance that they’ve done something about reiki etc. I wonder whether they applied pressure to the PSA to accredit CNHC, despite it clearly breaking their own rules. I have sent a request under the Freedom of Information Act in an attempt to discover if the Department of Health has misbehaved in the way it did when it attempted to override NHS Choices.
The responsibility for this cock-up has to rest squarely on the shoulders of the PSA’s director, Harry Cayton. He was director of the CHRE from which PSA evolved and is the person who so signally failed to do anything about the General Chiropractic Council fiasco,
What can be done?
This is just the latest of many examples of regulators who not only fail to help but actually do harm by giving their stamp of approval to mickey mouse organisations like the CNHC. Most of the worst quangos survived the “bonfire of the quangos”.. The bonfire should have started with the PSA, CNHC and Skills for Health. They cost a lot and do harm.
There is a much simpler answer. There is a good legal case that much of alternative medicine is illegal. All one has to do is to enforce the existing law. Nobody would object to quacks if they stopped making false claims (though whether they could stay in business if they stopped exaggerating is debatable). There is only one organisation that has done a good job when it comes to truthfulness. That is the Advertising Standards Authority. But the ASA can do nothing apart from telling people to change the wording of their advertisements, and even that is often ignored.
The responsibility for enforcing the Consumer Protection Law is Trading Standards. They have consistently failed to do their job (see Medico-Legal Journal, Rose et al., 2012. “Spurious Claims for Health-care Products“.
If they did their job of prosecuting people who defraud the public with false claims, the problem would be solved.
But they don’t, and it isn’t.
Follow-up
The indefatigable Quackometer has wriiten an excellent account of the PSA fiasco
Despite the First Amendment in the US and a new Defamation Act in the UK, fear of legal threats continue to suppress the expression of honest scientific opinion.
I was asked by Nature Medicine (which is published in the USA) to write a review of Paul Offit’s new book. He’s something of a hero, so of course I agreed. The editor asked me to make some changes to the first draft, which I did. Then the editor concerned sent me this letter.
|
Thank you for the revised version of the book review.
The chief editor of the journal took a look at your piece, and he thought that it would be a good idea to run it past our legal counsel owing to the strong opinions expressed in the piece in relation to specific individuals. I regret to say that the lawyers have advised us against publishing the review. |
After that I tried the UK Conversation. They had done a pretty good job with my post on the baleful influence of royals on medicine. They were more helpful then Nature Medicine, but for some reason that I can’t begin to understand, they insisted that I should not name Nature Medicine, but to refer only to "a leading journal". And they wanted me not to name Harvard in the last paragraph. I’m still baffled about why. But it seemed to me that editorial interference had gone too far, so rather than have an editor re-write my review, I withdrew it.
It is precisely this sort of timidity that allows purveyors of quackery such success with their bait and switch tactics. The fact that people seem so terrified to be frank must be part of the reason why Harvard, Yale and the rest have shrugged their shoulders and allowed nonsense medicine to penetrate so deeply into their medical schools. It’s also why blogs now are often better sources of information than established journals.
Here is the review. I see nothing defamatory in it.
Do You Believe in Magic? The Sense and Nonsense of Alternative Medicine
|
Paul A. Offit Reviewed by David Colquhoun Research Professor of Pharmacology, UCL. |
|
Here’s an odd thing. There is a group of people who advocate the silly idea that you can cure all ills by stuffing yourself with expensive pills, made by large and unscrupulous Pharma companies. No, I’m not talking about pharmacologists or doctors or dietitians. They mostly say that stuffing yourself with pills is often useless and sometimes harmful, because that’s what the evidence says .
Rather, the pill pushers are the true believers in the alternative realities of the “supplement” industry. They seem blithely unaware that the manufacturers are mostly the same big pharma companies that they blame for trying to suppress “natural remedies”. Far from trying to suppress them, pharma companies love the supplement industry because little research is needed and there are few restrictions on the claims that can be made.
Paul Offit’s excellent book concentrates on alternative medicine in the USA, with little mention of the rest of the world. He describes how American pork barrel politics have given supplement hucksters an almost unrestricted right to make stuff up.
Following the thalidomide tragedy, which led to birth defects in babies in the 1950s and 60s, many countries passed laws that required evidence that a drug was both effective and safe before it could be sold. This was mandate by the Kefauver-Harris amendment (1961) in the USA and the Medicines Act (1968) in the UK. Laws like that upset the quacks, and in the UK the quacks got a free pass, a ‘licence of right‘, largely still in existence.
|
In order to sell a herbal concoction in the UK you need to present no evidence at all that it works, just evidence of safety, in return for which you get a reassuring certification mark and freedom to use misleading brand names and labels. |
 Tradional herbal mark |
In the USA the restrictions didn’t last long. Offit describes how a lobby group for vitamin sellers, the National Health Federation, had a board made up of quacks, some of whom, according to Offit (page 73) had convictions. They found an ally in Senator William Proxmire who introduced in 1975 an amendment that banned the Food and Drugs Administration (FDA) from regulating the safety of megavitamins. Tragically, this bill was even supported by the previously-respected scientist Linus Pauling. Offit tells us that “to Proxmire” became a verb meaning to obstruct science for political gain.
The author then relates how the situation got worse with the passage of the Dietary Supplement Health and Education Act (DSHEA) in 1994. It was passed with the help of ex-vitamin salesman Senator Orin Hatch and lots of money from the supplement industry.
This act iniquitously defined a “supplement” as “a product intended to supplement the diet that bears or contains one or more of the following ingredients: a vitamin, a mineral, an herb or other botanical, or an amino acid”. At a stroke, herbs were redefined as foods. There was no need to submit any evidence of either efficacy or even of safety, before marketing anything. All a manufacturer had to do to sell almost any herbal drug or megadose vitamin was to describe it as a “dietary supplement”. The lobbying to get this law through was based on appealing to the Tea Party tendency –get the government’s hands off our vitamins. And it was helped by ‘celebrities’ such as Sissy Spacek and Mel Gibson (it’s impossible to tell whether they really believed in the magic of vitamins, or whether they were paid, or had Tea Party sympathies).
Offit’s discussion of vaccination is a heartbreaking story of venom and misinformation. As co-inventor of the first rotavirus vaccine he’s responsible for saving many lives around the world. But he, perhaps more than anyone, suffered from the autism myth started by the falsified work of Andrew Wakefield.
The scientific community took the question seriously and soon many studies showed absolutely no link between vaccination and autism. But evidence did not seem to interest the alternative world. Rather than Offit being lauded as a saver of children’s lives, he describes how he was subjected to death threats and resorted to having armed guards at meetings.
Again, Offit tells us how celebrities were able to sway public opinion For example (chapter 6), the actress Jenny McCarthy and talk-show hostess Oprah Winfrey promoted, only too successfully, the vaccine-autism link despite abundant evidence that it didn’t exist, and promoted a number of theories that were not supported by any evidence, such as the idea that autism can be “cured” by mega-doses of vitamins and supplements.
Of course vaccines like the one for rotavirus can’t be developed without pharmaceutical companies because, as Offit says, only they "have the resources and expertise to make a vaccine. We can’t make it in our garage". When the Children’s Hospital of Philadelphia sold its royalty stake in the rotavirus vaccine for $182 million, Offit received an undisclosed share of the intellectual property, “in the millions ”.
That’s exactly what universities love. We are encouraged constantly to collaborate with industry, and, in the process, make money for the university. It’s also what Wakefield, and the Royal Free Hospital where he worked, hoped to do. But sadly, these events led to Offit being called names such as “Dr Proffit” and “Biostitute” (to rhyme with “prostitute”) by people like Jenny McCarthy and Robert F. Kennedy Jr. The conspiritorialist public lapped up this abuse, but appeared not to notice that many quacks have become far richer by peddling cures that do not work.
One lesson from this sad story is that we need to think more about the potential for money to lead to good science being disbelieved, and sometimes to corrupt science.
Everyone should buy this book, and weep for the gullibility and corruption that it describes.
I recommend it especially to the deans of US Medical schools, from Harvard downwards, who have embraced “integrative medicine” departments. In doing so they have betrayed both science and their patients.
Abraham Flexner, whose 1910 report first put US medicine on a sound scientific footing, must be turning in his grave.
|

|
Follow-up
30 August 2013
Quack lobby groups got a clause inserted into Obamacare that will make any attempt to evaluate whether a treatment actually works will leave insurance companies open to legal action for "discrimination".
"Discrimination? Yes! We must not allow the government to exclude health care providers just because those providers don’t cure anything."
The latest piece of well-organised corporate corruption by well-funded lobbyists is revealed by Steven Salzberg, in Forbes Magazine. The chaos in the US health system makes one even more grateful for the NHS and for the evaluation of effectiveness of treatments by NICE.
It’s hard to know what to make of David Tredinnick MP (Cons, Bosworth). He is certainly an extreme example of the scientific ignorance of our parliamentary representatives, but he isn’t alone in that. Our present minister of Education, Michael Gove, memorably referred to Newton’s Laws of Thermodynamics, blissfully unaware that thermodynamics was a 19th century development. And our present Minister of Health seems to think that magic water cures diseases.
But Mr Treddinick breaks every record for anti-scientific nonsense. That, no doubt, is why he was upset by the recent revision of come NHS Choices web pages, so that they now give a good account of the evidence (that’s their job, of course). They did that despite two years of obstruction by the Department of Health. which seemed to think that it was appropriate to take advice from Michael Dixon of the Prince’s Foundation for integrated Health. That shocking example of policy based evidence was revealed on this blog, and caused something of a stir.
Treddinick’s latest letter
A copy of a letter from Mr Tredinnick to the Minister of Health, Jeremy Hunt, has some into my possession by a tortuous route [download the letter]. It’s a corker. Here are a few quotations.
"1. UKIP moving onto our ground
Attached is an extract from a recent UKIP policy statement. The position which UKIP has taken is one with which most of our Daily Mail reading supporters of complementary medicine would agree."
It seems that Treddinick’s preferred authority on medicine is now Nigel Farage, leader of the UK’s far right party. UKIP’s policy on health is appended to the letter, and it’s as barmy as most of the other things they say.
"2. Herbal Medicine
. . .there is very real concern that the Government will not regulate Herbal Medicine and Traditional Chinese Medicine. The current situation is unacceptable, because herbal practitioners need regulation and cannot function as herbal therapists, nor can they cannot obtain stocks of their herbal remedies, without it.
