
Download Lectures on Biostatistics (1971). Corrected and searchable version of Google books edition
Download review of Lectures on Biostatistics (THES, 1973).
NHS
It’s hard to know what to make of David Tredinnick MP (Cons, Bosworth). He is certainly an extreme example of the scientific ignorance of our parliamentary representatives, but he isn’t alone in that. Our present minister of Education, Michael Gove, memorably referred to Newton’s Laws of Thermodynamics, blissfully unaware that thermodynamics was a 19th century development. And our present Minister of Health seems to think that magic water cures diseases.
But Mr Treddinick breaks every record for anti-scientific nonsense. That, no doubt, is why he was upset by the recent revision of come NHS Choices web pages, so that they now give a good account of the evidence (that’s their job, of course). They did that despite two years of obstruction by the Department of Health. which seemed to think that it was appropriate to take advice from Michael Dixon of the Prince’s Foundation for integrated Health. That shocking example of policy based evidence was revealed on this blog, and caused something of a stir.
Treddinick’s latest letter
A copy of a letter from Mr Tredinnick to the Minister of Health, Jeremy Hunt, has some into my possession by a tortuous route [download the letter]. It’s a corker. Here are a few quotations.
"1. UKIP moving onto our ground
Attached is an extract from a recent UKIP policy statement. The position which UKIP has taken is one with which most of our Daily Mail reading supporters of complementary medicine would agree."
It seems that Treddinick’s preferred authority on medicine is now Nigel Farage, leader of the UK’s far right party. UKIP’s policy on health is appended to the letter, and it’s as barmy as most of the other things they say.
"2. Herbal Medicine
. . .there is very real concern that the Government will not regulate Herbal Medicine and Traditional Chinese Medicine. The current situation is unacceptable, because herbal practitioners need regulation and cannot function as herbal therapists, nor can they cannot obtain stocks of their herbal remedies, without it.
This refers to a saga that has been running for at least 10 years. Herbalists are desperate to get a government stamp of approval by getting statutory regulation, much like real doctors have, despite the fact that they make money by selling sick people "an unknown dose of an ill-defined drug, of unknown effectiveness and unknown safety" (as quoted recently in the House of Lords).
Even the US National Center for Complementary and Alternative Medicine (NCCAM) doesn’t claim that a single herbal treatment is useful. The saga of herbal regulation is long and tedious. The short version is that a very bad report, The Pittilo report, recommended regulation of herbalists. After years of prevarication, Andrew Lansley ignored the impartial scientific advice and yielded to the pressure from the herbal industry to accept the Pittilo report. But still nothing has happened.
Could it be that even Jeremy Hunt realises, deep down, that the regulation of nonsense is a nonsense that would harm the public?
We can only hope that a letter from Mr Tredinnick is the kiss of death. Perhaps his continuous pestering will only reinforce the doubts that seem to exist at the Department of Health.
Then Tredinnick returns (yawn) to his obsession with magic water. He vents his rage at the now excellent NHS Choices page on homeopathy.
3. Homeopathy
"Recently this wording has been removed and instead a comment by the Chief Medical Officer that homeopathy is placebo inserted in its place, as well as links to external organisations which campaign against homeopathy. For instance, there is a link to the Sense About Science website, and Caroline Finucane, who is Editor of new content at NHS Choices, also writes for the Sense About Science website. This is an organisation which has no expertise in homeopathy and traces its roots back to the ultra-left Revolutionary Communist Party (RCP)."
"I respectfully suggest that the original wording be reinstated and these links to external organisations be removed or changed to ensure a balanced view.".
So it seems that he prefers the medical views of Nigel Farage and the Prince of Wales to those of the Chief Medical Officer and the government’s chief scientist. Disgracefully, Tredinnick picks out one particular employee of NHS Choices among many, and one who does an excellent job. And he raises the hoary old myth that Sense About Science is a communist organisation. Odd, since others accuse it of being neo-libertarian. The actual history is here. The organisation that is a bit too libertarian for my taste is Spiked Online. I haven’t agreed with every word that Sense about Science has printed, but they have a totally honest belief in evidence.
To drag in the name of one person out of many, and to justify it by a false history shows, once again, how very venomous and vindictive the advocates of delusional medicine can be when they feel cornered.
A bit more information about Mr Treddinick
This is what the BBC News profile says about him.
|
David Tredinnick is an old style Conservative MP, being an Eton-educated former Guards officer, who has sat in the Commons since 1987. However, his ambition for high office was thwarted by his role in one of the sleaze stories which helped to sink the Major government. He accepted £1,000 from an undercover reporter to ask parliamentary questions about a fictitious drug. He was obliged to resign from his role as a PPS and was suspended from the Commons for 20 sitting days. He has not sat on the frontbench since. He is an orthodox Conservative loyalist, though he is more supportive of the European Union than many of his colleagues. He has, however, carved himself a niche as the Commons’ most enthusiastic supporter of complementary medicine. He has wearied successive health secretaries with his persistent advocacy of any and all homeopathic remedies. He has also supported their use in prisons and even suggested them as an aid in alleviating the foot and mouth crisis. |
|
Tredinnick has also asserted that he was aware of a psychiatric hospital that doubled its staff at full moon (this is an old urban myth, and is, of course, quite untrue). His advocacy of homeopathic borax as a way to control the 2001 epidemic of foot and mouth diease can be read here. Luckily it was ignored by the government. I hope his latest letter will be treated similarly. Picture of David Tredinnick MP from the Conservative Party |
 |
Follow-up
[Use Firefox if embedded videos do not show in Chrome]
Andrew Lansley’s Health Bill (HASSB) aims to change the NHS into something more like the US system, which gives worse results at twice the cost.
The only possible reason for wanting to do that is simple far-right ideology. No wonder that no hint was given of its intentions before the election.
On the contrary, David Cameron stated repeatedly that there would be no top-down reorganisation of the NHS. That turned out to be a straight lie.
“First let me tell you what we are not going to do. There will be no more of those pointless reorganisations that aim for change, but instead bring chaos.” [David Cameron speaking to Royal College of Nursing in 2009, before election].
We all know that money must be saved. But the two major disasters of the coalition government don’t save any money.
On the contrary, both tuition fees and NHS-wrecking will cost taxpayers’ money. The tuition fees are done (for the time being) but there is still time to save the NHS.
The best simple explanation that I’ve found is by Dr Max Pemberton in the Telegraph: Read this – and prepare to fight for your NHS. The Bill is three times longer than the 1946 Bill that brought the NHS into existence.
“The power to determine the services that make up the NHS will be transferred from the Secretary of State to newly created Clinical Commissioning Groups (CCGs), which are unelected. Members will include GPs but also company chief executives who can, if they wish, outsource decisions about the appropriate level of services offered to companies with commercial interests. This is what the Government means when it says it is handing GPs £60 billion of NHS money. ”
“Monitor. This quango is composed of unelected and unaccountable individuals. It will not have overarching responsibility – which the Government does currently – to ensure that everyone’s health needs are met.” “It will have the power to decide, on purely financial grounds, if an area loses its existing range of hospital services, such as A&E departments, with no duty to consider alternative provision.
“With so many different providers of health care created under this Bill, those with complex health care needs may not receive the joined-up medical care that the NHS now works hard to provide.”
“Less profitable patients – those requiring complex levels of care from multiple individuals and areas of expertise, for example – may be sidelined by these private companies. ”
“the Bill allows CCGs to contract out commissioning functions to private accountancy, health insurance and management consultant firms, which will be able to decide what care is provided free at the point of use through the NHS and what is not. This means that profit-making companies will be able to provide your clinical care and also decide what you’re entitled to under the NHS and from which care providers.” “There is the potential for commercial conflicts when the needs of shareholders come between doctors and patients. ”
“Providers, too, can reduce levels of service provision and entitlement to NHS-funded care and there are no restrictions on charging for non-NHS care.”
“Now, up to 49 per cent of income can be generated from private income. This means that almost half the beds currently used for NHS care could be given over to private patients.” “This could create a two-tier system in hospitals” and “create a conflict of interest, with hospitals having a clear incentive to encourage as many patients as possible to use the private half of their facilities. Moreover, hospitals can decide when to discharge patients. The requirement for coordinated discharge and aftercare of patients between health and social care is abolished in the Bill. “
Why is the bill needed at all?
Most people believe that there is no need for a bill. The real aim appears to be in part 3, which proposes a vast increase in private providers. Oliver Huitson says
“A US report comparing the health services of 7 major economies ranked the NHS 1st in terms of efficiency, and 2nd overall. The US, which has vast private sector involvement and much greater use of GP commissioning, was ranked last despite spending more than twice as much per head as the UK”
” Despite being ranked as one of the most efficient and equitable health services in the developed world, the Conservatives are determined to remodel it in the image of one of the least efficient – all in the name of “improving efficiency”.”
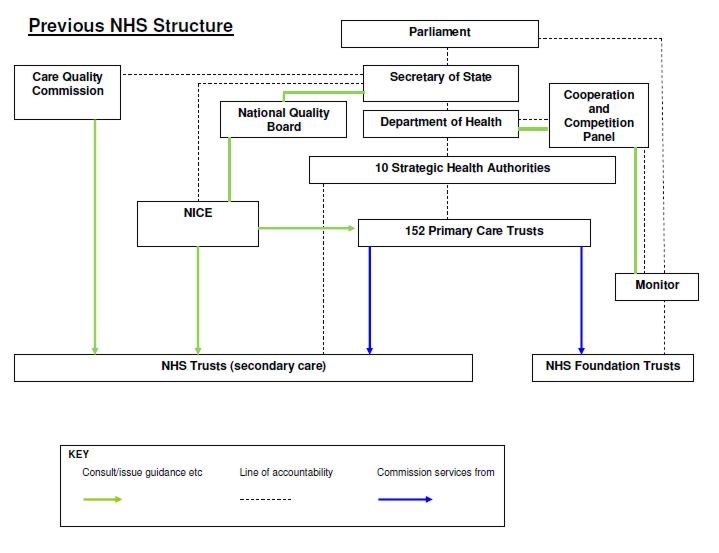
Although most GPs are in favour of having more say in what happens, even the first parts of the bill are a mess. They are advertised as reducing bureaucracy and reducing costs. According to the Financial Times, they do exactly the opposite.
“Here was the original NHS bureaucracy in graphic form”
Here is the new NHS bureaucracy in graphic form
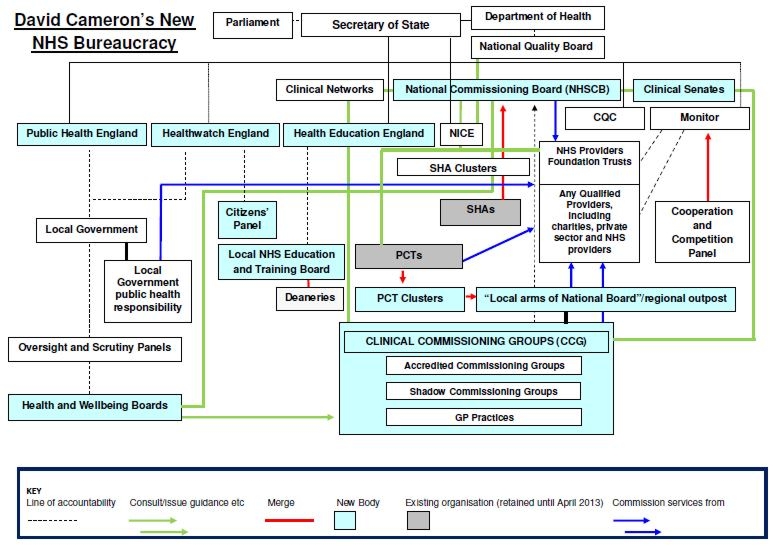
Ed Miliband pointed out that the number of NHS statutory organisations was growing from 163 to 521 – including “health and wellbeing committees,” “national commissioning boards”, “clinical networks”, “clinical senates” and so on.