This refers to a saga that has been running for at least 10 years. Herbalists are desperate to get a government stamp of approval by getting statutory regulation, much like real doctors have, despite the fact that they make money by selling sick people "an unknown dose of an ill-defined drug, of unknown effectiveness and unknown safety" (as quoted recently in the House of Lords).
Even the US National Center for Complementary and Alternative Medicine (NCCAM) doesn’t claim that a single herbal treatment is useful. The saga of herbal regulation is long and tedious. The short version is that a very bad report, The Pittilo report, recommended regulation of herbalists. After years of prevarication, Andrew Lansley ignored the impartial scientific advice and yielded to the pressure from the herbal industry to accept the Pittilo report. But still nothing has happened.
Could it be that even Jeremy Hunt realises, deep down, that the regulation of nonsense is a nonsense that would harm the public?
We can only hope that a letter from Mr Tredinnick is the kiss of death. Perhaps his continuous pestering will only reinforce the doubts that seem to exist at the Department of Health.
Then Tredinnick returns (yawn) to his obsession with magic water. He vents his rage at the now excellent NHS Choices page on homeopathy.
3. Homeopathy
"Recently this wording has been removed and instead a comment by the Chief Medical Officer that homeopathy is placebo inserted in its place, as well as links to external organisations which campaign against homeopathy. For instance, there is a link to the Sense About Science website, and Caroline Finucane, who is Editor of new content at NHS Choices, also writes for the Sense About Science website. This is an organisation which has no expertise in homeopathy and traces its roots back to the ultra-left Revolutionary Communist Party (RCP)."
"I respectfully suggest that the original wording be reinstated and these links to external organisations be removed or changed to ensure a balanced view.".
So it seems that he prefers the medical views of Nigel Farage and the Prince of Wales to those of the Chief Medical Officer and the government’s chief scientist. Disgracefully, Tredinnick picks out one particular employee of NHS Choices among many, and one who does an excellent job. And he raises the hoary old myth that Sense About Science is a communist organisation. Odd, since others accuse it of being neo-libertarian. The actual history is here. The organisation that is a bit too libertarian for my taste is Spiked Online. I haven’t agreed with every word that Sense about Science has printed, but they have a totally honest belief in evidence.
To drag in the name of one person out of many, and to justify it by a false history shows, once again, how very venomous and vindictive the advocates of delusional medicine can be when they feel cornered.
A bit more information about Mr Treddinick
This is what the BBC News profile says about him.
|
David Tredinnick is an old style Conservative MP, being an Eton-educated former Guards officer, who has sat in the Commons since 1987. However, his ambition for high office was thwarted by his role in one of the sleaze stories which helped to sink the Major government. He accepted £1,000 from an undercover reporter to ask parliamentary questions about a fictitious drug. He was obliged to resign from his role as a PPS and was suspended from the Commons for 20 sitting days. He has not sat on the frontbench since. He is an orthodox Conservative loyalist, though he is more supportive of the European Union than many of his colleagues. He has, however, carved himself a niche as the Commons’ most enthusiastic supporter of complementary medicine. He has wearied successive health secretaries with his persistent advocacy of any and all homeopathic remedies. He has also supported their use in prisons and even suggested them as an aid in alleviating the foot and mouth crisis. |
|
Tredinnick has also asserted that he was aware of a psychiatric hospital that doubled its staff at full moon (this is an old urban myth, and is, of course, quite untrue). His advocacy of homeopathic borax as a way to control the 2001 epidemic of foot and mouth diease can be read here. Luckily it was ignored by the government. I hope his latest letter will be treated similarly. Picture of David Tredinnick MP from the Conservative Party |
 |
Follow-up
The time when I lose patience with quacks is when they make unjustified claims about serious diseases. Giving false hope to the desperate (often at a high price) is plain wicked. If the patient stops more effective treatment, it’s homicide. Homeopaths have been jailed for that. Sometimes it’s a result of wishful thinking. Sometimes it’s to make money. The latter is morally more despicable. Both are culpable.
|
One example was the Totnes (aka Narnia) to “offer real alternatives to the conventional approach to cancer health care“. Another case, the Dove Clinic, was investigated in the Sunday Times, by Jon Ungoed-Thomas and Justin Stoneman: Clinics mislead patients over cancer ‘cure‘. |
|
There is yet another cancer conference, Back2Health, coming up in April (remember that "integrative", in this context, is a euphemism for quackery).

The speakers are listed on the left, as they were when I first noticed the conference in December 2012. On the right are the speakers as of February 2013,
Spot the difference
|
18 December 2012
 |
28 February 2013
 |
Yes, the one respectable oncologist on the programme, Robert Thomas, has withdrawn from the meeting.
I came across Robert Thomas because it was pointed out to me that he spoke at a meeting of YesToLife, an organisation that advocates all sorts of treatments that are unsupported by evidence. That seemed like an odd thing for a respectable oncologist to be doing, so I wrote to him, to point out some of the bizarre beliefs of his fellow speakers. Most are familiar names in made-up medicine, but probably not widely known among real oncologists.
Professor Thomas seemed unaware of this because he told me
"Thank you for your email and pointing out the vitamin C issues which of course, as you say has no scientific basis and should be outlawed along with many other practices."
Nevertheless he thought it was too late to pull out of the YesToLife meeting, so went ahead.
After this Robert Thomas wrote to me again (18 December 2012) to ask for advice about another conference he’d been invited to speak at, the Back2health event. Again he seemed unaware of the reputations of his fellow speakers, just about all of whom have a track record of advocating treatments for which there is no good evidence. Many of them are purveyors of false hope, often at a high price. I’ll deal with only three of them.
Dr Rosy Daniel is there. She’s featured several times on this blog. I met her, with Karol Sikora,here. Her course in quackery was ditched by the University of Buckingham after a year..
Chris Woollams of CancerActive is also there. As readers of this blog will know, I accept he is an honest man and I do feel a great deal of sympathy for him having lost his daughter. This doesn’t mean I am any closer to accepting his views on cancer treatment.
Next to Thomas’s picture is Barbara Wren. She was secretly filmed by the BBC claiming "to have cured thyroid cancer by applying external compresses, half an hour with castor oil and half an hour with your own urine". You can’t get much barmier than that.
Then there is a nurse, Patricia Peat, who runs a private "integrative" cancer consultancy, Cancer Options. She’s a prominent supporter of YesToLife which, since at least February 8th 2013, has been promoting a video, "Cancer is Curable Now", which makes totally irresponsible claims (and is illegal in the UK under the Cancer Act, 1939). Among other baseless treatments she has advocated high dose Vitamin C.
“The first of these people is the proprietor of Cancer Options. Cancer Options is a private consultancy offering advice to cancer patients. It is run by Patricia Peat who is a qualified nurse. My dad went to see her and she told him the good news, if he followed her advice he could be tumour free in 3 to 4 years. She advised him to have intravenous vitamin C, to have oxygen therapy, heat therapy and to take a myriad of supplements.”
I have heard that the cost of these useless recommendations over a three months would have been £4,640, plus the considerable cost of moving to Brighton, to the Vision of Hope hospital. That includes, for example, a telephone consultation (£175), supplement pills (£400) and intravenous vitamin C (£3000). There is no good evidence that any of these would help the patient. Not only would this have destituted his family and taken the patient away from them: it would also have made his last days an unnecessary misery. For Christmas he would have been condemned to a vegan diet, no wheat, sugar or alcohol, and to live on five glasses of raw juice and two jars of sprouts a day (see "Would you kick a dying man" for a real life experience).
Patricia Peat appears prominently on another web site too, Self Help Cancer. There she’s partnered by Dr Chris Etheridge (an ex biochemist, turned herbalist, with no medical qualifications). On that site you’ll find every kind of barminess endorsed. It even takes seriously the notorious Burzynski clinic about which so much has been written, both here and in the USA.
Recommending a bit of foot massage or reiki as a way to relax distraught patients is harmless enough if you like that sort of thing. Recommending you to ignore real doctors is quite another. Patricia Peat is on record as saying (my emphasis).
"Also detoxification is as important as what goes in – the rapid removal of toxins from the body would be massively beneficial in reducing the side effects. If someone is on chemotherapy, its very important to get any herbal preparations checked out by a qualified practitioner, to make sure there are no interactions, with the chemotherapy. A lot of nutritional and herbal supplements are very strong, and it is dangerous to suppose that because they are natural, they can do no harm. Probably the worst person to ask about this is your oncologist "
There is, of course, no reason to think that "detoxification" is anything other than a figment of the imagination. There is no reason to think that (never-named) toxins are important, and no reason to think that the procedures get rid of anything.
If you want sound advice about diet, go to somewhere like the American Cancer Society. There you will find that most of the things that quack nutritionists love to sell you just don’t work. The ACS asks "Will a vitamin a day keep cancer away?". Their answer is
"Can popping vitamin pills prevent cancer? The simple answer is no, based on what we know so far. In fact, some vitamin supplements have even shown harm."
The journalist, John Diamond, described movingly the way that the alternative industry moved in on him when it became known that he had cancer. His book, Snake Oil and Other Preoccupations was never finished before he died. These extracts from the foreword to the book, by Richard Dawkins, sum it up.
"When the pathologist has read the runes; when the oracles of X-ray, CT scan and biopsy have spoken and hope is guttering low; when the surgeon enters the room accompanied by ‘a tallish man … looking embarrassed … in hood and gown with a scythe over his shoulder’, it is then that the ‘alternative’ or ‘complementary’ vultures start circling. This is their moment. This is where they come into their own, for there’s money in hope: the more desperate the hope, the richer the pickings. And. to be fair, many pushers of dishonest remedies are motivated by an honest desire to help. Their persistent importunings of the gravely ill, their intrusively urgent offers of pills and potions, have a sincerity that rises above the financial greed of the quacks they promote. "
"They are targets that deserve to be hit hard, targets whose neutralisation would leave the world a better place: cynical charlatans (or honest foolish dreamers) who prey on gullible unfortunates. And the best part is that although this gallant man is dead, his guns are not silenced"
Shortly before he died, John Diamond said something that I think is one of the most perceptive comments that I’ve ever read. Some of the blame for the rise of the profitable alternative industry lies with the hype of real medicine. It’s worth quoting at length.
|
"But we expected more. Hell, we’d been promised more. Just as we’d learned, rightly, to expect that the political system could be arranged to provide a roof over the head and food in the stomach of all of us, so, we believed, could the medical system be arranged to give us all health and happiness. It was our right, dammit. And the medical establishment, flattered by all those pieces in the popular press describing the latest miracle cure which was just about —always just about — to arrive at the local surgery, joined in with the celebrations and connived with the scam. Indeed, if the boom in alternative medicine is anybody’s fault it’s that of orthodox medicine. It was the orthodoxy -helped by the media and our own vanity – which allowed us to believe that we could all be healthy and happy, that there was a pill for every problem and that if we died too early or too painfully it was an act of some agency other than capricious old God. The orthodoxy allowed us to expect And the elsewhere we looked to was the alternative practitioners. They were only too willing to take our custom . . ." |
I have no way of knowing whether the people at this conference are "cynical charlatans" or "honest foolish dreamers". I impute no motives. But I can say that their treatments are very expensive and for the most part they don’t work.
There is an interesting question about the extent to which charities like YesToLife function as charities, and the extent to which they act as agencies that channel desperate patients into the hands of private hucksters. I don’t pretend to know tha answer. I’d like to.
|
“It is difficult to get a man to understand something, when his salary depends upon his not understanding it.” |
Follow-up
1 April 2013. The Times contacted me shortly after this came out, about some of the (illegal) nonsense to be found on sale at Amazon. One of their journalists, Kat Lay, did a good write-up, and they contacted the MHRA and stirred it into action. [download pdf].
5 April 2013. I quoted some of Patricia Peat’s views on diet from a page on Woollams’ blog. I notice that the copyright conditions on that page changed
![]()
" This content may be copied, in full or in part", has been changed to " No content may be reproduced, in whole or in part".
It’s curious that there should be an attempt to ban the reproduction of content, of which he authors are presumably proud, and which appears on a public web site. Of course it is also baseless in law, because copyright law has always allowed reproduction of parts of any document for the purposes of fair comment or in the public interest.
20 May 2012
In the USA, the first amendment allows the most outrageous claims to be made. But when they do decide the law has been broken, they do something about it. Their law enforcement is not as pathetically impotent as in the UK.
A Dr Christine Donald treated patients with cancer with an expensive herbal concoction, from her Wellness Clinic in San Fernando Valley. She promised 60 – 80% success rate. she was trusted because she was also a Pentecostal minister.
She was convicted of four counts of mail and wire fraud, six counts of tax evasion and one count of witness tampering she was found guilty of in September 2011
She was sentenced to 14 years in jail and a fine of $1.2 million.
One wonders why that never happens in the UK
26 May 2013 I noticed another incredible assertion by Patricia Peat.
“One could be forgiven for thinking how does anyone manage to die from cancer when the answers to curing it are actually so simplistic and one dimensional.”
So that’s solved, then.
10 June 2013.
I have just come across a good source of information about all sorts of alternative cancer treatments. "CAM-Cancer" was originally funded by the European Commission (EC) within the Framework 5 Programme, it is now hosted by the National Information Center for Complementary and Alternative Medicine (NIFAB) at the University of Tromsø, Norway.
|
“In causing NHS Choices to publish content that is less than completely frank about the evidence on homeopathy, the DH have compromised the editorial standards of a website that they themselves established”. . . “. . . they have failed the general public, by putting special interests, politics, and the path of least resistance (as they saw it) before the truth about health and healthcare.” David Mattin, lately of NHS Choices |
NHS Choices is usually a good source of information for the public. But there is one exception: the information they provide about alternative medicine is poor. A Freedom of Information Act request has revealed that the attempt of NHS Choices to rewrite their pages more accurately was censored by the Department of Health in conjunction with the late Prince’s Foundation for Integrated Health. The Department of Health (DH) has misled the public.
The earliest version of the homeopathy information page recorded by the Wayback Machine was November 12 2007. It was still there on December 5 2010. The comments were mostly critical. One said, quite correctly,
|
I find it most regrettable that the way NHS has covered this subject is to give uncritical voice to the claims of homoeopathy without giving readers the information they need to evaluate those claims. To refer readers to the websites of the British Homeopathy Association is like settling the question of the shape of planet by a reference to the website of the Flat Earth Society |
There were a lot of complaints, and to the credit of NHS Choices, the page vanished. Throughout 2011, and up to October 2012 the information page on homeopathy read
|
Introduction Content on homeopathy has been removed from the website pending a review by the Department of Health policy team responsible for complementary and alternative medicines. Homeopathy is not part of mainstream medicine. Instead it is defined as a complementary or alternative medicine. If you are considering using homeopathy, talk to your GP first. For more information about homeopathy see the House of Commons Science and Technology Committee report on homeopathy published on 8 February 2010 and the Department of Health response to that report published in July 2010 (PDF, 69KB). |
Then, at the end of 2012, the page reappeared. It was a bit better than the original, but not much. Many of the comments criticise the misleading nature of the information (as well as the usual “it worked for me” comments). The “useful links” still has six links to flat-earth organisations like the Society of Homeopaths, and only one to a sensible source, the excellent pamphlet from Sense about Science. They do link at the end to the 2010 Science and Technology Committee Report: Evidence Check 2: Homeopathy (PDF, 1.61Mb), and to the Government Response to the Science and Technology Committee Report, Evidence Check 2: Homeopathy (PDF, 69kb) but no comment is made on the findings.
Policy-based evidence
I wondered why the NHS Choices page, after an absence of almost two years, had returned in such an unsatisfactory form. So I asked them. After a reminder, I was told that my queries were being dealt with not by NHS Choices, but had been referred to Dr Sunjai Gupta “the DH official with responsibility for this area”. Dr Sunjai Gupta OBE is Deputy Director of Public Health Strategy and Social Marketing, Department of Health.
Dr Gupta is not obviously sympathetic to woo. It’s hard to tell since he doesn’t seem to have published much. But one is not reassured by an article that he wrote for the Journal of Holistic Healthcare. It appears straight after an article by fantasy herbalist, Simon Mills.
Despite assurances that I’d hear from Dr Gupta shortly, nothing happened. So I sent a request for the correspondence under the Freedom of Information Act (2000). Although the request was addressed to NHS Choices, a public body, strenuous efforts were made to divert it to the Department of Health. These were resisted. Nevertheless when, after a long delay, the material arrived, it came not from NHS Choices, but from DH, who had evidently vetted it,. The emails were rather shocking [download all].
A mail dated 1 December 2009 said

This is the most direct statement I’ve seen that, in the Department of Health, policy dictates evidence. NHS Choices is meant to provide evidence, but what they say has to be checked by DH to make sure they “don’t clash with any policy messages”.
The re-written page
The original version of the re-written page was sent to me by David Mattin, who worked for NHS Choices until September 2012. You can download the whole draft here. It is an enormous improvement on the original page. For example, it says
|
“Does it work?
Many independent experts would respond to this question ‘no, homeopathy does not work’ There is no good quality clinical evidence to show that homeopathy is more successful than placebo in the treatment of any type of condition. Furthermore, if the principles of homeopath were true it would violate all the existing theories of science that we make use of today; not just our theory of medicine, but also chemistry, biology and physics. |
This original draft was sent to Mattin on 29 January 2010. After editing it for length Mattin sent it to DH for approval. Over the next two years, DH removed much of the accurate content. Mattin’s own comments on this evisceration are reproduced below.
The DH emails
All the names have been redacted. Needless to say, nobody is willing to take responsibility. But the number of people who support magic medicine is really quite small so the main players were easy to identify.
During the nearly 2 year absence of the homeopathy page, dozens of changes were made by DH. It seems that the policy message with which the NHS Choices draft failed to comply were those of the Prince’s Foundation for Integrated Health, and its successor (after April 2010), the College of Integrated Health, now known as the College of Medicine.
NHS Choices sought advice about their redrafted pages from the right person, Sir Iain Chalmers, one of the founders of the Cochrane Collaboration. On 3 Nov 2009, Chalmers advised
The most reliable source in the country - and one of the most reliable in the world - is Professor Edzard Ernst, professor of Complementary Medicine at the Peninsular Medical School, |
Ernst returned his suggestions in July 2010, but it seems that few of them survived the subsequent 18 months of revisions by DH.
On 2 December 2009, a mail from the NHS headquarters (Quarry House, Leeds) was sent to NHS Choices
This makes it perfectly clear that DH regards the Prince’s Foundation, and the equally flaky Complementary and Natural Healthcare Council (CNHC: known on the web as Ofquack) as appropriate guides for public health policy. The fact of the matter is that regulation of magic medicine by the government has been a total disaster, because, it seems, DH regards the Prince of Wales as a reliable source.
On 29 December 2009, the Prince’s Foundation went on the attack.
On 10th January 2010, two more letters were sent to DH by the Prince’s Foundation. At 13.48 they wrote
And at 22.14 on the same day, it was followed up with
The references to Devon and to Thought Field Therapy, make it very obvious that these letters were written by Dr Michael Dixon OBE, who was medical director of the Prince’s Foundation, and who is now a director of the “College of Medicine”. And the object of Dixon’s bile is obviously Edzard Ernst (the quotation is from his book, Trick or Treatment).
I find it fascinating to see just how venomous quacks become when the evidence contradicts their views. The cuddly “holistic” veneer quickly vanishes.
It gets worse. On 21 January 2010, a mail from NHS Choices to DH said
The only person in the country who fits this description is the (in)famous George Lewith. It is simply mind-boggling that DH regards him as an appropriate person to advise on anything.
After that, NHS Choices kept asking DH to sign off the documents, and changes continued to be made. Almost two years later, DH were still stalling.
The admission that “We are a bit short of doctors within DH these days” is interesting.
A bit short of anyone capable of critical thinking would be more accurate.
The most interesting document that I got from DH was an intermediate draft of the rewritten page on homeopathy (undated). Download the document. Here are a couple of extracts.
It’s a story of two years of meddling and procrastination. The end result misinforms the public.

Right at the start, the NHS Choices draft says, reasonably enough
A House of Commons Science and Technology Committee report said that homeopathic remedies perform no better than placebos and that the principles on which homeopathv is based are “scientifically implausible”.
But a comment, added apparently by DH, says
Can we remove this statement? This report is really quite contentious and we may well be subject to quite a lot of challenge from the Homeopathic community if published.
What on earth? The DH seems to think that that its job is not to present the evidence, but to avoid challenges from the homeopathic community! And true enough, this piece is missing from the final version.