So much for reduced bureaucracy.
Who thinks this is not a good idea?
Almost everyone. Not just the BMA which Lansley dismisses as a Trade Union, despite the fact that now (unlike in 1948) the BMA is voting against the financial interests of its members.
The Royal College of General Practitioners says Drop the Bill. So do Royal College of Nursing. Royal College of Midwives, Faculty of Public Health, Chartered Society of Physiotherapists, the Patients’ Association, among others. Almost the only support left is from the NHS Alliance, a tiny organisation run by Michael Dixon, friend of the Prince of Wales and advocate of quack medicine. The NHS alliance ran its own poll. A total of 100 people have voted so far, 99 of them against the Alliance’s policy. Some support. A rather good infographic shows how the balance lies.
The BMA’s General Practitioners Committee, which represents all GPs in the UK says [read full letter]
“1. Formally reaffirms its opposition to the NHS Health and Social Care Bill;
2. Believes that if passed the Bill will be irreversibly damaging to the NHS as a public service, converting it into a competitive marketplace that will widen health inequalities and be detrimental to patient care; . . . .”
In contrast, the e-petition to the government, started by Dr Kailash Chand OBE, states simply that it “Calls on the Government to drop its Health and Social Care Bill.”. It now has over 167,000 signatories. But despite the fact that petitions with over 100,000 signatures are meant to trigger a debate in the House of Commons, the backbench business committee of MPs has decided not to debate the e-petition.
So many people have rallied to oppose the daftness that it’s invidious to single out names. Nonetheless special mentions must go to Clare Gerada (@clarercgp on Twitter) (chair of the RCGP), and to Clive Peedell (@cpeedell) (oncologist and co-chair NHS Consultants’ Association) -read his Bevan’s Run blog. Among academics, Allyson Pollock and Martin McKee have done superb work on the details.
Most telling of all, some of the people who started by supporting Lansley have changed their minds. One concern about the “any qualified provider” idea is that it could open the door to quackery. Any “qualified” homeopath could bid for business at a competitive rate -sugar pills don’t cost much. Michael Dixon is one such.
Dr Sam Everington of Tower Hamlets is another. Services provided by his practice include “referrals to Inside Out Health and Wellbeing Ltd“. This private company will sell you fraudulent scams like homeopathy and kinesiology at £50 per session, among other nonsense (according to Companies House, it was wound up on 17 January 2012). He’s also associated with the “College of Medicine” (the reincarnation of the Prince of Wales’ Foundation). See also, Dr Margaret McCartney’s blog. As chair of the first Clinical Commissioning Group (CCG) he was embraced by Cameron. His Bromley-by-Bow surgery was host for Andrew Lansley’s first speech as health secretary after the 2010 election, and also host to the Prince of Wales..
But now even Everington has turned against the Bill (read the full letter).
“Dear Prime Minister
The Board of NHS Tower Hamlets Clinical Commissioning Group ask you to reflect and to withdraw the Health and Social Care Bill.”
“We care deeply about the patients that we see every day and we believe the improvements we all want to see in the NHS can be achieved without the bureaucracy generated by the Bill.
Your government has interpreted our commitment to our patients as support for the bill. It is not.”
And, on 1st March, another request to drop the bill, from the East London Integrated Care (ELIC is a not-for-profit social enterprise which is owned and run by local people and health professionals”). Read the full letter.
“Thursday, 1 March 2012 N1 5LZ
Dear Prime Minister,
The Board of City & Hackney Clinical Commissioning Group (CCG) join Tower Hamlets
and most other GPs and nurses and ask you to withdraw the Health and Social Care Bill.”
Is it really privatisation?
If you feel reassured by Lansley’s assurances that his measures aren’t de facto privatisation, just watch this video. It reveals some of the network of lobby groups that are circling the NHS, eager to take your money. For example, the lobby group, Policy Exchange, “Cameron’s favourite”, co-founded by Francis Maude, a member of Cameron’s cabinet, and is lobbying for more private sector provision of NHS services. One of the companies that it’s taken money from is called Tribal, which wants to take over commissioning from GPs. One of the directors of Tribal has described Andrew Lansley’s reforms as being “denationalisation of health services in England”.
So you don’t need to listen to left-wingers. The industry itself is in no doubt that it’s privatisation, and it’s ready and waiting to grab our money..
And of all unlikely allies, the vice chair of the British Holistic Medical Association has written a powerful letter about how the bill really would result in privatisation.
The likely consequences have been put well by Ben Goldacre in his What will happen with the NHS bill, in 5 tweets. The following points are based partly on this.
- GPs know they’re being set up to fail by being given commissioning powers, which they have neither the time nor the expertise to do properly.
- After GPs fail, private commissioning expertise will be needed. Large private companies will be given the job and they will come to operate like health insurers.
- These large bodies, like public/private insurance companies, will be able to pick and choose patients. They will naturally prefer the ones from whom they can make the most money (and not the sick or the old). Note that there is no geographical responsibility in the bill
- Small differences will gradually emerge in what services they offer. Top up plans will become available. And that will be the end of the NHS in the form in which we know it.
The only way that the proposals make any sense at all is if the underlying aim is to destroy the NHS, in anything like its present form. I believe that Lansley’s aims are much more to do with his personal political ideologies than anything to do with health. Those ideologies are far to the right of anything envisaged by Margaret Thatcher.
The politics. Where are the Lib Dems?
I voted Lib Dem in 2010, and I said precisely why. Of course I didn’t expect they’d get a majority. They were just the party that I found least objectionable. Like so many others I watched with horror as the numbers came out. There was no other option but to form a coalition with Conservatives. Well, I’d have been happier with no coalition, but the danger of that producing an overall majority for Conservatives after a year or so made that a very risky option.
When the coalition formed I was alarmed by the prospects for both education and for the NHS. I was less alarmed by the latter, because Cameron had said so many times that he had no intention of messing with the NHS. That turned out to be a direct lie. I could scarcely believe it when Lansley produced a plan after the election for the biggest reorganisation ever in the NHS, something that had not been foreshadowed in any way in the Conservative manifesto. This was one of the most dishonest bits of political manoeuvring that I’ve ever encountered.
Clearly we were spending more than we could afford. What’s unforgivable is to do things that actually cost the taxpayer more than before. Such actions are quite the opposite of cuts. Yet they are being done in the two areas, than any others, that have got Lib Dem voters angry.
(a) The £9k tuition fees cost the taxpayer more than the £3k fees did, because of the financing arrangements. I can see no conceivable reason for spending more taxpayers’ money than before apart from (Conservative) political ideology. That’s done (for now) so back to the main topic of this post, the NHS.
(b) It seems inevitable that Lansley’s proposals will cost money, not save money. Presumably that was predicted in the risk register, the concealment of which is a disgrace. See Liberal Conspiracy and the Green Benches blogs. The Information Commissioner ordered the release of the risk register, but the coalition refused (so much for transparent government). They appealed so now it goes to an Information Tribunal.
An Early Day Motion in the House of Commons urged release. It was signed by only 16 Lib Dems.
The bill started to fall apart in a major way when, on February 6th, The Times reported that
“Andrew Lansley should be taken out and shot,” says a Downing Street source. “He’s messed up both the communication and the substance of the policy.”
But Cameron, instead of grasping the chance, decided to back a loser.
Some Lib Dems have stuck to their principles. For example
John Pugh MP, Co-Chair of the Lib Dem Parliamentary Health Committee, re-established the Beveridge group, and wrote a letter to parliamentarians to explain why.
Andrew George MP wrote Health Bill has no friends. Dignified withdrawal would be best.
On 13 February, hearts soared when Lib Dem peer Shirley Williams spoke out at last. She urged Lansley to drop part 3 of the bill, the part that deals with privatisation. The elation didn’t last long though. Nick Clegg told the BBC: “Andrew Lansley is the architect of the NHS bill. He cares passionately about the NHS. He’s the right man for the job and he must see it through.”. Yes, I know about Cabinet solidarity, but it’s hard to think of any surer way to lose elections than to make statements like that. Even many Conservatives don’t believe it: see, for example, Dr Rachel Joyce on Conservative Home.
On 24th February, the Lib Dem president, Tim Farron MP, spoke up at last. “Mr Farron told ITV the bill should have been “massively changed” or dropped earlier and he wanted plans for more competition in the NHS to be dropped”.
On 26 February, Nigel Crisp, described the bill as a confusing mess that risks setting the NHS back. Crisp was formerly NHS chief executive and the permanent secretary at the Department of Health from 2000 to 2006, and is now a crossbench peer. Like everyone else, he was ignored.
The elation about Shirley Williams intervention didn’t last long. On 27th February a joint letter from Williams and Clegg claimed that they’d fixed the bill. The letter was quickly subjected to a bullshitometer analysis, by Health Policy Insight. Bafflingly, Lansley declared in public that he’d “changed his mind” about the privatisation, while at the same time Lansley and Cameron claimed that nothing much had changed: see Downing Street in knots as it plays down Nick Clegg’s NHS concessions, and Paul Corrigan’s blog.
March 1st saw two more blows for Clegg and Lansley. First, as reported thus in the Independent.
“Graham Winyard, the former deputy Chief Medical Officer, resigned from the party in protest at the leadership’s backing for the Bill. Dr Winyard, who was chairman of Winchester Liberal Democrats until last year, told Mr Clegg in a letter: “It is just not sensible to impose this top-down reorganisation on an NHS struggling to meet the biggest financial challenge in its history. To continue to do so in the face of near unanimous opposition from patient, staff and professional organisations simply invites slow motion disaster both for the NHS and for the party.” He said that he had no option but to resign “with great sadness”. “
Then, also on 1st March, Dr Laurence Buckman, chairman of the BMA’s GPs committee, wrote to 22,000 GPs. [full letter]
- Believes the bill will compromise the role of GPs, and could cause irreparable damage to the relationship between GPs and their patients.
- Believes the bill to be complex, incoherent and not fit for purpose, and almost impossible to implement successfully, given widespread opposition across the NHS workforce.
- Believes that passing the bill will be an irresponsible waste of taxpayers’ money, which will be spent on unnecessary reorganisation rather than on patient care, as well as increasing the running costs of the NHS from the processes of competition, and transaction costs
The chaos that the Lib Dems now find themselves in is illustrated clearly by a post on Liberal Democrat Voice by Andrew Tennant. He’s apparently an unreconstructed 19th century Whig, masquerading as a 21st century liberal. The comments on the post reveal the mess the party has got itself into by refusing to drop the bill.
More to the point, look at the proper detailed analyses done by people who are a lot more knowledgeable than Andrew Tennant, or Andrew Lansley.
- RCGP Report Stage Briefing – Health and Social Care Bill February 2012
- Allyson Pollock explains, line by line, a lot of problems that “Recent amendments put forward by the Liberal Democrats do not address”.