A bit later, the NHS Choices draft was censored again

“A 2010 Science and Technology Committee report said that scientific tests had shown that homeopathic treatments don’t work”
But again this doesn’t appear in the final version. The comment, apparently from DH, says
“The DH response to this report (point 24) doesn’t support this statement though”
That’s a gross distortion of point 24, which actually concludes
“The Government Chief Scientific Adviser cannot envisage scientifically credible proposals for funding for research into homeopathy in the future”
NHS Choices was not happy with the result
Shortly before the revised page was published, Paul Nuki, Editor in Chief of NHS Choicea, sent an email to DH.
|
Date: 7th September 2011 Time: 3:33:42 pm Hi I’ve been through the CAM articles and asked that we publish them asap as requested. For the record, we will be publishing these pieces outside of the normal editorial process. Although originally signed off by a suitably qualified clinician, the time lapse and policy changes have been so substantial as to render that null and void. We also don’t have a formal |
It doesn’t need much reading between the lines to see that he was unhappy with the result. It will be interesting to see whether the Information Standard people at the Royal Society for Public Health do anything about it.
The Department of Health has not just ignored evidence but actively opposed it.
That’s the only possible conclusion from the documents that I was sent. And it’s pretty shocking that the DH has preferred advice from the Prince’s Foundation and its handful of acolytes (in particular Michael Dixon and George Lewith) to the findings of the Science and Technology Select Committee and the views of the Chief Scientific Advisor.
In January this year, the Chief medical Officer, Dame Sally Davies, said, in a rare outburst of candour
|
‘I’m very concerned when homeopathic practitioners try to peddle this way of life to prevent malaria or other infectious disease,” she said. “I am perpetually surprised that homeopathy is available on the NHS.” Dame Sally, who is England’s most senior doctor, concluded by remarking that homeopathy “is rubbish”. |
 |
So one part of DH is working to contradict another part. the Chief Medical Officer. Perhaps Sally Davies should have a word with Dr Gupta.
This all predates the advent of Jeremy Hunt (and known defender of homeopathy) as health minister. But the sympathies of some DH people are made obvious by the presence on the DH web site of an article “Personal health budgets: A new way of accessing complementary therapies?”. This astonishing piece confirms the worst fears that quacks will see personal health budgets as a commercial opportunity to peddle their wares. The article is by Jim Rogers of Lincoln University. What his paper does not mention is Rogers’ conflict of interest. He’s a homeopath, and he has a paper in the International Journal of High Dilution Research (yes, there is a journal for every form of make-believe). You can download a reprint of this paper. It advocates more research into homeopathic provings, something that even George Lewith seems to have given up on.
It’s about time that the DH started to listen to the Chief Medical Officer. As it is, some people at DH seem to prefer the advice of the Prince’s Foundation, and to actively suppress employees who prefer evidence to anecdote.
One thing is clear. The DH is an unholy mess. Parts of it are intent on producing policy-based evidence.
Comment by David Mattin, who edited the first draft for NHS Choices
David Mattin left NHS Choices in September, 2012. He edited the new version and lived through the two years of wrangling with DH during which much of the best content was eviscerated. He sent me this statement about the affair.
|
As an editor at NHS Choices, I viewed it as my job to present evidence-based information to the public. The article we prepared on homeopathy stayed true to that central purpose: it made clear to readers that there is no good quality evidence that homeopathy is an effective treatment for any health condition, and also presented the broad scientific consensus that the supposed method of action of homeopathy is implausible.
What followed was a two year story of delay, and eventual suppression, of that article. My strong impression was of DH civil servants who lacked the courage, and, frankly, the energy to stand up to the criticism from special interest groups that they anticipated would arise because of the article; and that did indeed arise when a draft of the article and other draft content on complementary and alternative medicines fell into the hands of the Prince’s Foundation and other CAM groups.
The attitude of DH civil servants, broadly, was simply to tell us ‘we can’t say this about homeopathy, people will complain’. They seemed to have no interest in making an appraisal of the evidence on homeopathy themselves to see if what we were saying was actually true or not. We repeatedly pushed back with the message: ‘some people may very well complain, but if what we are saying about the evidence base is true – and it is – then we must simply weather those complaints, and stand by our content. Our duty is to supply our readers with the best information, not to please the homeopathy community.’ But these arguments were disregarded. The DH civil servants were almost entirely concerned with the politics of the situation – that is, the politics as they saw them – and the possibility that this article may create new work for them, and very little concerned with the evidence itself, or the presentation of this evidence to the public.
The whole episode is an insight into the way special interest groups can influence the workings of government and the public sector simply by making a lot of noise, and having a few powerful friends. In causing NHS Choices to publish content that is less than completely frank about the evidence on homeopathy, the DH have compromised the editorial standards of a website that they themselves established, and that they fund. They have sold out the NHS Choices editorial team, who work tirelessly to fulfil their remit. And, most seriously, they have failed the general public, by putting special interests, politics, and the path of least resistance (as they saw it) before the truth about health and healthcare.
|
Follow-up
13 February 2013 The Guardian version of this story, written by Sarah Boseley, is Prince’s charity lobbied government to water down homeopathy criticism. It’s fine as far as it goes but it doesn’t name any names. There are some good comments though.
14 February 2013. The printed Guardian gave the story full 5 column-width coverage. [download print version]

And news has reached the USA: there’s an account of the affair on the Neurologica blog: Politics trumping science at the NHS.
On 14 February, the Guardian version was Editor’s Choice by lunchtime, and the Guardian web version already had 414 comments, mostly sensible (though this blog got far more referrals from twitter than from the Guardian)

And news has reached the USA: there’s an account of the affair on the Neurologica blog: Politics trumping science at the NHS.
15 February 2013. The Daily Mail had very fair coverage of the story.

The Guardian closed the comments on the story when it had got 642 comments, most of them very sensible. And this page got almost 6000 hits in 24 hours. The majority of the referrals came from Twitter rather than from the Guardian, despite the direct link to the page from the Guardian.
18 February 2013. The affair featured in BMJ News [download the reprint]. The item featured prominently on the BMJ news page.
![]()

19 February 2013 Only six days of this post, the NHS Choices page has been re-written again, in a much improved form. That looks like bloggers 1, DH 0. It is baffling that it’s left to bloggers, working for nothing, to extract a bit of sense from the highly-paid civil servants at the Department of Health. But at least they listened this time, which is a lot more than happens often. Paul Nuki, who runs NHS Choices, deserves congratulations. Of course the revised page still doesn’t call a spade a spade, but it gets close at times. I like the way it starts "Homeopathy is a ‘treatment’ based". Notice the quotation marks.
Reputation management?
Incidentally, NHS Choices is outsourced to the (in)famous company, Capita. And the moderation of the comments on their site is outsourced again to Tempero, which describes itself as a "reputation management" company. Each of them creams off money meant of patient care. This discovery might explain why I and others have had comments rejected by NHS Choices several times. "Reputation management" is the antithesis of evidence. It is public relations, i.e. paid lying. That is quite wrong for a site that is meant to provide dispassionate information.
21 February 2013. Sadly a step backwards. Part of the improved page was removed. This bit.
The Chief Medical Officer, Professor Dame Sally Davies, has said there is no scientifically plausible way that homeopathy can prevent or cure diseases. She has made it clear she is particularly concerned about the use of homeopathy in developing countries as a so-called cure for malaria.
We can only speculate why this was removed, because it was true. In fact she accurately described homeopathy as "rubbish". Why she should not be quoted beats me.
Nobody could have been more surprised than I when I found myself nominated as an academic role model at UCL. I had to answer a few questions. It is not obvious to me what the object of the stunt is, but the person who asked me to do it seemed to find the answers amusing, so I’ll reproduce here what I said. I apologise for the temporary lapse into narcissism.
The final version has now been printed [download a copy]. Sadly the printed edition was “corrected” by someone who replaced “whom I asked to submit the first theoretical paper by Hawkes and me to the Royal Society” (as written below), with “paper by Hawkes and I”. Aaargh.
Your nomination – Why you were nominated as an Academic Role Model?
"David Colquhoun has made major contributions to our understanding of how ion channels (proteins which allow charged ions to pass across cell membranes) function to mediate electrical signalling in nerve and muscle cells. This work elegantly combines experimental and theoretical aspects, and resulted in David being made a Fellow of the Royal Society. David Colquhoun played a key role in resisting the notion that UCL should merge with Imperial College in 2002, by running a website opposed to the merger. He thus facilitated the continued existence of an independent UCL. He is also well-known for his principled opposition to therapies that are not based on scientific evidence, and for his blog which comments on this issue as well as on university bureaucracy and politics."
Role models’ questions
1. What is your response to being nominated?
Astounded.
We are interested in giving people a very brief ‘snapshot’ description of their career trajectory, to help a broad range of people see how you got to where you are:
2. What has your career path been?
|
My first job (in 1950s) was as an apprentice pharmacist in Timothy Whites & Taylors (Homeopathic Chemists) in Grange Road, Birkenhead. You can’t get a more humble start than that. But it got me interested in drugs, and thanks to my schoolmaster father, I got to the University of Leeds. |
 My father (1907 – 2001), in 1955 |
|
One of the courses involved some statistics, and that interested me. I think I made a semi-conscious decision that it would be sensible to be good at something that others were bad at, so I learned quite a lot of statistics and mathematics. I recall buying a Methuen’s Monograph on Determinants and Matrices in my final year, and, with the help of an Argentinian PhD student in physical chemistry (not my lecturers) I began to make sense of it. |

|
I purposely went into my final viva with it sticking out of my pocket. The examiner was Walter Perry, then professor of Pharmacology in Edinburgh (he later did a great job setting up the Open University). That’s how I came to be a PhD student in Edinburgh.
Although Perry was one of my supervisors, the only time I saw him was when he came into my lab between committee meetings for a cigarette. But he did make me an honorary lecturer so I could join the Staff Club, where I made many friends, including a young physics lecturer called Peter Higgs. The staff club exists no longer, having been destroyed in one of those acts of short-sighted academic vandalism that vice-chancellors seem so fond of.
The great university expansion in the 1960s made it easy to get a job. The most famous pharmacology department in the world was at UCL so I asked someone to introduce me to its then head, Heinz Schild, and asked him if he had a job. While interned during WW2 he had written a paper on the statistics of biological assay and wanted someone to teach it to students, so I got a job (in 1964), and have been at UCL ever since apart from 9 years. Between 1964 and 1970 I published little, but learned a great deal by writing a textbook on statistics.
That sort of statistics is now thought too difficult for undergraduates, and the famous department that attracted me was itself destroyed in another act of academic vandalism, in 2007.
I have spent my life doing things that I enjoy. Such success as I’ve had, I attribute to a liking for spending time with people cleverer than I am, and wasting time drinking coffee. I found a very clever statistician, Alan Hawkes, in the Housman Room in the late 1960s, and we began to collaborate on the theory of single ion channel analysis in a series of papers that still isn’t quite finished. He did the hard mathematics, but I knew enough about it to write it up in a more or less comprehensible form and to write computer programs to evaluate the algebra. When I got stuck, I would often ask Hyman Kestelman (co-author of the famous mathematics textbook, Massie & Kestelman) to explain, usually in what was then the Joint Staff Common Room at lunch time (it is now the Haldane room, the common room having been confiscated by unenlightened management). Before leaving for the USA in 1970, I, in league with the then professor of French, Brian Woledge, eventually got through a motion that allowed women into the Housman room.
I’d also talk as much as I could to Bernard Katz, whom I asked to submit the first theoretical paper by Hawkes and me to the Royal Society. His comments on the first draft led to the published version making a prediction about single ion channel behaviour before channels could be observed.
The next step was sheer luck. As this was going on, two young Germans, Neher & Sakmann, succeeded in observing the tiny currents that flow through single ion channel molecules, so it became possible to test the theory. In series of visits to Göttingen, Sakmann and I did experiments late into the night. Neher & Sakmann got a well-deserved Nobel Prize in 1991, and I expect I benefitted from a bit of reflected glory
The work that I have done is nothing if not basic. It doesn’t fit in with the current vogue for translational research (most of which will fail), although I would regard it as laying the basis for rational drug design. My only regret is that rational drug design has proved to be so difficult that it won’t be achieved in my lifetime (please don’t believe the hype).
We’d also like you to take a slightly more personal view:
3. What have been the highs (and the lows?) of your career so far?
The highs have been the chance to work with brilliant people and write a handful of papers that have a chance of having a lasting influence. Because I have been able to take my time on those projects there haven’t been too many lows, apart from observing the continuous loss of academic integrity caused by the intense pressure to publish or perish, and the progressive decline in collegiality in universities caused by that pressure combined with the rise in power of managerialism. Luckily the advent of blogs has allowed me to do a little about that.
I’m saddened by the fact that the innumeracy of biologists that I noticed as an undergraduate has not really improved at all (though I don’t believe it is worse). Most biologists still have difficulty with even the simplest equations. Worse still, they don’t know enough maths to communicate their problem to a mathematician, so only too often one sees collaborations with mathematicians produce useless results.
The only real failure I’ve had was when, in a fit of vanity, I applied for the chair of Pharmacology in Oxford, in 1984, and failed to get it. But in retrospect that was really a success too. I would have hated the flummery of Oxford, and as head of department (an increasingly unattractive job) I would have spent my time on pushing paper, not ion channels. In retrospect, it was a lucky escape. UCL is my sort of place (most of the time).
We would like to hear what our role models have to say about the next generation:
4. What advice would you give to people finishing off their PhD?
My career course would be almost impossible now. In fact it is very likely that I would have been fired before I got going in the present climate. There were quite long periods when I didn’t publish much. I was learning the tools of my trade, both mathematical and experimental. Now there is no time to do that. You are under pressure to publish a paper a week (for the glory of your PI and your university) and probably rarely find time to leave the lab to talk to inspiring people. If you are given any courses they’ll probably be in some inane HR nonsense, not in algebra. That is one reason we started our summer workshop, though bizarrely that has now been dropped by the graduate school in favour of Advanced Powerpoint.
The plight of recent PhDs is dire. Too many are taken on (for the benefit of the university, not of the student) and there aren’t many academic jobs. If you want to stay in academia, all I can suggest is that you get good at doing something that other people can’t do, and to resist the pressure to publish dozens of trivial papers.
Try to maintain some academic integrity despite the many pressures to do the opposite that are imposed on you by your elders (but not always betters). That may or may not be enough to get you the job that you want, but at least you’ll be able to hold your head high.
Finally, we want to give a balanced impression of our role models because many were nominated for their ability to motivate others, and to balance life and work:
5. How do you keep motivated?
Work-life balance is much talked about by HR, though they are one of the reasons why it is now almost impossible, In the past it wasn’t a great problem. I’m fascinated by the problems that I’m trying to puzzle out. I’ve had periods of a year or two when things haven’t gone well and I’ve felt as though I was a failure, but luckily they haven’t lasted too long, and they occurred in a time before some idiotic performance manager would harass you for failing to publish for a year or two. The climate of “performance management” is doing a lot to kill innovation and creativity.
6. What do you do when are not working in SLMS?
I’ve had various phases. For a while I carried on boxing (which had been compulsory at school). When I was first at UCL in 1964 I bought a 21 foot sloop (and as a consequence could barely afford to eat), and in 1970 (at Yale) I learned to fly. I had a lot of fun sailing right up to the early 1980s, when I found I could not afford a son as well as a boat. That was when running came into fashion and that could be done for the price of a pair of shoes. I did marathons and half marathons for fun (the London in 1988 was great fun). And that was supplanted by walking country trails in the early 2000s.
There is never a clear division between work and play, especially with algebra. You can continue to struggle with a derivation on a boat, or even get a new angle on it while running. That, of course, is why the transparency review is such total nonsense.
The main cause of stress has never been work for me. Stress comes mainly from the imposition of dim-witted managerialism and incompetent HR policies. And that has become progressively worse. I doubt that if I were a young academic now I’d have the time to spend the weekend sailing.
I’m not sure whether the blogging that has taken up something like half my time since my nominal retirement in 2004 counts as work or not. It certainly depends on things that I have learned in my academic work. And it’s fun to have effects in the real world after a life spent on problems that many would regard as esoteric.
If you want a hobby that costs very little, and allows you to say what you want, start a blog.
Follow-up
The Scottish Universities Medical Journal asked me to write about the regulation of alternative medicine. It’s an interesting topic and not easy to follow because of the veritable maze of more than twenty overlapping regulators and quangos which fail utterly to protect the public against health fraud. In fact they mostly promote health fraud. The paper is now published, and here is a version with embedded links (and some small updates).
We are witnessing an increasing commercialisation of medicine. It’s really taken off since the passage of the Health and Social Security Bill into law. Not only does that mean having NHS hospitals run by private companies, but it means that “any qualified provider” can bid for just about any service. The problem lies, of course, in what you consider “qualified” to mean. Any qualified homeopath or herbalist will, no doubt, be eligible. University College London Hospital advertised for a spiritual healer. The "person specification" specified a "quallfication", but only HR people think that a paper qualification means that spiritual healing is anything but a delusion.
The vocabulary of bait and switch
First, a bit of vocabulary. Alternative medicine is a term that is used for medical treatments that don’t work (or at least haven’t been shown to work). If they worked, they’d be called “medicine”. The anti-malarial, artemesinin, came originally from a Chinese herb, but once it had been purified and properly tested, it was no longer alternative. But the word alternative is not favoured by quacks. They prefer their nostrums to be described as “complementary” –it sounds more respectable. So CAM (complementary and alternative medicine became the politically-correct euphemism. Now it has gone a stage further, and the euphemism in vogue with quacks at the moment is “integrated” or “integrative” medicine. That means, very often, integrating things that don’t work with things that do. But it sounds fashionable. In reality it is designed to confuse politicians who ask for, say, integrated services for old people.
Put another way, the salespeople of quackery have become rather good at bait and switch. The wikepedia definition is as good as any.
Bait-and-switch is a form of fraud, most commonly used in retail sales but also applicable to other contexts. First, customers are “baited” by advertising for a product or service at a low price; second, the customers discover that the advertised good is not available and are “switched” to a costlier product.
As applied to the alternative medicine industry, the bait is usually in the form of some nice touchy-feely stuff which barely mentions the mystical nonsense. But when you’ve bought into it you get the whole panoply of nonsense. Steven Novella has written eloquently about the use of bait and switch in the USA to sell chiropractic, acupuncture, homeopathy and herbal medicine: "The bait is that CAM offers legitimate alternatives, the switch is that it primarily promotes treatments that don’t work or are at best untested and highly implausible.".
The "College of Medicine" provides a near-perfect example of bait and switch. It is the direct successor of the Prince of Wales’ Foundation for Integrated Health. The Prince’s Foundation was a consistent purveyor of dangerous medical myths. When it collapsed in 2010 because of a financial scandal, a company was formed called "The College for Integrated Health". A slide show, not meant for public consumption, said "The College represents a new strategy to take forward the vision of HRH Prince Charles". But it seems that too many people have now tumbled to the idea that "integrated", in this context, means barmpottery. Within less than a month, the new institution was renamed "The College of Medicine". That might be a deceptive name, but it’s a much better bait. That’s why I described the College as a fraud and delusion.
Not only did the directors, all of them quacks, devise a respectable sounding name, but they also succeeded in recruiting some respectable-sounding people to act as figureheads for the new organisation. The president of the College is Professor Sir Graham Catto, emeritus professor of medicine at the University of Aberdeen. Names like his make the bait sound even more plausible. He claims not to believe that homeopathy works, but seems quite happy to have a homeopathic pharmacist, Christine Glover, on the governing council of his college. At least half of the governing Council can safely be classified as quacks.
So the bait is clear. What about the switch? The first thing to notice is that the whole outfit is skewed towards private medicine: see The College of Medicine is in the pocket of Crapita Capita. The founder, and presumably the main provider of funds (they won’t say how much) is the huge outsourcing company, Capita. This is company known in Private Eye as Crapita. Their inefficiency is legendary. They are the folks who messed up the NHS computer system and the courts computer system. After swallowing large amounts of taxpayers’ money, they failed to deliver anything that worked. Their latest failure is the court translation service.. The president (Catto), the vice president (Harry Brunjes) and the CEO (Mark Ratnarajah) are all employees of Capita.
The second thing to notice is that their conferences and courses are a bizarre mixture of real medicine and pure quackery. Their 2012 conference had some very good speakers, but then it had a "herbal workshop" with Simon Mills (see a video) and David Peters (the man who tolerates dowsing as a way to diagnose which herb to give you). The other speaker was Dick Middleton, who represents the huge herbal company, Schwabe (I debated with him on BBC Breakfast), In fact the College’s Faculty of Self-care appears to resemble a marketing device for Schwabe.
Why regulation isn’t working, and can’t work
There are various levels of regulation. The "highest" level is the statutory regulation of osteopathy and chiropractic. The General Chiropractic Council (GCC) has exactly the same legal status as the General Medical Council (GMC). This ludicrous state of affairs arose because nobody in John Major’s government had enough scientific knowledge to realise that chiropractic, and some parts of osteopathy, are pure quackery,
The problem is that organisations like the GCC function more to promote chiropractic than to regulate them. This became very obvious when the British Chiropractic Association (BCA) decided to sue Simon Singh for defamation, after he described some of their treatments as “bogus”, “without a jot of evidence”.