- Statement on Liberal Democrat amendments
Prof Allyson Pollock, David Price, Peter Roderick, and Tim Treuherz
28 February 2012 - Royal College of Physicians, in The Lancet “What began as a ham-fisted attempt to modernise the NHS has become a grotesque political disaster for government.”
- The NHS bill could finish the health service – and David Cameron Polly Toynbee says it as it is.
- A big document by SOSNHS -great source of links Breaking the NHS.
There is one last chance for the Lib Dems to restore their reputation. Lib Dems hope to finally kill health reforms. “Liberal Democrat activists will defy Nick Clegg over the Government’s controversial health reforms by seeking to “kill” them at a party policy-making conference next week.”
Good luck to them. They could save the Lib Dems if they win. Much more importantly, they could save the NHS.
Follow-up
Sunday 4 March. Yet another story of corruption, this time in the Mail on Sunday.
“The head of the NHS regulator that is meant to ensure fairness when private-sector firms bid for public contracts is also the chairman of a huge company whose Health Service business is worth £80 million a year – and set to increase massively.
As the chairman of the NHS Co-operation and Competition Panel (CCP), Lord Carter of Coles is paid £57,000 for two days’ work each week. But his other role, as chairman of the UK branch of the American healthcare firm McKesson, is more generously rewarded. Last year it paid him £799,000.”
“Dr Clare Gerada, chairman of the Royal College of General Practitioners, said: ‘He cannot have any credibility when he is also heading a company with such huge interests in the very contracts his organisation is meant to police.”
See also Conflicts of Interest and NHS reform.
According to a tweet from James Ball
“Politics of the #NHSbill awful for lib dems: only 17% of their current supporters back it – and only 9% of their 2010 voters.”
Sounds plausible. Are you listening, Nick Clegg?
5 March 2012. The emergency motion for the Lib Dem Spring Conference (March 10 -11) has been published. See also the blog of the heroic Dr Charles West for more details. If Clegg manages to defeat this excellent motion, the last chance to save the NHS will be gone.
10 March 2012
Bitterly disappointed by vote at Lib Dem conference, not to debate the motion to drop the NHS bill. Who do I vote for now?
One thing that one can still do is to email all Lib Dem MPs give your views. Here is a list of their email addresses (via Lindy).
bakern@parliament.uk, danny.alexander.mp@parliament.uk, alan.beith.mp@parliament.uk, gordon.birtwistle.mp@parliament.uk, brookea@parliament.uk, braket@parliament.uk, brownej@parliament.uk, hernandeza@parliament.uk, burstowp@parliament.uk, lorely.burt.mp@parliament.uk, cablev@parliament.uk, menzies.campbell.mp@parliament.uk, carmichaela@parliament.uk, nick.clegg.mp@parliament.uk, mike.crockart.mp@parliament.uk, farront@parliament.uk, daveye@parliament.uk, simon.wright.mp@parliament.uk, willottj@parliament.uk, featherstonel@parliament.uk, fosterd@parliament.uk, andrew.george.mp@parliament.uk, duncan.hames.mp@parliament.uk, stephen.gilbert.mp@parliament.uk, stephenwilliamsmp@parliament.uk, kennedyc@parliament.uk, jo.swinson.mp@parliament.uk, julian.huppert.mp@parliament.uk,hunterm@parliament.uk, simon@simonhughes.org.uk, chris.huhne.mp@parliament.uk, martin.horwood.mp@parliament.uk, hemmingj@parliament.uk, david.heath.mp@parliament.uk, hancockm@parliament.uk, pagep@parliament.uk, lambn@parliament.uk, lawsd@parliament.uk, john.leech.mp@parliament.uk, stephen.lloyd.mp@parliament.uk, michaelmooremp@parliament.uk, greg.mulholland.mp@parliament.uk, teathers@parliament.uk, tessa.munt.mp@parliament.uk, john.thurso.mp@parliament.uk, david.ward.mp@parliament.uk, webbs@parliament.uk, williamsmf@parliament.uk, williamsr@parliament.uk, pughj@parliament.uk, reida@parliament.uk, contact@danrogerson.org, susan.hislop@parliament.uk, robert.smith.mp@parliament.uk, stunella@parliament.uk, ian.swales.mp@parliament.uk
And here are email addresses for (most) Lib Dem peers)
williamss@parliament.uk, walmsleyj@parliament.uk, wallacej@parliament.uk, wallacew@parliament.uk, tordoffg@parliament.uk, topeg@parliament.uk, thomascm@parliament.uk, thomass@parliament.uk, stephenn@parliament.uk, smitht@parliament.uk, shipleyj@parliament.uk, shuttd@parliament.uk, sharpm@parliament.uk, scottrc@parliament.uk, robertsr@parliament.uk, rennardc@parliament.uk, randersonj@parliament.uk, palmerm@parliament.uk, oakeshottm@parliament.uk, northoverl@parliament.uk, newbyr@parliament.uk, millers@parliament.uk, methuenr@parliament.uk, methuenr@parliament.uk, maddockd@parliament.uk, maddockd@parliament.uk, maclennanr@parliament.uk, loombar@parliament.uk, linklaterv@parliament.uk, lestera@parliament.uk, leej@parliament.uk, kramers@parliament.uk, jonesn@parliament.uk, ecem@parliament.uk, harrisa@parliament.uk, hamwees@parliament.uk, greavesa@parliament.uk, goodhartw@parliament.uk, germanm@parliament.uk, gardens@parliament.uk, falknerk@parliament.uk, ezrad@parliament.uk, dholakian@parliament.uk, cotterb@parliament.uk, clementjonest@parliament.uk, chidgeyd@parliament.uk, carlilea@parliament.uk, brintons@parliament.uk, willisg@parliament.uk, addingtond@parliament.uk , alderdicej@parliament.uk, allanr@parliament.uk, ashdownp@parliament.uk, barkere@parliament.uk, benjaminf@parliament.uk , bonhamcarterj@parliament.uk
13 March 2012. This is really last chance day. At 11 am, the Lords debate third reading of health bill and at 2 pm the Commons have emergency debate, triggered by the e-petition, which now has more than 173,000 signatures. I sent the following email to all Lib Dem peers and MPs this morning.
|
The idea that the changes to the health bill have solved its problems is simply wrong. Before you vote, please read http://abetternhs.wordpress.com/2012/03/11/40points/ ,
That is written by a working GP who knows what he’s talking about. For the truth about the 49% disaster, read this. There are 27 professional organisations who are against the bill (see here). Do you really understand the implications better than they do? The vote at the lib dem conference gives you the mandate to vote according to your conscience. Please vote to drop the bill and start again. I voted Lib Dem at every election from 2001. If you let us down on the health bill, I will certainly not do so again. David Colquhoun |
16 March 2012. I have learned ( from Lord Shutt) that there will be a 3-line whip on Lib Dem peers to vote against Lord Owen’s amendment. And this despite the vote against the Clegg-Williams motion at the Lib Dem conference last week. This makes the much vaunted party democracy look like a bit of a joke. The only hope now is the bishops. Here is a list of their email addresses. You can also contact them through Dr Éoin Clarke’s site (from where I got the addresses)
bishop@bathwells.anglican.org, bishop@birmingham.anglican.org, chaplain@bishopofblackburn.org.uk, bishop@bristoldiocese.org, bpchester@chester.anglican.org, bishchichester@diochi.org.uk, bishop@bishopofderby.org, durham@durham.anglican.org, langrishm@parliament.uk, bshpglos@glosdioc.org.uk, bishop.christopher@cofeguildford.org.uk, bishop@hereford.anglican.org, bishop.tim@leccofe.org, bishop.lichfield@lichfield.anglican.org, bishopslodge@liverpool.anglican.org, bishop@londin.clara.co.uk, bishop@bishopscourt.manchester.anglican.org, bishop@newcastle.anglican.org, bishop@norwich.anglican.org, bishop@riponleeds-diocese.org.uk, bishop.nigel@stedmundsbury.anglican.org, bishop@bishopofwakefield.org.uk, contact@lambethpalace.org.uk, office@archbishopofyork.org
This is what I sent to them today.
|
Dear Bishop,
You will be aware of the widespread concerns about the commercialisation of the NHS. No fewer than 27 medical organisations have now come out strongly against the bill and it’s clear that, despite (or because of?) over 1000 amendments, it is a real mess. Despite the vote at the Lib Dems conference against the bill, I hear that there will be a 3-line whip in the Lords to force Lib Dem peers to vote against the very sensible proposal by Lord Owen to delay passing of the bill until the government release the assessment of the risks of passing it. This means that the Bishops will be crucial. I would like to ask you seriously to consider voting for Lord Owen’s motion on Monday. The future of the National Health Service lies in your hands Best regards |
18 March 2012. Tomorrow is last hope for stopping the bill in the Lords. The 3-line whip will, I expect, ensure the defeat of Lord David Owen’s excellent amendment. The bill will probably become law. Two tweets express the impending death of the NHS quite poignantly. On 15 March @Heardin London wrote
"For a brief period during 20th century, people gave a fuck and looked after each other. Unfortunately this proved unprofitable."
and today, from @thewritertype,
"Years from now you’ll have to explain to children what the NHS was. Then you’ll have to explain what a LibDem was."
Poetry in 140 characters.
20 March 2012.
|
The hated bill was rammed through in the House of Commons, thanks to support from Lib Dems. .The list of the peers and MPs who will make money out of privatisation is truly scary and deeply corrupt. |
|
This is a slightly-modified version of the article that appeared in BMJ blogs yesterday, but with more links to original sources, and a picture. There are already some comments in the BMJ.
The original article, diplomatically, did not link directly to UCL’s Grand Challenge of Human Wellbeing, a well-meaning initiative which, I suspect, will not prove to be value for money when it comes to practical action.
Neither, when referring to the bad effects of disempowerment on human wellbeing (as elucidated by, among others, UCL’s Michael Marmot), did I mention the several ways in which staff have been disempowered and rendered voiceless at UCL during the last five years. Although these actions have undoubtedly had a bad effect on the wellbeing of UCL’s staff, it seemed a litlle unfair to single out UCL since similar things are happening in most universities. Indeed the fact that it has been far worse at Imperial College (at least in medicine) has probably saved UCL from being denuded. One must be thankful for small mercies.
There is, i think, a lesson to be learned from the fact that formal initiatives in wellbeing are springing up at a time when university managers are set on taking actions that have exactly the opposite effect. A ‘change manager’ is not an adequate substitute for a vote. Who do they imagine is being fooled?
![]()
Click logo to go to BMJ
The A to Z of the wellbeing industry
From angelic reiki to patient-centred care
Nobody could possibly be against wellbeing. It would be like opposing motherhood and apple pie. There is a whole spectrum of activities under the wellbeing banner, from the undoubtedly well-meaning patient-centred care at one end, to downright barmy new-age claptrap at the other end. The only question that really matters is, how much of it works?
Let’s start at the fruitcake end of the spectrum.
One thing is obvious. Wellbeing is big business. And if it is no more than a branch of the multi-billion-dollar positive-thinking industry, save your money and get on with your life.
In June 2010, Northamptonshire NHS Foundation Trust sponsored a “Festival of Wellbeing” that included a complementary therapy taster day. In a BBC interview one practitioner used the advertising opportunity, paid for by the NHS, to say “I’m an angelic reiki master teacher and also an angel therapist.” “Angels are just flying spirits, 100 percent just pure light from heaven. They are all around us. Everybody has a guardian angel.” Another said “I am a member of the British Society of Dowsers and use a crystal pendulum to dowse in treatment sessions. Sessions may include a combination of meditation, colour breathing, crystals, colour scarves, and use of a light box.” You couldn’t make it up.