In order to support Singh, several bloggers assessed the "plethora of evidence" which the BCA said could be used to justify their claims. When, 15 months later, the BCA produced its "plethora" it was shown within 24 hours that the evidence was pathetic. The demolition was summarised by lawyer, David Allen Green, in The BCA’s Worst Day.
In the wake of this, over 600 complaints were made to the GCC about unjustified claims made by chiropractors, thanks in large part to heroic work by two people, Simon Perry and Allan Henness. Simon Perry’s Fishbarrel (browser plugin) allows complaints to be made quickly and easily -try it). The majority of these complaints were rejected by the GCC, apparently on the grounds that chiropractors could not be blamed because the false claims had been endorsed by the GCC itself.
My own complaint was based on phone calls to two chiropractors, I was told such nonsense as "colic is down to, er um, faulty movement patterns in the spine". But my complaint never reached the Conduct and Competence committee because it had been judged by a preliminary investigating committee that there was no case to answer. The impression one got from this (very costly) exercise was that the GCC was there to protect chiropractors, not to protect the public.
The outcome was a disaster for chiropractors, wno emerged totally discredited. It was also a disaster for the GCC which was forced to admit that it hadn’t properly advised chiropractors about what they could and couldn’t claim. The recantation culminated in the GCC declaring, in August 2010, that the mythical "subluxation" is a "historical concept " "It is not supported by any clinical research evidence that would allow claims to be made that it is the cause of disease.". Subluxation was a product of the fevered imagination of the founder of the chiropractic cult, D.D. Palmer. It referred to an imaginary spinal lesion that he claimed to be the cause of most diseases. .Since ‘subluxation’ is the only thing that’s distinguished chiropractic from any other sort of manipulation, the admission by the GCC that it does not exist, after a century of pretending that it does, is quite an admission.
The President of the BCA himself admitted in November 2011
“The BCA sued Simon Singh personally for libel. In doing so, the BCA began one of the darkest periods in its history; one that was ultimately to cost it financially,”
As a result of all this, the deficiencies of chiropractic, and the deficiencies of its regulator were revealed, and advertisements for chiropractic are somewhat less misleading. But this change for the better was brought about entirely by the unpaid efforts of bloggers and a few journalists, and not at all by the official regulator, the GCC. which was part of the problem. not the solution. And it was certainly not helped by the organisation that is meant to regulate the GCC, the Council for Health Regulatory Excellence (CHRE) which did nothing whatsoever to stop the farce.
At the other end of the regulatory spectrum, voluntary self-regulation, is an even worse farce than the GCC. They all have grand sounding "Codes of Practice" which, in practice, the ignore totally.
The Society of Homeopaths is just a joke. When homeopaths were caught out recommending sugar pills for prevention of malaria, they did nothing (arguably such homicidal advice deserves a jail sentence).
The Complementary and Natural Healthcare Council (CNHC) is widely know in the blogosphere as Ofquack. I know about them from the inside, having been a member of their Conduct and Competence Committee, It was set up with the help of a £900,000 grant from the Department of Health to the Prince of Wales, to oversee voluntary self-regulation. It fails utterly to do anything useful.. The CNHC code of practice, paragraph 15 , states
“Any advertising you undertake in relation to your professional activities must be accurate. Advertisements must not be misleading, false, unfair or exaggerated”.
When Simon Perry made a complaint to the CNHC about claims being made by a CNHC-registered reflexologist, the Investigating Committee upheld all 15 complaints. But it then went on to say that there was no case to answer because the unjustified claims were what the person had been taught, and were made in good faith.
This is precisely the ludicrous situation which will occur again and again if reflexologists (and many other alternative therapies) are “accredited”. The CNHC said, correctly, that the reflexologist had been taught things that were not true, but then did nothing whatsoever about it apart from toning down the advertisements a bit. They still register reflexologists who make outrageously false claims.
Once again we see that no sensible regulation is possible for subjects that are pure make-believe.
The first two examples deal (or rather, fail to deal) with regulation of outright quackery. But there are dozens of other quangos that sound a lot more respectable.
European Food Standards Agency (EFSA). One of the common scams is to have have your favourite quack treatment classified as a food not as a medicine. The laws about what you can claim have been a lot laxer for foods. But the EFSA has done a pretty good job in stopping unjustified claims for health benefits from foods. Dozens of claims made by makers of probiotics have been banned. The food industry, needless to say, objects very strongly to be being forced to tell the truth. In my view, the ESFA has not gone far enough. They recently issued a directive about claims that could legally be made. Some of these betray the previously high standards of the EFSA. For example you are allowed to say that "Vitamin C contributes to the reduction of tiredness and fatigue" (as long as the product contains above a specified amount of Vitamin C. I’m not aware of any trials that show vitamin C has the slightest effect on tiredness or fatigue, Although these laws do not come into effect until December 2012, they have already been invoked by the ASA has a reason not to uphold a complaint about a multivitamin pill which claimed that it “Includes 8 nutrients that can contribute to the reduction in tiredness and fatigue”
The Advertising Standards Authority (ASA). This is almost the only organisation that has done a good job on false health claims. Their Guidance on Health Therapies & Evidence says
"Whether you use the words ‘treatment’, ‘treat’ or ‘cure’, all are likely to be seen by members of the public as claims to alleviate effectively a condition or symptom. We would advise that they are not used"
"Before and after’ studies with little or no control, studies without human subjects, self-assessment studies and anecdotal evidence are unlikely to be considered acceptable"
"Before and after’ studies with little or no control, studies without human subjects, self-assessment studies and anecdotal evidence are unlikely to be considered acceptable"
They are spot on.
The ASA’s Guidance for Advertisers of Homeopathic Services is wonderful.
"In the simplest terms, you should avoid using efficacy claims, whether implied or direct,"
"To date, the ASA has have not seen persuasive evidence to support claims that homeopathy can treat, cure or relieve specific conditions or symptoms."
That seems to condemn the (mis)labelling allowed by the MHRA as breaking the rules.. Sadly, though, the ASA has no powers to enforce its decisions and only too often they are ignored. The Nightingale collaboration has produced an excellent letter that you can hand to any pharmacist who breaks the rules
The ASA has also judged against claims made by "Craniosacral therapists" (that’s the lunatic fringe of osteopathy). They will presumably uphold complaints about similar claims made (I’m ashamed to say) by UCLH Hospitals.
The private examination company Edexcel sets exams in antiscientific subjects, so miseducating children. The teaching of quackery to 16 year-olds has been approved by a maze of quangos, none of which will take responsibility, or justify their actions. So far I’ve located no fewer than eight of them. The Office of the Qualifications and Examinations Regulator (OfQual), Edexcel, the Qualifications and Curriculum Authority (QCA), Skills for Health, Skills for Care, National Occupational Standards (NOS), private exam company VTCT and the schools inspectorate, Ofsted.. Asking any of these people why they approve of examinations in imaginary subjects meets with blank incomprehension. They fail totally to protect tha public from utter nonsense.
The Department of Education has failed to do anything about the miseducation of children in quackery. In fact it has encouraged it by, for the first time, giving taxpayers’ money to a Steiner (Waldorf) school (at Frome, in Somerset). Steiner schools are run by a secretive and cult-like body of people (read about it). They teach about reincarnation, karma, gnomes, and all manner of nonsense, sometimes with unpleasant racial overtones. The teachers are trained in Steiner’s Anthroposophy, so if your child gets ill at school they’ll probably get homeopathic sugar pills. They might well get measles or mumps too, since Steiner people don’t believe in vaccination.
Incredibly, the University of Aberdeen came perilously close to appointing a chair in anthroposophical medicine. This disaster was aborted by bloggers, and a last minute intervention from journalists. Neither the university’s regulatory mechanisms. nor any others, seemed to realise that a chair in mystical barmpottery was a bad idea.
Trading Standards offices and the Office of Fair Trading.
It is the statutory duty of Trading Standards to enforce the Consumer Protection Regulations (2008) This European legislation is pretty good. it caused a lawyer to write " Has The UK Quietly Outlawed “Alternative” Medicine?". Unfortunately Trading Standards people have consistently refused to enforce these laws. The whole organisation is a mess. Its local office arrangement fails totally to deal with the age of the internet. The situation is so bad that a group of us decided to put them to the test. The results were published in the Medico-Legal Journal, Rose et al., 2012. "Spurious Claims for Health-care Products: An Experimental Approach to Evaluating Current UK Legislation and its Implementation". They concluded "EU directive 2005/29/EC is
largely ineffective in preventing misleading health claims for consumer products in
the UK"
Skills for Health is an enormous quango which produces HR style "competences" for everything under the son. They are mostly quite useless. But those concerned with alternative medicine are not just useless. They are positively harmful. Totally barmy. There are competences and National Occupational Standards for every lunatic made-up therapy under the sun. When I phoned them to discover who’d written them, I learned that the had been drafted by the Prince of Wales’ Foundation for Magic Medicine. And when I joked by asking if they had a competence for talking to trees, I was told, perfectly seriously, “You’d have to talk to LANTRA, the land-based organisation for that.”
That was in January 2008. A lot of correspondence with the head of Skills for Health got nowhere at all. She understood nothing and it hasn’t improved a jot.
This organisation costs a lot of taxpayers’ money and it should have been consigned to the "bonfire of the quangos" (but of course there was no such bonfire in reality). It is a disgrace.
The Quality Assurance Agency (QAA) is supposed to ensure the quality of university courses. In fact it endorses courses in nonsense alternative medicine and so does more harm than good. The worst recent failure of the QAA was in the case of the University of Wales: see Scandal of the University of Wales and the Quality Assurance Agency. The university was making money by validating thousands of external degrees in everything from fundamentalist theology to Chinese Medicine. These validations were revealed as utterly incompetent by bloggers, and later by BBC Wales journalist Ciaran Jenkins (now working for Channel 4).
The mainstream media eventually caught up with bloggers. In 2010, BBC1 TV (Wales) produced an excellent TV programme that exposed the enormous degree validation scam run by the University of Wales. The programme can be seen on YouTube (Part 1, and Part 2). The programme also exposed, incidentally, the uselessness of the Quality Assurance Agency (QAA) which did nothing until the scam was exposed by TV and blogs. Eventually the QAA sent nine people to Malaysia to investigate a dodgy college that had been revealed by the BBC. The trip cost £91,000. It could have been done for nothing if anyone at the QAA knew how to use Google.
The outcome was that the University of Wales stopped endorsing external courses, and it was soon shut down altogether (though bafflingly, its vice-chancellor, Marc Clement was promoted). The credit for this lies entirely with bloggers and the BBC. The QAA did nothing to help until the very last moment.