The enormous positive-thinking industry is no better. Barbara Ehrenreich’s book, Smile Or Die: How Positive Thinking Fooled America and the World, explains how dangerous the industry is, because, as much as guardian angels, it is based on myth and delusion. It simply doesn’t work (except for those who make fortunes by promoting it). She argues that it fosters the sort of delusion that gave us the financial crisis (and pessimistic bankers were fired for being right). Her interest in the industry started when she was diagnosed with cancer. She says
”When I was diagnosed, what I found was constant exhortations to be positive, to be cheerful, to even embrace the disease as if it were a gift. If that’s a gift, take me off your Christmas list,”
It is quite clear that positive thinking does nothing whatsoever to prolong your life (Schofield et al 2004; Coyne et al 2007; 2,3), any more than it will cure tuberculosis or cholera. “Encouraging patients to “be positive” only may add to the burden of having cancer while providing little benefit” (Schofield et al 2004). Far from being helpful, it can be rather cruel.
Just about every government department, the NHS, BIS, HEFCE, and NICE, has produced long reports on wellbeing and stress at work. It’s well known that income is correlated strongly with health (Marmot, M., 2004). For every tube stop you go east of Westminster you lose a year of life expectancy (London Health Observatory). It’s been proposed that what matters is inequality of income (Wilkinson & Pickett, 2009). The nature of the evidence doesn’t allow such a firm conclusion (Lynch et al. 2004), but that isn’t really the point. The real problem is that nobody has come up with good solutions. Sadly the recommendations at the ends of all these reports don’t amount to a hill of beans. Nobody knows what to do, partly because pilot studies are rarely randomised so causality is always dubious, and partly because the obvious steps are either managerially inconvenient, ideologically unacceptable, or too expensive.
Take two examples:
Sir Michael Marmot’s famous Whitehall study (Marmot, M., 2004) has shown that a major correlate of illness is lack of control over one’s own fate: disempowerment. What has been done about it?
In universities it has proved useful to managers to increase centralisation and to disempower academics, precisely the opposite of what Marmot recommends.
|
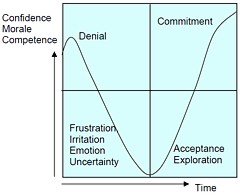
As long as it’s convenient to managers they are not going to change policy. Rather, they hand the job to the HR department which appoints highly paid “change managers,” who add to the stress by sending you stupid graphs that show you emerging from the slough of despond into eternal light once you realise that you really wanted to be disempowered after all. Or they send you on some silly “resilience” course. |
|
A second example comes from debt. According to a BIS report (Mental Capital and Wellbeing), debt is an even stronger risk factor for mental disorder than low income. So what is the government’s response to that? To treble tuition fees to ensure that almost all graduates will stay in debt for most of their lifetime. And this was done despite the fact that the £9k fees will save nothing for the taxpayer: in fact they’ll cost more than the £3k fees. The rise has happened, presumably, because the ideological reasons overrode the government’s own ideas on how to make people happy.
Nothing illustrates better the futility of the wellbeing industry than the response that is reported to have been given to a reporter who posed as an applicant for a “health, safety, and wellbeing adviser” with a local council. When he asked what “wellbeing” advice would involve, a member of the council’s human resources team said: “We are not really sure yet as we have only just added that to the role. We’ll want someone to make sure that staff take breaks, go for walks — that kind of stuff.”
The latest wellbeing notion to re-emerge is the happiness survey. Jeremy Bentham advocated “the greatest happiness for the greatest number,” but neglected to say how you measure it. A YouGov poll asks, “what about your general well-being right now, on a scale from 1 to 10.” I have not the slightest idea about how to answer such a question. As always some things are good, some are bad, and anyway wellbeing relative to whom? Writing this is fun. Trying to solve an algebraic problem is fun. Constant battling with university management in order to be able to do these things is not fun. The whole exercise smacks of the sort of intellectual arrogance that led psychologists in the 1930s to claim that they could sum up a person’s intelligence in a single number. That claim was wrong and it did great social harm.
HEFCE has spent a large amount of money setting up “pilot studies” of wellbeing in nine universities. Only one is randomised, so there will be no evidence for causality. The design of the pilots is contracted to a private company, Robertson Cooper, which declines to give full details but it seems likely that the results will be about as useless as the notorious Durham fish oil “trials”(Goldacre, 2008).
Lastly we get to the sensible end of the spectrum: patient-centred care. Again this has turned into an industry with endless meetings and reports and very few conclusions. Epstein & Street (2011) say
“Helping patients to be more active in consultations changes centuries of physician-dominated dialogues to those that engage patients as active participants. Training physicians to be more mindful, informative, and empathic transforms their role from one characterized by authority to one that has the goals of partnership, solidarity, empathy, and collaboration.”
That’s fine, but the question that is constantly avoided is what happens when a patient with metastatic breast cancer expresses a strong preference for Vitamin C or Gerson therapy, as advocated by the YesToLife charity. The fact of the matter is that the relationship can’t be equal when one party, usually (but not invariably) the doctor, knows a lot more about the problem than the other.
What really matters above all to patients is getting better. Anyone in their right mind would prefer a grumpy condescending doctor who correctly diagnoses their tumour, to an empathetic doctor who misses it. It’s fine for medical students to learn social skills but there is a real danger of so much time being spent on it that they can no longer make a correct diagnosis. Put another way, there is confusion between caring and curing. It is curing that matters most to patients. It is this confusion that forms the basis of the bait and switch tactics (see also here) used by magic medicine advocates to gain the respectability that they crave but rarely deserve.
If, as is only too often the case, the patient can’t be cured, then certainly they should be cared for. That’s a moral obligation when medicine fails in its primary aim. There is a lot of talk about individualised care. It is a buzzword of quacks and also of the libertarian wing which says NICE is too prescriptive. It sounds great, but it helps only if the individualised treatment actually works.
Nobody knows how often medicine fails to be “patient-centred.”. Even less does anyone know whether patient-centred care can improve the actual health of patients. There is a strong tendency to do small pilot trials that are as likely to mislead as inform. One properly randomised trial (Kinmonth et al., 1998) concluded
“those committed to achieving the benefits of patient centred consulting should not lose the focus on disease management.”
Non-randomised studies may produce more optimistic conclusions (e.g. Hojat et al, 2011), but there is no way to tell if this is simply because doctors find it easy to be empathetic with patients who have better outcomes.
Obviously I’m in favour of doctors being nice to patients and to listening to their wishes. But there is a real danger that it will be seen as more important than curing. There is also a real danger that it will open the doors to all sorts of quacks who claim to provide individualised empathic treatment, but end up recommending Gerson therapy for metastatic breast cancer. The new College of Medicine, which in reality is simply a reincarnation of the late unlamented Prince’s Foundation for Integrated Health, lists as its founder Capita, the private healthcare provider that will, no doubt, be happy to back the herbalists and homeopaths in the College of Medicine, and, no doubt, to make a profit from selling their wares to the NHS.
In my own experience as a patient, there is not nearly as much of a problem with patient centred care as the industry makes out. Others have been less lucky, as shown by the mid-Staffordshire disaster (Delamothe, 2010), That seems to have resulted from PR being given priority over patients. Perhaps all that’s needed is to save money on all the endless reports and meetings (“the best substitute for work”), ban use of PR agencies (paid lying) and to spend the money on more doctors and nurses so they can give time to people who need it. This is a job that will be hindered considerably by the government’s proposals to sell off NHS work to private providers who will be happy to make money from junk medicine.
Reference
Wilkinson. R & Pickett, K. 2009 , The Spirit Level, ISBN 978 1 84614 039 6
A footnote on Robertson Cooper and "resilience"
I took up the offer of Robertson Cooper to do their free "resilience" assessment, the company to which HEFCE has paid an undisclosed amount of money.
The first problem arose when it asked about your job. There was no option for scientist, mathematician, university or research, so I was forced to choose "education and training". (a funny juxtaposition since training is arguably the antithesis of education). It had 195 questions. mostly as unanswerable as in the YouGov happiness survey. I particularly liked question 124 "I see little point in many of the theoretical models I come across". The theoretical models that I come across most are Markov models for the intramolecular changes in a receptor molecule when it binds a ligand (try, for example, Joint distributions of apparent open and shut times of single-ion channels and maximum likelihood fitting of mechanisms). I doubt the person who wrote the question has ever heard of a model of that sort. The answer to that question (and most of the others) would not be worth the paper they are written on.
The whole exercise struck me as the worst sort of vacuous HR psychobabble. It is worrying that HEFCE thinks it is worth spending money on it.
Follow-up
Having recently been fired from Ofquack, the Complementary and Natural Healthcare Council (CNHC). I found I was missing the constant dribble of double-speak, Then, as luck would have it, a friend emailed me to draw my attention to a lucrative job at Ninewells Hospital, Dundee. On August 11th I put out a tweet, just in case any of my friends were interested.
How to save money. NHS Scorland (Tayside) advertises for homeopathic doctor http://bit.ly/9Ou9Yo Pathetic #fail
After the story appeared in the Daily Express it occurred to me that I should apply. It seems that NHS Scotland
Tayside) is determined to look idiotic in the eyes of the world. They advertised for a homeopathic doctor, The upper level of salary, £68,000 for two sessions a week, is a great deal more than I ever got paid as holder of the established chair of pharmacology at UCL, Then I discovered that a crystallographer, David Briggs (@xtaldave on twitter) had applied for the job. If he can, why not I? I found it hard to match the wit of his supporting statement, but just in case others want to apply, here’s my attempt. The more the merrier.
.
|
As a Fellow of the Royal Society for the last 25 years, and author of a textbook on statistics, I feel sure that I am capable of dealing with the intellectual rigours of handing out placebos to patients. I feel that my academic qualifications, and my authorship of many research papers, including several articles about homeopathy, should more than make up for my lack of formal qualifications in medicine or homeopathy. Indeed I have spent more time than I care to remember on reading the extensive literature on homeopathy. Having some expertise in the statistical analysis of clinical trials, my reading of the literature has equipped me well to impress gullible patients with sciencey sounding words like “succussion”, “energy medicine” and “quantum theory”. As an additional qualification, I have read widely about crystal healing, magnetic bracelets, aura photography and other such fairground paraphernalia which are designed, like homeopathy, to impress those with no knowledge of science or medicine. I have had over two years’ experience of serving on the Conduct and Competence Committee of the Complementary and Natural Healthcare Council, which has provided me with valuable insights into the world of alternative medicine. Indeed I have been told that my name is well known in Clarence House itself. If appointed to this job, I should like to combine it with research in homeopathy. I would approach this by using systems biology, in the hope that proteomics and metabolomics would be able to explain the still mysterious ability of medicines that contain no medicine to satisfy patients. People whom I know at the University of Westminster have proposed to use systems biology to explain Traditional Chinese Medicine, and I imagine that its application to homeopathy will be every bit as successful as theirs. To have cutting edge research of this sort will, I believe, give NHS Scotland a reputation that will spread around the world. I would also propose to save the Tayside PCT a lot of money, something not to be ignored in these hard times. At present, homeopathic pharmacies stock many thousands of sorts of pill. Recognising that the majority of them contain nothing at all, I’d retain the labels but fill all the bottles with sugar pills. This would save huge amounts of time and money, while having no effect at all on the outcome for patients. Despite my lack of formal qualifications, I hope you will agree that I’m qualified intellectually to meet the rigours of your job. |
Follow-up
I was not the only person to follow the example of David Briggs (@xtaldave). So far I’ve seen Dean Burnett (@garboy) on Science Digestive, Peter Harrison on Reality is My Religion, and Torgwen.
Three days on, there are at least eleven applications, and the three earliest ones have been read something like 12.000 times.
18 August 2010. Astonished to receive by snail-mail a straight-faced acknowledgment of my application from NHS Tayside [download pdf]. They ask me to send four copies of my CV and fill in forms for Equal Opportunities and Fitness to Practise. Does this mean I’ve been short-listed? This gets more surreal by the minute.
The Yuletide edition of the BMJ carries a lovely article by Jeffrey Aronson, Patent medicines and secret remedies. (BMJ 2009;339:b5415).
I was delighted to be asked to write an editorial about it, In fact it proved quite hard work, because the BMJ thought it improper to be too rude about the royal family, or about the possibility of Knight Starvation among senior medics. The compromise version that appeared in the BMJ is on line (full text link).
The changes were sufficient that it seems worth posting the original version (with links embedded for convenience).
The cuts are a bit ironic, since the whole point of the article is to point out the stifling political correctness that has gripped the BMA, the royal colleges, and the Department of Health when it comes to dealing with evidence-free medicine. It has become commonplace for people to worry about the future of the print media, The fact of the matter is you can often find a quicker. smarter amd blunter response to the news on blogs than you can find in the dead tree media. I doubt that the BMJ is in any danger of course. It has a good reputation for its attitude to improper drug company influence (a perpetual problem for clinical journals) as well as for clinical and science articles. It’s great to see its editor, Fiona Godlee, supporting the national campaign for reform of the libel laws (please sign it yourself).
The fact remains that when it comes to the particular problem of magic medicine, the action has not come from the BMA, the royal colleges, and certainly not from the Department of Health, It has come from what Goldacre called the “intrepid, ragged band of bloggers”. They are the ones who’ve done the investigative journalism, sent complaints and called baloney wherever they saw it. This article was meant to celebrate their collective efforts and to celebrate the fact that those efforts are beginning to percolate upwards to influence the powers that be.
It seems invidious to pick on one example, but if you want an example of beautiful and trenchant writing on one of the topics dealt with here, you’d be better off reading Andrew Lewis’s piece "Meddling Princes, Medical Regulation and Licenses to Kill” than anything in a print journal.
I was a bit disappointed by removal of the comment about the Prince of Wales. In fact I’m not particularly republican compared with many of my friends. The royal family is clearly good for the tourist industry and that’s important. Since Mrs Thatcher (and her successors) destroyed large swathes of manufacturing and put trust in the vapourware produced by dishonest and/or incompetent bankers, it isn’t obvious how the UK can stay afloat. If tourists will pay to see people driving in golden coaches, that’s fine. We need the money. What is absolutely NOT acceptable is for royals to interfere in the democratic political process. That is what the Prince of Wales does incessantly. No doubt he is well-meaning, but that is not sufficient. If I wanted to know the winner of the 2.30 at Newmarket, it might make sense to ask a royal. In medicine it makes no sense at all. But the quality of the advice is irrelevant anyway. The royal web site itself says “As a constitutional monarch, the Sovereign must remain politically neutral.”. Why does she not apply that rule to her son? Time to put him over your knee Ma’am?
Two of the major bits that were cut out are shown in bold, The many other changes are small.
BMJ editorial December 2009
Secret remedies: 100 years onTime to look again at the efficacy of remedies Jeffrey Aronson in his article [1] gives a fascinating insight into how the BMA, BMJ and politicians tried, a century ago, to put an end to the marketing of secret remedies. They didn’t have much success. The problems had not improved 40 years later when A.J. Clark published his book on patent medicines [2]. It is astounding to see how little has changed since then. He wrote, for example, “On the other hand the quack medicine vendor can pursue his advertising campaigns in the happy assurance that, whatever lies he tells, he need fear nothing from the interference of British law. The law does much to protect the quack medicine vendor because the laws of slander and libel are so severe.”> Clark himself was sued for libel after he’d written in a pamphlet “ ‘Cures’ for consumption, cancer and diabetes may fairly be classed as murderous”. Although he initially tried to fight the case, impending destitution eventually forced him to apologise [3]. If that happened today, the accusation would have been repeated on hundreds of web sites round the world within 24 hours, and the quack would, with luck, lose [4]. As early as 1927, Clark had written “Today some travesty of physical science appears to be the most popular form of incantation” [5]. That is even more true today. Homeopaths regularly talk utter nonsense about quantum theory [6] and ‘nutritional therapists’ claim to cure AIDS with vitamin pills or even with downloaded music files. Some of their writing is plain delusional, but much of it is a parody of scientific writing. The style, which Goldacre [7] calls ‘sciencey’, often looks quite plausible until you start to check the references. A 100 years on from the BMA’s efforts, we need once again to look at the efficacy of remedies. Indeed the effort is already well under way, but this time it takes a rather different form. The initiative has come largely from an “intrepid, ragged band of bloggers” and some good journalists, helped by many scientific societies, but substantially hindered by the BMA, the Royal Colleges, the Department of Health and a few vice-chancellors. Even NICE and the MHRA have not helped much. The response of the royal colleges to the resurgence in magic medicine that started in the 1970s seems to have been a sort of embarrassment. They pushed the questions under the carpet by setting up committees (often populated with known sympathizers) so as to avoid having to say ‘baloney’. The Department of Health, equally embarrassed, tends to refer the questions to that well-known medical authority, the Prince of Wales (it is his Foundation for Integrated Health that was charged with drafting National Occupational Standards in make-believe subjects like naturopathy [8]. Two recent examples suffice to illustrate the problems. The first example is the argument about the desirability of statutory regulation of acupuncture, herbal and traditional Chinese medicine (the Pittilo recommendations) [9]. Let’s start with a definition, taken from ‘A patients’ guide to magic medicine’ [10]. “Herbal medicine: giving patients an unknown dose of an ill-defined drug, of unknown effectiveness and unknown safety”. It seems to me to be self-evident that you cannot start to think about a sensible form of regulation unless you first decide whether what you are trying to regulate is nonsense, though this idea does not seem to have penetrated the thinking of the Department of Health or the authors of the Pittilo report. The consultation on statutory regulation has had many submissions [11] that point out the danger to patients of appearing to give official endorsement of treatments that don’t work. The good news is that there seems to have been a major change of heart at the Royal College of Physicians. Their submission points out with admirable clarity that the statutory regulation of things that don’t work is a danger to patients (though they still have a blank spot about the evidence for acupuncture, partly as a result of the recent uncharacteristically bad assessment of the evidence by NICE [12]). Things are looking up. Nevertheless, after the public consultation on the report ended on November 16th, the Prince of Wales abused his position to make a well-publicised intervention on behalf of herbalists [13]. Sometimes I think his mother should give him a firm lesson in the meaning of the term ‘constitutional monarchy’, before he destroys it. The other example concerns the recent ‘evidence check: homeopathy’ conducted by the House of Commons Science and Technology Select Committee (SCITECH). First the definition [10]: “Homeopathy: giving patients medicines that contain no medicine whatsoever”. When homeopathy was dreamt up, at the end of the 18th century, regular physicians were lethal blood-letters, and it’s quite likely that giving nothing saved people from them. By the mid-19th century, discoveries about the real causes of disease had started, but homeopaths remain to this day stuck in their 18th century time warp. In 1842 Oliver Wendell Holmes said all that needed to be said about medicine-free medicine [14]. It is nothing short of surreal that the UK parliament is still discussing it in 2009. Nevertheless it is worth watching the SCITECH proceedings [15]. The first two sessions are fun, if only for the statement by the Professional Standards Director of Boots that they sell homeopathic pills while being quite aware that they don’t work. I thought that was rather admirable honesty. Peter Fisher, clinical director of the Royal Homeopathic Hospital, went through his familiar cherry-picking of evidence, but at least repeated his condemnation of the sale of sugar pills for the prevention of malaria. But for pure comedy gold, there is nothing to beat the final session. The health minister, Michael O’Brien, was eventually cajoled into admitting that there was no good evidence that homeopathy worked but defended the idea that the taxpayer should pay for it anyway. It was much harder to understand the position of the chief scientific advisor in the Department of Health, David Harper. He was evasive and ill-informed. Eventually the chairman, Phil Willis, said “No, that is not what I am asking you. You are the Department’s Chief Scientist. Can you give me one specific reference which supports the use of homeopathy in terms of Government policy on health?”. But answer came there none (well, there were words, but they made no sense). Then at the end of the session Harper said “homeopathic practitioners would argue that the way randomised clinical trials are set up they do not lend themselves necessarily to the evaluation and demonstration of efficacy of homeopathic remedies, so to go down the track of having more randomised clinical trials, for the time being at least, does not seem to be a sensible way forward.” Earlier, Kent Woods (CEO of the MHRA) had said “the underlying theory does not really give rise to many testable hypotheses”. These two eminent people seemed to have been fooled by the limp excuses offered by homeopaths. The hypotheses are testable and homeopathy, because it involves pills, is particularly well suited to being tested by proper RCTs (they have been, and when done properly, they fail). If you want to know how to do it, all you have to do is read Goldacre in the Guardian [16]. It really isn’t vert complicated. “Imagine going to an NHS hospital for treatment and being sent away with nothing but a bottle of water and some vague promises.” “And no, it’s not a fruitcake fantasy. This is homeopathy and the NHS currently spends around £10million on it.” That was written by health journalist Jane Symons, in The Sun [17]. A Murdoch tabloid has produced a better account of homeopathy than anything that could be managed by the chief scientific advisor to the Department of Health. And it isn’t often that one can say that. These examples serve to show that the medical establishment is slowly being dragged, from the bottom up, into realising that matters of truth and falsehood are more important than their knighthoods. It is all very heartening, both for medicine and for democracy itself. David Colquhoun. Declaration of interests. I was A.J. Clark chair of pharmacology at UCL, 1985 – 2004. 1. Aronson, JK BMJ 2009;339:b5415 2. Clark, A,J, (1938) Patent Medicines FACT series 14, London. See also Patent medicines in 1938 and now https://www.dcscience.net/?p=257 3. David Clark “Alfred Joseph Clark, A Memoir” (C. & J. Clark Ltd 1985 ISBN 0-9510401-0-3) 4. Lewis, A. (2007) The Gentle Art of Homeopathic Killing 5. A.J. Clark (1927) The historical aspect of quackery, BMJ October 1st 1927 6. Chrastina, D (2007) Quantum theory isn’t that weak, (response to Lionel Milgrom). 7 Goldacre, B. (2008) Bad Science. HarperCollins 8. Skills for Health web site 9. A very bad report: gamma minus for the vice-chancellor 10. A Patients’ Guide to Magic Medicine, and also in the Financial Times. 12. NICE fiasco, part 2. Rawlins should withdraw guidance and start again 13. BBC news 1 December 2009 Prince Charles: ‘Herbal medicine must be regulated’. 14. Oliver Wendell Holmes (1842) Homeopathy and Its Kindred Delusions. 15. House of Commons Science and technology committee. Evidence check: homeopathy. Videos and transcripts available at http://www.viewista.com/s/fywlp2/ez/1 16. Goldacre, B. A Kind of Magic Guardian 16 November 2007. 17. Homeopathy is resources drain says |
Follow-up
There is a good account of the third SCITECH session by clinical science consultant, Majikthyse, at The Three Amigos.