Throughout this saga Universities UK (UUK), has maintained its usual total passivity. They have done nothing whatsoever about their members who give BSc degrees in anti-scientific subjects. (UUK used to known as the Committee of Vice-Chancellors and Principals).
Council for Health Regulatory Excellence (CHRE), soon to become the PSAHSC,
Back now to the CHRE, the people who failed so signally to sort out the GCC. They are being reorganised. Their consultation document says
"The Health and Social Care Act 20122 confers a new function on the Professional Standards Authority for Health and Social Care (the renamed Council for Healthcare Regulatory Excellence). From November 2012 we will set standards for organisations that hold voluntary registers for people working in health and social care occupations and we will accredit the register if they meet those standards. It will then be known as an ‘Accredited Register’. "
They are trying to decide what the criteria should be for "accreditation" of a regulatory body. The list of those interested has some perfectly respectable organisations, like the British Psychological Society. It also contains a large number of crackpot organisations, like Crystal and Healing International, as well as joke regulators like the CNHC.
They already oversee the Health Professions Council (HPC) which is due to take over Herbal medicine and Traditional Chinese Medicine, with predictably disastrous consequences.
Two of the proposed criteria for "accreditation" appear to be directly contradictory.
Para 2.5 makes the whole accreditation pointless from the point of view of patients
2.5 It will not be an endorsement of the therapeutic validity or effectiveness of any particular discipline or treatment.
Since the only thing that matters to the patient is whether the therapy works (and is safe), accrediting of organisations that ignore this will merely give the appearance of official approval of crystal healing etc etc. This appears to contradict directly
A.7 The organisation can demonstrate that there either is a sound knowledge base underpinning the profession or it is developing one and makes that explicit to the public.
A "sound knowledge base", if it is to mean anything useful at all, means knowledge that the treatment is effective. If it doesn’t mean that, what does it mean?
It seems that the official mind has still not grasped the obvious fact that there can be no sensible regulation of subjects that are untrue nonsense. If it is nonsense, the only form of regulation that makes any sense is the law.
Please fill in the consultation. My completed return can be downloaded as an example, if you wish.
Medicines and Healthcare products Regulatory Agency (MHRA) should be a top level defender of truth. Its strapline is
"We enhance and safeguard the health of the public by ensuring that medicines and medical devices work and are acceptably safe."
The MHRA did something (they won’t tell me exactly what) about one of the most cruel scams that I’ve ever encountered, Esperanza Homeopathic Neuropeptide, peddled for multiple sclerosis, at an outrageous price ( £6,759 for 12 month’s supply). Needless to say there was not a jot of evidence that it worked (and it wasn’t actually homeopathic).
Astoundingly, Trading Standards officers refused to do anything about it.
The MHRA admit (when pushed really hard) that there is precious little evidence that any of the herbs work, and that homeopathy is nothing more than sugar pills. Their answer to that is to forget that bit about "ensuring that medicines … work"
Here’s the MHRA’s Traditional Herbal Registration Certificate for devils claw tablets.

The wording "based on traditional use only" has to be included because of European legislation. Shockingly, the MHRA have allowed them to relegate that to small print, with all the emphasis on the alleged indications. The pro-CAM agency NCCAM rates devil’s claw as "possibly effective" or "insufficient evidence" for all these indications, but that doesn’t matter because the MHRA requires no evidence whatsoever that the tablets do anything. They should, of course, added a statement to this effect to the label. They have failed in their duty to protect and inform the public by allowing this labelling.
But it gets worse. Here is the MHRA’s homeopathic marketing authorisation for the homeopathic medicinal product Arnicare Arnica 30c pillules
It is nothing short of surreal.
|
|
Since the pills contain nothing at all, they don’t have the slightest effect on sprains, muscular aches or bruising. The wording on the label is exceedingly misleading.
If you "pregnant or breastfeeding" there is no need to waste you doctor’s time before swallowing a few sugar pills.
"Do not take a double dose to make up for a missed one". Since the pills contain nothing, it doesn’t matter a damn.
"If you overdose . . " it won’t have the slightest effect because there is nothing in them
And it gets worse. The MHRA-approved label specifies ACTIVE INGREDIENT. Each pillule contains 30c Arnica Montana
No, they contain no arnica whatsoever.
|
|
It truly boggles the mind that men with dark suits and lots of letters after their names have sat for hours only to produce dishonest and misleading labels like these.
When this mislabeling was first allowed, it was condemned by just about every scientific society, but the MHRA did nothing.
The Nightingale Collaboration.
This is an excellent organisation, set up by two very smart skeptics, Alan Henness and Maria MacLachlan. Visit their site regularly, sign up for their newsletter Help with their campaigns. Make a difference.
Conclusions
The regulation of alternative medicine in the UK is a farce. It is utterly ineffective in preventing deception of patients.
Such improvements as have occurred have resulted from the activity of bloggers, and sometime the mainstream media. All the official regulators have, to varying extents, made things worse.
The CHRE proposals promise to make matters still worse by offering "accreditation" to organisations that promote nonsensical quackery. None of the official regulators seem to be able to grasp the obvious fact that is impossible to have any sensible regulation of people who promote nonsensical untruths. One gets the impression that politicians are more concerned to protect the homeopathic (etc, etc) industry than they are to protect patients.
Deception by advocates of alternative medicine harms patients. There are adequate laws that make such deception illegal, but they are not being enforced. The CHRE and its successor should restrict themselves to real medicine. The money that they spend on pseudo-regulation of quacks should be transferred to the MHRA or a reformed Trading Standards organisation so they can afford to investigate and prosecute breaches of the law. That is the only form of regulation that makes sense.
Follow-up
The shocking case of the continuing sale of “homeopathic vaccines” for meningitis, rubella, pertussis etc was highlighted in an excellent TV programme by BBC South West. The failure of the MHRA and the GPC do take any effective action is a yet another illustration of the failure of regulators to do their job. I have to agree with Andy Lewis when he concludes
“Children will die. And the fault must lie with Professor Sir Kent Woods, chairman of the regulator.”
Although many university courses in quackery have now closed, two subjects that hang on in a few places are western herbalism, and traditional Chinese medicine (including acupuncture). The University of Westminster still runs Chinese medicine, and Western herbal medicine (with dowsing). So do the University of Middlesex and University of East London.
Since the passing of the Health and Social Security Act, these people have been busy with their customary bait and switch tactics, trying to get taxpayers’ money. It’s worth looking again at the nonsense these people talk.
Take for example, the well known herbalist, Simon Mills. At one time he was associated with the University of Exeter, but no longer. Perhaps his views are too weird even for their Third Gap section (the folks who so misrepresented their results in a trial of acupuncture). Unsurprisingly, he was involved in the late Prince’s Foundation for Magic Medicine, and, unsurprisingly, he is involved with its successor, the "College of Medicine", where he spoke along similar lines. You can get a good idea about his views from the video of a talk that he gave at Schumacher College in 2005. It’s rather long, and exceedingly uncritical, so here’s a shorter version to which some helpful captions have been added.
That talk is weird by any standards. He says, apparently with a straight face, that "all modern medicines are cold in the third degree"..And with ginger and cinnamon "You can stop a cold, generally speaking, in its tracks" (at 21′ 30" in the video). This is simply not true, but he says it, despite the fact that the Plant Medicine with site (of which he’s a director) which he is associated gives them low ratings
Simon Mills is also a director of SustainCare. Their web site says
SustainCare Community Interest Company is a social enterprise set up to return health care to its owners: “learning to look after ourselves and our families in ways that make sense and do not cost the earth“. It is founded on the principle that one’s health is a personal story, and that illness is best managed when we make our health care our own. The enterprise brings clinical expertise, long experience of academia, education and business, and the connections and resources to deliver new approaches.
"As its own social enterprise contribution to this project Sustaincare set up and supported Café Sustain as a demonstration Intelligent Waiting Room at Culm Valley Integrated Centre for Health in Devon". (yes, that’s Michael Dixon, again]
In the talk (see video) Mills appears to want to take medicine back to how it was 1900 years ago, in the time of Galen. The oblique speaking style is fascinating. He never quite admits that he thinks all that nonsense is true, but presumably it is how he treats patients. Yet a person with these bizarre pre-scientific ideas is thought appropriate to advise the MHRA
It’s characteristic of herbalists that they have a very long list of conditions for which each herb is said to be good. The sort of things said by Mills differ little from the 1900-year old ideas of Galen, io the 17th century ideas of Culpepper.
You can see some of the latter in my oldest book, Blagrave’s supplement to Culpepper’s famous herbal, published in 1674.

See what he has to say about daffodils
It is "under the dominion of Mars, and the roots hereof are hot and dry almost in the third degree".
"The root, boyled in posset drink, and drunk, causeth vomiting, and is used with good successe in the beginning of Agues, especiallyTertians, which frequently rage in the spring-time: a plaister made of the roots with parched Barley meal, and applied to swellings and imposthumes do dissolve them; the juice mingled with hony, frankincense, wine and myrrhe, and dropped into the Eares, is good against the corrupt filth and running matter of the Eares; the roots made hollow and boyled in oyl doth help Kib’d heels [or here]: the juice of the root is good for Morphew, and discolourings of the skin."
It seems that daffodils would do a lot in 1674. Even herbalists don’t seem to use it much now. A recent herbal site describes daffodil as "poisonous".
But the descriptions are very like those used by present day herbalists, as you can hear in Simon Mills’ talk.
Chinese medicine is even less tested than western herbs. Not a single Chinese herb has been shown to be useful for treating anything (though in a very few case, they have been found to contain drugs that are useful when purified, notably the anti-malarial compound, artemesinin). They are often contaminated, some are dangerously toxic. And they contribute to the extinction of tigers and rhinoceros because of the silly myths that these make useful medicines. The cruelty of bear bile farming is legendary.
In a recent report in China Daily (my emphasis).
In a congratulation letter, Vice-Premier Li Keqiang called for integration of TCM and Western medicine.
TCM, as a time-honored treasure of Chinese civilization, has contributed to the prosperity of China and brought impacts to world civilization, Li said.
He also urged medical workers to combine the merits of TCM with contemporary medicine to better facilitate the ongoing healthcare reform in China.
The trade in Chinese medicines survives only for two reasons. One is that thay are a useful tool for promoting Chinese nationalism. The other is that they are big business. Both are evident in the vice-premier’s statement.