16 December 2009.. Recorded an interview for BBC Radio 5 Live. It was supposed to go out early on 17th.
17 December 2009. The editorial is mentioned in Editor’s Choice, by deputy editor Tony Delamothe. I love his way of putting the problem "too many at the top of British medicine seem frozen in the headlights of the complementary medicine bandwagon". He sounds remarkably kind given that I was awarded (by the editor, Fiona Godlee, no less) a sort of booby prize at the BMJ party for having generated a record number of emails during the editing of a single editorial (was it really 24?). Hey ho.
17 December 2009. More information on very direct political meddling by the Prince of Wales in today’s Guardian, and in Press Association report.
17 December 2009. Daily Telegraph reports on the editorial, under the heading “ ‘Nonsense’ alternative medicines should not be regulated“. Not a bad account for a non-health journalist.
17 December 2009. Good coverage in the excellent US blog, Neurologica, by the superb Steven Novella.’ “Intrepid, Ragged Band of Bloggers” take on CAM‘ provides a chance to compare and contrast the problems in the UK and the USA.’
18 December 2009. Article in The Times by former special advisor, Paul Richards. “The influence of Prince Charles the lobbyist is out of hand. Our deference stops us asking questions.”
“A good starting point might be publication of all correspondence over the past 30 years. Then we will know the extent, and influence, of Prince Charles the lobbyist.”
Comments in the BMJ Quite a lot of comments had appeared by January 8th, though sadly they were mostly from the usual suspects who appear every time one suggests evidence matters. A reply was called for, so I sent this (the version below has links).
After a long delay, this response eventually appeared in the BMJ on January 15 2010.
It’s good to see so many responses, though somewhat alarming to see that several of them seem to expect an editorial to provide a complete review of the literature. I ‘ll be happy to provide references for any assertion that I made.
I also find it a bit odd that some people think that an editorial is not the place to express an opinion robustly. That view seems to me to be a manifestation of the very sort of political correctness that I was deploring. It’s a bit like the case when the then health minister, Lord Hunt, referred to psychic surgery as a “profession” when he should have called it a fraudulent conjuring trick. Anything I write is very mild compared with what Thomas Wakley wrote in the Lancet, a journal which he founded around the time UCL came into existence. For example (I quote)
“[We deplore the] “state of society which allows various sets of mercenary, goose-brained monopolists and charlatans to usurp the highest privileges…. This is the canker-worm which eats into the heart of the medical body.” Wakley, T. The Lancet 1838-9, 1
I don’t think it is worth replying to people who cite Jacques Benveniste or Andrew Wakefield as authorities. Neither is it worth replying to people who raise the straw man argument about wicked pharmaceutical companies (about which I am on record as being as angry as anyone). But I would like to reply directly to some of the more coherent comments.
Sam Lewis and Robert Watson. [comment] Thank you for putting so succinctly what I was trying to say.
Peter Fisher [comment]. I have a lot of sympathy for Peter Fisher. He has attempted to do some good trials of homeopathy (they mostly had negative outcomes). He said he was "very angry" when the non-medical homeopaths were caught out recommending their sugar pills for malaria prevention (not that this as stopped such dangerous claims which are still commonplace). He agreed with me that there was not sufficient scientific basis for BSc degrees in homeopathy. I suppose that it isn’t really surprising that he continues to cherry pick the evidence. As clinical director of the Royal London Homeopathic Hospital and Homeopathic physician to the Queen, just imagine the cognitive dissonance that would result if he were to admit publicly that is all placebo after all. He has come close though. His (negative) trial for homeopathic treatment of rheumatoid arthritis included the words "It seems more important to define if homeopathists can genuinely control patients’ symptoms and less relevant to have concerns about whether this is due to a ‘genuine’ effect or to influencing the placebo response” [2]. [download
the paper]. When it comes to malaria, it matters a lot.
Adrian White [comment] seems to be cross because I cited my own blog. I did that simply because if he follows the links there he will find the evidence. In the case of acupuncture it has been shown time after time that "real" acupuncture does not differ perceptibly from sham. That is true whether the sham consists of retractable needles or real needles in the "wrong" places. A non-blind comparison between acupuncture and no acupuncture usually shows some advantage for the former but it is, on average, too small to be of much clinical significance [3]. I agree that there is no way to be sure that this advantage is purely placebo effect but since it is small and transient it really doesn’t matter much. Nobody has put it more clearly than Barker Bausell in his book, Snake Oil Science [4]
White also seems to have great faith in peer review. I agree that in real science it is probably the best system we have. But in alternative medicine journals the "peers" are usually other true believers in whatever hocus pocus is being promoted and peer reveiw breaks down altogether.
R. M. Pittilo [comment] I’m glad that Professor Pittilo has replied in person because I did single out his report for particular criticism. I agree that his report said that NHS funding should be available to CAM only where there is evidence of efficacy. That was not my criticism. My point was that in his report, the evidence for efficacy was assessed by representatives of Herbal Medicine, Chinese Medicine and Acupuncture (four from each). Every one of them would have been out of work if they had found their subjects were nonsense and that, no doubt, explains why the assessment was so bad. To be fair, they did admit that the evidence was not all that it might be and recommended (as always) more research I’d like to ask Professor Pittilo how much money should be spent on more research in the light of the fact that over a billion dollars has been spent in the USA on CAM research without producing a single useful treatment. Pittilo says "My own view is that both statutory regulation and the quest for evidence should proceed together" but he seems to neglect the possibility that the quest for evidence might fail. Experience in the USA suggests that is exactly what has, to a large extent, already happened.
I also find it quite absurd that the Pittilo report should recommend, despite a half-hearted admission that the evidence is poor, that entry to these subjects should be via BSc Honours degrees. In any case he is already thwarted in that ambition because universities are closing down degrees in these subjects having realised that the time to run a degree is after, not before, you have some evidence that the subject is not nonsense. I hope that in due course Professor Pittilo may take the same action about the courses in things like homeopathy that are run by the university of which he is vice-chancellor. That could only enhance the academic reputation of Robert Gordon’s University.
George Lewith [comment] You must be aware that the proposed regulatory body, the Health Professions Council, has already broken its own rules about "evidence-based practice" by agreeing to take on, if asked, practitioners of Herbal Medicine, Chinese Medicine and Acupuncture. They have (shamefully) excluded the idea that claims of efficacy would be regulated. In other word they propose to provide exactly the sort of pseudo-regulation which would endanger patients They are accustomed to the idea that regulation is to do only with censoring practitioners who are caught in bed with patients. However meritorious that may be, it is not the main problem with pseudo-medicine, an area in which they have no experience. I’m equally surprised that Lewith should recommend that Chinese evaluation of Traditional Chinese medicine should be included in meta-analyses, in view of the well-known fact that 99% of evaluations from China are positive: “No trial published in China or Russia/USSR found a test treatment to be ineffective” [5]. He must surely realise that medicine in China is a branch of politics. In fact the whole resurgence in Chinese medicine and acupuncture in post-war times has less to do with ancient traditions than with Chinese nationalism, in particular the wish of Mao Tse-Tung to provide the appearance of health care for the masses (though it is reported that he himself preferred Western Medicine).
1. Lord Hunt thinks “psychic surgery” is a “profession”. https://www.dcscience.net/?p=258
2. Fisher, P. Scott, DL. 2001 Rheumatology 40, 1052 – 1055. [pdf file]
3. Madsen et al, BMJ 2009;338:a3115 [pdf file]
4. R, Barker Bausell, Snake Oil Science, Oxford University Press, 2007
5. Vickers, Niraj, Goyal, Harland and Rees (1998, Controlled Clinical Trials, 19, 159-166) “Do Certain Countries Produce Only Positive Results? A Systematic Review of Controlled Trials”. [pdf file]
15 January 2010. During the SciTech hearings, Kent Woods (CEO of the MHRA) made a very feeble attempt to defend the MHRA’s decision to allow misleading labelling of homeopathic products. Now they have published their justification for this claim. It is truly pathetic, as explained by Martin at LayScience: New Evidence Reveals the MHRA’s Farcical Approach to Homeopathy. This mis-labelling cause a great outcry in 2006, as documented in The MHRA breaks its founding principle: it is an intellectual disgrace, and Learned Societies speak out against CAM, and the MHRA.
22 January 2010 Very glad to see that the minister himself has chosen to respond in the BMJ to the editorial
|
Rt Hon. Mike O’Brien QC MP, Minister of State for Health Services I am glad that David Colquhoun was entertained by my appearance before the Health Select Committee on Homeopathy. But he is mistaken when he says, “you cannot start to think about a sensible form of regulation unless you first decide whether or not the thing you are trying to regulate is nonsense.” Regulation is about patient safety. Acupuncture, herbal and traditional Chinese medicine involve piercing the skin and/or the ingestion of potentially harmful substances and present a possible risk to patients. The Pittilo Report recommends statutory regulation and we have recently held a public consultation on whether this is a sensible way forward. Further research into the efficacy of therapies such as Homeopathy is unlikely to settle the debate, such is the controversy surrounding the subject. That is why the Department of Health’s policy towards complementary and alternative medicines is neutral. Whether I personally think Homeopathy is nonsense or not is besides the point. As a Minister, I do not decide the correct treatment for patients. Doctors do that. I do not propose on this occasion to interfere in the doctor-patient relationship. |
Here is my response to the minister
|
I am very glad that the minister himself has replied. I think he is wrong in two ways, one relatively trivial but one very important. First, he is wrong to refer to homeopathy as controversial. It is not. It is quite the daftest for the common forms of magic medicine and essentially no informed person believes a word of it. Of course, as minister, he is free to ignore scientific advice, just as the Home Secretary did recently. But he should admit that that is what he is doing, and not hide behind the (imagined) controversy. Second, and far more importantly, he is wrong, dangerously wrong, to say it I was mistaken to claim that “you cannot start to think about a sensible form of regulation unless you first decide whether or not the thing you are trying to regulate is nonsense". According to that view it would make sense to grant statutory regulation to voodoo and astrology. The Pittilo proposals would involve giving honours degrees in nonsense if one took the minister’s view that it doesn’t matter whether the subjects are nonsense or not. Surely he isn’t advocating that? The minister is also wrong to suppose that regulation, in the form proposed by Pittilo, would do anything to help patient safety. Indeed there is a good case to be made that it would endanger patients (not to mention endangering tigers and bears). The reason for that is that the main danger to patients arises from patients being given “remedies” that don’t work. The proposed regulatory body, the Health Professions Council, has already declared that it is not interested in whether the treatments work or not. That in itself endangers patients. In the case of Traditional Chinese Medicine, there is also a danger to patients from contaminated medicines. The HPC is not competent to deal with that either. It is the job of the MHRA and/or Trading Standards. There are much better methods of ensuring patient safety that those proposed by Pittilo. In order to see the harm that can result from statutory regulation, it is necessary only to look at the General Chiropractic Council. Attention was focussed on chiropractic when the British Chiropractic Association decided, foolishly, to sue Simon Singh for defamation. That led to close inspection of the strength of the evidence for their claims to benefit conditions like infant colic and asthma. The evidence turned out to be pathetic, and the result was that something like 600 complaints were made to the GCC about the making of false health claims (including two against practices run by the chair of the GCC himself). The processing of these complaints is still in progress, but what is absolutely clear is that the statutory regulatory body, the GCC, had done nothing to discourage these false claims. On the contrary it had perpetrated them itself. No doubt the HPC would be similarly engulfed in complaints if the Pittilo proposals went ahead. It is one thing to say that the government chooses to pay for things like homeopathy, despite it being known that they are only placebos, because some patients like them. It is quite another thing to endanger patient safety by advocating government endorsement in the form of statutory regulation, of treatments that don’t work. I would be very happy to meet the minister to discuss the problems involved in ensuring patient safety. He has seen herbalists and other with vested interests. He has been lobbied by the Prince of Wales. Perhaps it is time he listened to the views of scientists too. |
Both the minister’s response, and my reply, were reformatted to appear as letters in the print edition of the BMJ, as well as comments on the web..
This is a post about Markovian queuing theory. But hang on, don’t run away. It isn’t so hard.
|
The idea came from my recent experience. On Friday 23 October, I was supposed to have a kidney removed at the Royal Marsden Hospital. At the very last minute the operation was cancelled. That is more irritating than serious. A delay of a few weeks poses no great risk for me. . |

|
The cancellation arose because there was no bed available in the High Dependency Unit (HDU), which is where nephrectomy patients go for a while after the operation. Was this a failure of the NHS? I think not and here’s why
The first reaction of a neighbour to this news was to say "that’s why I have private insurance". Well, wrong actually. For a start, at the Marsden private patients and NHS patients get identical treatment (the only difference on the NHS is that "you don’t get hot and cold running margaritas at your bedside", my surgeon said). And secondly, the provision of emergency beds poses a really difficult problem, which I’ll attempt to explain.
Bed provision raises a fascinating statistical question. How many beds must be available to make sure nobody is ever turned away? The answer, in principle, is an infinite number. In practice it is more than anyone can afford.
The HDU has eleven beds but let’s think about a simpler case to start with. If patients arrived regularly at a fixed rate, and each patient stayed for a fixed length of time. there would be no problem. Say, for example, that a patient arrived regularly at 10 am and 4 pm each day, and suppose that each patient stayed for exactly 46 hours. It’s pretty obvious that you’d need four beds. Each bed could take a patient every two days and there are two patients per day coming in. Allowing two hours for changing beds, all four beds would be occupied for essentially 100 percent of the time, actually 95% = 46 hours/48 hours).
Random arrivals
The problem arises because patients don’t arrive regularly and they don’t stay for a fixed length of time. What happens if patients arrive at random and stay for a random length of time? (We’ll get back to the meaning of ‘random’ in this context later.)
Suppose again that two patients per day arrive on average, and that each patient stays in the HDU for 46 hours on average. So the mean arrival rate, and the mean length of stay in the HDU are the same as in the first example. When there was no randomness, four beds coped perfectly.
But with random arrivals and random length of stay the situation is very different. With four beds, if a queue were allowed to build up, the average number of patients in the queue would be 21 and the average length of time a patient would spend waiting to get a bed would be 10.5 days. This would be an efficient use of resources because every time a bed was vacated it would be filled straight away from the queue. The resources would be used to the maximum possible extent:, 95%. But it would be terrible for patients. The length of the queue would, of course, fluctuate, as shown by this distribution (see below) of the queue length. Occasionally it might reach 100 or more.
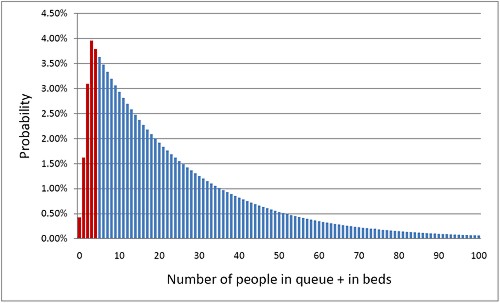
The histogram shows the total number of people in the system.The first five bins (red) represent the probabilities of 0, 1, 2, 3 or 4 beds being occupied. All the rest are in the queue.
What if you can’t queue?
For a High Dependency Unit or an Intensive Care Unit you can’t have a queue. If there is no bed, you are turned away. In the example just described, 91% of patients would have to wait, and that’s impossible in an HDU or ICU. The necessary statistical theory has been done for this case too (it is described as having zero queue capacity). Let’s look at the same case, with 4 beds, mean time between arrival of patients, 0.5 days, mean length of stay 1.917 days (46 hours).
|
In this case there is no queue so the only possibilities are that 0, 1, 2, 3 or all 4 beds are occupied. The relative probabilities of these cases are shown on the right (they add up to 100% because there are no other possibilities). |
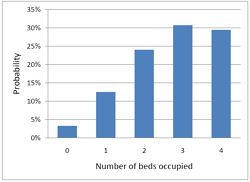
|
Despite the pressure on the unit, the randomness ensures that beds are by no means always occupied. All four are occupied for only 29% of the time and the average occupancy is 2.7 so the resources are used only 68% of the time (rather than 95% when a queue was allowed to form). Worse still, there is a 29% chance of the system being full, so you would be turned away.
So how many beds do you need? Clearly the more beds you have, the smaller the chance of anyone being turned away. But more beds means more cost and less efficiency. This is how it works out in our case.
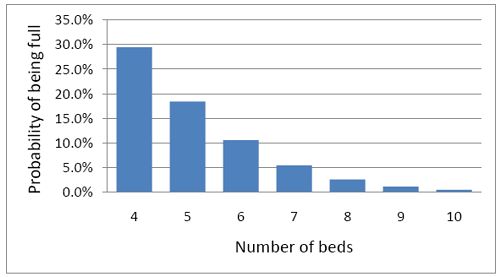
To get the chance of being turned away below 5%, rather than 29%, you’d have to double the number of beds from 4 to 8. But in doing so the beds would not be in use 68% of the time as with 4 beds, but for only 47% of the time.
|
Looked at another way, if you try to increase the utilisation of beds, above 50 or 60%, then the rate at which patients get turned away goes shooting up exponentially. |
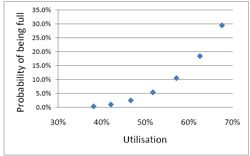
|
This isn’t inefficiency. It is an inevitable consequence of randomness in arrival times and lengths of stay.
A real life example
McManus et al. (2004) looked at all admissions to the medical–surgical Intensive Care Unit (ICU) of a large, urban children’s hospital in the USA during a 2-year period. (Anesthesiology 2004; 100:1271–6. Download pdf). Their Figure 2 shows the monthly average rejection rates mostly vary between 10 and 20%, so there is nothing unusual in there being no bed available in the private US medical system. For a period the rate of rejection reaches disastrous values, up to 47%. This happens, unsurprisingly, at times when the utilisation of beds was high.
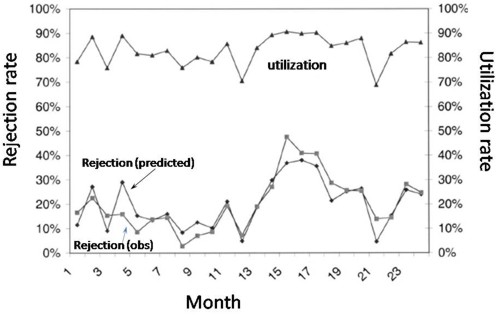
The observed relationship (McManus, Fig. 3) is very much as predicted above.with a very steep (roughly exponential) rise in rejection rate when the beds are in use for more than half the time.
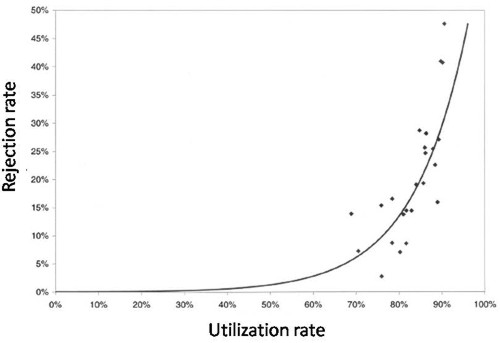
How to do the calculations
You can get the message without reading this section. It’s included for those who want to know a bit more about what we mean when we say that patients arrive at random rather than at fixed intervals, and that durations of stay in the unit have random rather than fixed durations.
Consider the durations of stay in the unit. They are variable in length and the usual way to represent variability is to plot a distribution of the variable quantity. The best known sort of probability distribution is the bell-shaped curve known as the Gaussian distribution. This is shown at the top of the Figure (note that pdf stands for probability density function, not portable document format).
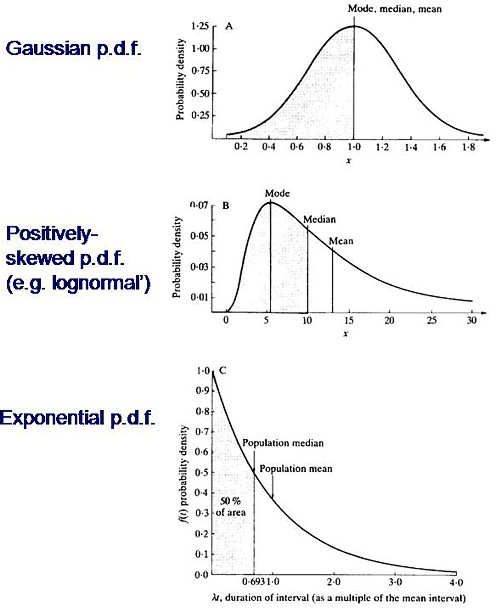
Not every sort of variability is described by a symmetrical bell-shaped curve. Quite often distributions with a positive skew are seen, like the middle example in the Figure. The distribution of incomes in the population have this sort of shape. Notice that more people earn less than average than earn more than average (the median is less than the mean). This can happen because those that earn less than average can’t get much less than average (unless we allow negative incomes), whereas bankers can earn (or at least be paid) a great deal more than average. The most frequent income (the peak of the distribution) is still smaller than the median.
An extreme form of a positively-skewed distribution is shown at the bottom. It is called the exponential distribution (because it has the shape of a decaying exponential curve). If this described personal incomes (and we are heading that way) it would mean that the most frequent income was zero and 63.2% of people earn less than average.
It is this last, rather unusual, sort of distribution that, in the simplest case, describes the lengths of random time intervals. This is getting very close to my day job. If an ion channel has a single open state, the lengths of individual ion channel openings is described by an exponential distribution.
|
The observation of an exponential distribution of durations is what would be predicted for a memoryless process, or Markov process. In the case of an ion channel, memoryless means that the probability of the channel shutting in the next microsecond is the same however long the channel has been open, This is exactly analogous to the fact that the probability of throwing a six with a die is exactly the same at each throw, regardless of how many sixes have been thrown before. |
Andrei A. Markov, 1856-1922 |
It is the simplest definition of a random length of time. For those who have done a bit of statistics, it is worth mentioning that if the number of events per unit time is described by a Poisson distribution, then the interval between events are exponentially-distributed. They are different ways of saying the same thing.
|
The lengths of stays in ICU in the McManus paper were roughly exponentially-distributed (right). The monthly average duration of stay ranged from 2.4 to 5.5 days, and average monthly admission rates to the 18 bed unit ranged from 4.6 to 6.2 patients per day. |
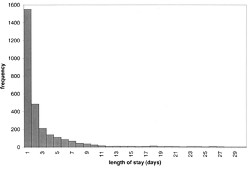
|
The monthly average percentage of patients who were turned away because there were no vacant beds varied widely, ranging from 3% up to a disastrous 47%
A technical note and an analogy with synapses
It’s intriguing to note that, in the simplest case, the time you’d spend waiting in a queue would have a simple exponential distribution (plus a discrete bit for the times when you don’t have to wait at all). The time you have to wait is the sum of all the lengths of stay of the people in front of you, and each of these lengths, in the case we discussing, is exponentially-distributed. If the queue was constant in length you can use a mathematical method known as convolution to show that the distribution of waiting time would follow a gamma distribution, a sort of distribution that goes through a peak, and eventually becomes Gaussian for long queues), However the queue is not fixed in length but its length is random (geometrically-distributed). It turns out that the distribution of the sum of a random number of exponentially distributed times is itself exponential. It is precisely this beautiful theorem that shows why the length of a burst of ion channel openings (which consists of the sum of a random number of exponentially-distributed open times, if you neglect the time spent in short shuttings) is, to a good approximation itself exponential, And that explains why the decay of synaptic currents is often close to following a simple exponential time course.