I presume that it’s the business bit that is the reason why London South Bank University (ranked 114 ou ot 114) that led to one of their main lecture theatres being decorated with pictures like this.“Mr Li Changchun awarding 2010 Confucius Institute of the year to LSBU Vice Chancellor” . I’ll bet Mr Li Changchun uses real medicine himself, as most Chinese who can afford it do.

Presumably, what’s taught in their Confucius Institute is the same sort of dangerous make-believe nonsense.that’s taught on other such courses.
The "College of Medicine" run a classical bait and switch operation. Their "First Thursday lectures" have several good respectable speakers, but then they have Andrew Flower, He is "a former president of the Register of Chinese Herbal Medicine, a medical herbalist and acupuncturist. He has recently completed a PhD exploring the role of Chinese herbal medicine in the treatment of endometriosis". He’s associated with the Avicenna Centre for Chinese Medicine, and with the University of Southampton’s quack division The only bit of research I could find by Andrew Flower was a Cochrane review, Chinese herbal medicine for endometriosis. The main results tell us
"Two Chinese RCTs involving 158 women were included in this review. Both these trials described adequate methodology. Neither trial compared CHM with placebo treatment."
But the plain language summary says
"This review suggests that Chinese herbal medicine (CHM) may be useful in relieving endometriosis-related pain with fewer side effects than experienced with conventional treatment."
It sounds to me as though people as partisan as the authors of this should not be allowed to write Cochrane reviews.
Flower’s talk is followed by one from the notorious representative of the herbal industry, Michael McIntyre, talking on Herbal medicine: A major resource for the 21st century. That’s likely to be about as objective as if they’d invited a GSK drug rep to talk about SSRIs.
The people at Kings College London Institute of Pharmaceutical Sciences are most certainly not quacks. They have made a database of chemicals found in traditional Chinese medicine. It’s sold by a US company, Chem-TCM and it’s very expensive (Commercial license: $3,740.00. Academic/government license: $1,850.00). Not much open access there. It’s a good idea to look at chemicals of plant origin, but only as long as you don’t get sucked into the myths. It’s only too easy to fall for the bait and switch of quacks (like TCM salespeople). The sample page shows good chemical and botanical information, and predicted (not observed) pharmacological activity. More bizarrely, it shows also analysis of the actions claimed by TCM people.
![]()
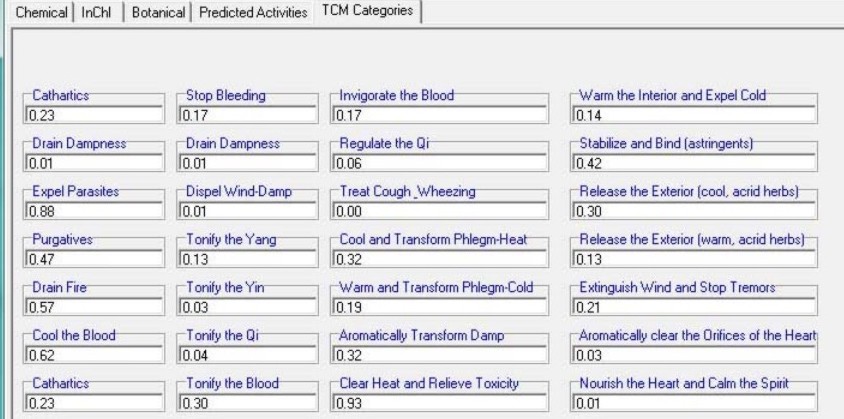
It does seem odd to me to apply sophisticated classification methods to things that are mostly myth.
The multiple uses claimed for Chinese medicines are very like the make-believe claims made for western herbs by Galen, Culpepper and (with much less excuse) by Mills.
They are almost all untrue, but their proponents are good salesmen. Don’t let them get a foot in your door.
Follow-up
10 June 2012. No sooner did this post go public when I can across what must be one of the worst herbal scams ever: “Arthroplex“
31 July 2012. Coffee is the subject of another entry in the 1674 edition of Blagrave.
Blagrave evidently had a lower regard for coffee than I have.
“But being pounded and baked, as do it to make the Coffee-liquor with, it then stinks most loathsomly, which is an argument of some Saturnine quality in it.”
“But there is no mention of an medicinal use thereof, by any Author either Antient of Modern”
Blagrave says also
“But this I may truly say of it [coffee]: Quod Anglorum Corpora quae huic liquori, tantopere indulgent, in Barbarorum naturam degenerasse videntur,”
This was translated expertly by Benet Salway, of UCL’s History department
“that the bodies of the English that indulge in this liquor to such an extent seem to degenerate into the nature of barbarians”
My boss, Lucia Sivolotti got something very like that herself. Be very impressed.
Salway suggested that clearer Latin would have been “quod corpora Anglorum, qui tantopere indulgent huic liquori, degenerasse in naturam barbarorum videntur”.
I’d have passed that on to Blagrave, but I can’t find his email address.
I much prefer Alfréd Rényi’s aphorism (often misattributed to Paul Erdös)
“A mathematician is a machine for turning coffee into theorems”
Much has been written on this blog about Dr Michael Dixon, and about the "College of Medicine", which is the direct inheritor of the mantle of the late, unlamented, Prince’s Foundation for Integrated Health. At the time of the foundation of the College it was stated that "The College represents a new strategy to take forward the vision of HRH Prince Charles".
Michael Dixon has also been chairman of the NHS Alliance since 1998. That was one of very few organisations to support Andrew Lansley’s Health Bill. No doubt he will be happy for Crapita Capita to supply alternative nonsense at public expense.
Dr Dixon took offence to a review in The Times of Mark Henderson’s new book, The Geek Manifesto.
 .
.
The review, by David Aaronovitch, said, apropos of the 1023 campaign,
" . . .there was now, almost for the first time, a group of people who were not content to see claims made for discredited treatments without making everyone aware of the science that disproved those claims. And second, what they were doing had implications for public policy."
and
"The geeks represent, for me, one of the most encouraging recent developments in British public life."
This excellent review evidently upset Dr Dixon, because on 20th May, his letter appeared in the Times.
|
David Aaronovitch is right to argue for a robust scientific approach in medicine. However, he is not being logical or scientific when he says that if something is suspected to be placebo then it has no benefit and the NHS should not pay for it. What about scientific research on remedies that many believe to be placebo? These frequently show that there is a benefit but this is confined to those who believe in the treatment given. Surely, in such cases, it would be logical to say that the treatment was beneficial albeit in a specific group of “believers”. From there, it would be good science to compare the safety costs of this supposed placebo remedy with its currently given alternative before deciding whether “believers” should be able to receive such a remedy on the NHS. The problem here is that belief and mindset play an enormous part in healing – science needs to take account of this. Patients’ symptoms are frequently metaphors and effective treatment can often be symbolic and culturally dependent. The mind, in the right circumstances, can produce its own healing chemicals often mimicking those given in conventional medicine. Until science can explain healing in psychosocial as well as biomedical language, we must be cautious about “voting for the geeks” as Mr Aaronovitch suggests. It is far better surely that individual treatment should be tailored, within reason, to the patient and their beliefs and perspectives. Further more, might it not be wiser to direct NHS resources according to pragmatic trials of cost effectiveness and safety rather than a limited interpretation of science that excludes the effect of the mind? Dr Michael Dixon Chair of Council College of Medicine. |
This letter seemed remarkable to me. It is very close to being an admission that alternative medicine is largely placebo. It called for a reply.
We have been here before. Many people have discussed the dubious ethics of deceiving patients by giving placebos while pretending they are no such thing. There is wide agreement that it is not only unethical, but also unnecessary. Kevin Smith has written a scholarly essay on the topic. Edzard Ernst wrote Mind over matter? Margaret McCartney, the Glasgow GP, and author of The Patient Paradox, has explained it. Some views of Dr Dixon’s approach are less flattering than mine. For example, from the USA, Steven Novella’s Dr. Michael Dixon – “A Pyromaniac In a Field of (Integrative) Straw Men”. And, from Majikthyse, Michael Dixon caught red-handed!, and Dr Aust’s Dr Michael Dixon is annoyed. The list is almost endless.
.Two replies were published in the Times on 26 May (and they were the lead letters -bold print). One from the excellent Evan Harris, and one from me.
![]()

Here they are as text.
|
Sir, Dr Michael Dixon’s letter (May 21) is fascinating. He is, of course, a well-known advocate of alternative medicine. Yet he seems now to believe that much alternative medicine is just a placebo. That’s something the geeks have been saying for years, and he appears, at last, to have accepted it. That being the case, it follows that we have to ask whether placebos produce useful benefits, and whether it is ethical to prescribe them. Nobody denies the existence of placebo effects. But recent research has shown that they are usually both small and transient. Often they are not big enough to provide a useful degree of relief. For example, a recent paper on acupuncture in the British Journal of General Practice showed that it had a remarkably small placebo effect. And placebos have no effect at all on the course of cancer or infectious diseases. There has been an admirable movement in medicine for doctors to be open and honest with patients. Prescribing of medicines that contain no active ingredient involves lying to patients. That is old-fashioned and unethical. It is fair to ask why so many people seem to believe in alternative medicine, if even their placebo effects are small. The answer seems to lie in the “get better anyway” effect (known to geeks as regression to the mean). Most of the conditions for which placebos seem to work are things that wax and wane naturally. You take the “cure” when you are at your worst, and next day you are better. You would have been better anyway, but it’s hard to avoid attributing the improvement to whatever you took. That is why alternative medicine is advertised largely on the basis of anecdotal testimonials. And it is doubtless why Dr Dixon advocates “pragmatic” trials: that’s a euphemism for trials without a proper control group. Psychosocial problems may indeed be very important for some patients. But deceiving such patients with dummy pills is not the proper way to deal with their problems. D. Colquhoun, FRS Professor of Pharmacology, University College London Sir, Dr Michael Dixon argues that the NHS should fund placebo treatments such as homeopathy (though he stops short of agreeing that homeopathy is a placebo) on the basis that they can offer limited help to those who “believe” in them. It is no part of modern ethical medical practice to deceive patients into thinking — or failing to disabuse them of the belief — that an inert substance or ineffective medicine has beneficial effects. This can not be justified by the hope — or even expectation — of deriving for that patient the limited psychologically based improvement in symptoms that may follow from the deployment of the placebo. Pedlars of homeopathy for profit in the private sector will, alas, always seek to fool people into believing the hocus pocus of “memory of water” and the effects of infinite dilution and a lot of bottle-shaking. But doctors have responsibilities not to deceive their patients, even out of a paternalistic wish to assist them to manage their symptoms; and public policy demands that the NHS spends its resources only on treatments that work without deception in a cost-effective way. Dr Evan Harris Oxford |