The calculations
The calculations for these graphs were done with a set of Excel add-in functions, Queueing Toolpak 4.0, which can be downloaded here. If this had been a paper of my own, rather than a blog post written in one weekend, I’d have done the algebra myself, just to be sure, The theory has much in common with that of single ion channels. Transitions between different states of the system can be described by transition rates or probabilities that don’t vary with time. The table, or matrix, of transition probabilities can be used to calculate the results, And if you want to know about the algebra of matrices, you could always apply for our summer workshop. There are some pictures from the workshop here.
Follow-up
Of course it is quite impossible for anyone who was around in the 60s to hear the name of a Russian mathematician without thinking of Tom Lehrer’s totally unjustified slur on another great Russian mathematician, Nicolai Ivanovich Lobachevsky. If you’ve never heard ‘Plagiarize’, you can hear it on Youtube. Sheer genius.
Why the size of the unit matters
This section was added as a result of a comment, below, from a statistician
At first glance one might think that if we quadruple the number of beds to 16 beds rather than 4, and we also quadruple the arrival rate to 8 rather than 2 per day, then the arrival rate per bed is the same and one might expect everything would stay the same.
As you say, it doesn’t.
If queueing was allowed, the mean queue length would be only slightly shorter, 18,7 rather than 20.9, but the mean time spent in the queue would fall from 10.5 days to 2.3 days.
In the more realistic case, with no queuing allowed, the rejection rate would fall from 29.4% to 15.5% and bed utilisation would increase from 68% to 81%. The rejection rate seems to fall roughly as the square root of the number of beds.
Clearly there is an advantage to having a big hospital with a big HDU.
Stochastic processes quite often behave unintuitive ways (unless you’ve spent years developing the right intuition).

Conservatives in the USA have been lying about the NHS on a massive scale. As Simon Hoggart comments today “There are few tribes more loathsome than the American right”.
In the forefront has been a far-right lobby group, Conservatives for Patients’ Rights (CPR). Even I was surprised to read in the Washington Post
“The campaign is being coordinated by CRC Public Relations, the group that masterminded the “Swift boat” attacks against 2004 Democratic presidential candidate, John F. Kerry”
CRC Public Relations is a conservative PR firm previously known as Creative Response Concepts. ‘Creative’ appears to mean ‘lying’, but I guess that is what PR is all about.
The founder of CPR, Rick Scott, has an interesting background. According to Stephen Barrett
“In 1987, he founded and became chief operating officer of a hospital chain that grew into the 23 billion-dollars-a-year Columbia/HCA. In 1997, a few weeks after the FBI raided HCA hospitals in five states, Scott was ousted as CEO and three executives were indicted on charges of Medicare fraud. The FBI’s investigation found that the hospital chain had been overbilling Medicare and giving kickbacks to doctors who steered patients to its hospitals. The overbilling included upcoding lesser procedures to get higher reimbursements and billing for lab tests that were not medically necessary and were not ordered by physicians. The situation was settled with a set of guilty pleas and criminal and civil fines totalling $1.7 billion. The U.S. Department of Justice referred to the matter as the “largest health care fraud case in U.S. history.”
Disgracefully, Karol Sikora, a former oncologist at the Hammersmith Hospital, supported CPR on US television. See Karol Sikora makes a fool of himself at NHSblogdoctor. I quote
“Karol Sikora had been duped by a slick American businessman into providing a “rent-a-quote” service for a notorious right-wing American organisation”
This post was reproduced on the US site, Trusted.MD
Sikora now works for the UK’s only private university and a private cancer treatment company. He is also famous for claiming,
falsely, to be a professor at Imperial College (he has an honorary contract with the Imperial College Hospital Trust but nothing with the University). And for promoting a load of nonsense about
alternative medicine (a lot more on that coming up shortly).
This is why love the NHS
Europe as a whole gets better health care for less money than in the USA. The fact that every US doctor has a financial interest in ordering expensive treatments whether they are needed or not,
is an obscenity. The fact that over 40 million Americans have no insurance is an obscenity (see The brutal truth about America’s healthcare).
Just look at the numbers (Source: WHO/OECD Health Data 2009)
Health spending as a share of GDP.
US 16% UK 8.4%
Public spending on healthcare (% of total spending on healthcare)
US 45% UK 82%
Health spending per head
US $7,290 UK $2,992
Practising physicians (per 1,000 people)
US 2.4 UK 2.5
Nurses (per 1,000 people)
US 10.6 UK 10.0
Acute care hospital beds (per 1,000 people)
US 2.7 UK 2.6
Life expectancy:
US 78 UK 80
Infant mortality (per 1,000 live births)
US 6.7 UK 4.8
My experience
Yes I know this is anecdote, but it matters a lot to me. I already posted a version of this story, but this seems like the time to repeat it.
On December 13th 1984, my wife had a subarachnoid haemorrhage when she was seven months pregnant. After an initial misdiagnosis by an obstetrician at St Peter’s Hospital, Chertsey, she was moved to UCH and diagnosed very quickly. The next morning I was called to see the neurourgeon, the great Alan Crockard. He was sitting surrounded by medical students some of whom I’d taught the previous year. He told me my wife had had a subarachnoid haemorrhage (at 33!) and they would operate straight away. And “I have to ask you, if we can save only the mother or the baby, which shall it be”. It’s as well to write that down because even 24 years later I can’t say it without a lump rising in my throat.
That same day she had neurosurgery to pin an aneurysm at the Maida Vale Neurosurgical Hospital, part of the UCLH group (it no longer exists). The surgeon, Alan Crockard, came out of theatre after five hours, looking rather tired and said “it was adhered to the optic chiasma on one side and about a millimetre from the pituitary on the other. It was a bit tricky but I think we got it”. Obstetricians were in theatre too because all this was done with the baby still in situ
| After a week in intensive care, under heavy sedation, Margaret’s blood pressure was not low enough and they decided to deliver the baby. At about 4 pm on a snowy Christmas Eve, a team of neurosurgeons and a team of obstetricians gathered and soon after, Andrew Stuart Colquhoun emerged in a small incubator to be whisked off in an ambulance to the Special Care Baby Unit at UCH (run, at that time, by Osmund Reynolds). Christmas day was spent in the hospital, with Margaret’s mother. Andrew weighed 1.4 kg at birth, but by Christmas day he had pulled out his ventilator himself, and was doing fine. He was so tiny that it was a couple of days before I dared to hold him. The Unit had racks of doll-sized clothes, knitted by volunteers. The care was superb. | 
Andrew (at 9 days) and Dad. Jan 2, 1985. Click for album. |
Once Margaret was well enough, she was given a side room in a neurosurgical ward with a cot for Andrew by her bed, an arrangement that gave the neurosurgical nurses some fun. They were in UCLH continuously until 27th April before Margaret had recovered enough to go home, [Full photo album here]
Now they are both fine.and Andrew is 6′ 7″ (200.5 cm)..
It is episodes like this that make one very proud of the NHS. She and Andrew were in hospital continuously for more than four months. Not a penny changed hands. Heaven knows what it would have cost in the USA, or even of insurance would have covered such a gargantuan bill.
Margaret & Andrew, with carer, Anna, June 2, 1985 |
Andrew (left) playing cricket in Bangladesh, Feb 2005. |
My own experience is trivial compared with that of Margaret and Andrew, but it has been as near perfect as anyone could wish. I had a lumbar spinal fusion (L3 – L4) in 1995, after several attempts at less drastic solutions. I’ve had two artificial hips. They allowed me to walk across the Alps for my 65th birthday. Then a few trivial things like bilateral hernia and DVT (I had been scanned and was on anticoagulant therapy within 4 hours of walking into UCLH’s Accident and Emergency). And now it looks as though I’ll be getting a partial or total nephrectomy too.
And not a penny has changed hands.
The NHS is a beautiful thing. OK it has has the usual excessive number of managers and HR-bollocks, like most big companies. It isn’t perfect but it is a great deal closer to perfection
than the US system.
 Approaching Seescharte (2600 m) at 08.20, 21 August 2001. Memminger Hütte visible below. With fused vertebrae and right prosthetic hip, thanks to the NHS. (Click for bigger picture.) |
Bush may have gone, but a large fraction of Americans seem to be unrepentant Bush-ites. Almost all of my many friends in the USA think more or less like I do. Even Obama is to the right of most European conservatives, The other 48% are to the right of Attila the Hun. The extent of the polarisation that still exists is nothing short of terrifying.
|
Thanks to the great Aneurin Bevan who established the NHS in 1948 for ordinary people like me, in the face of fierce opposition from the medical establishment.
|
 Statue of Bevan in Cardiff |
Ah well, The Daily Mash. is always there when you need a (wry) laugh
Follow-up
Paul Krugman in the New York Times is magnificent as always. In The Swiss Menace he points out that Obama’s scheme is nothing like the NHS anyway, but more like that in Switzerland.
“The plans on the table would, roughly speaking, turn America into Switzerland — which may be occupied by lederhosen-wearing holey-cheese eaters, but wasn’t a socialist hellhole the last time I looked.”
“In Britain, the government itself runs the hospitals and employs the doctors. We’ve all heard scare stories about how that works in practice; these stories are false.”
“So we can do this. At this point, all that stands in the way of universal health care in America are the greed of the medical-industrial complex, the lies of the right-wing propaganda machine, and the gullibility of voters who believe those lies.”
Comparing US and UK cancer statistics . As Ben Goldacre says, “I think you’ll find it’s a bit more complicated than that”. There’s an interesting analysis at Cancer Research UK
The US uses the PSA blood test far more widely than we do in the UK – despite questions over how effective it is at spotting cancers that would actually kill, as opposed to those that cause no symptoms. As a result, the USA has one of the highest recorded rates of prostate cancer in the world.
So although it’s undoubtedly ‘better’ at spotting prostate cancers, it’s also fair to say that some of these Americans will never die from their disease. This ‘overdiagnosis‘ inflates the survival statistics, at the expense of ‘overtreating‘ men – which is expensive and can cause long-term side effects (which can need further treatment).
In fact the age-standardised death rates per 100,000 people are almost the same in the UK (all races) when compared with the USA (whites only). What is different is that far more cases of prostate cancer are diagnosed in the USA. If the rate of ‘real’ (potentially fatal) prostate cancer were similar in both countries then both countries have much the same success in treating it, If, on the other hand, US men had a genuinely higher incidence of real prostate cancer, the US would be doing better, There is no way to distinguish between these two interpretations,
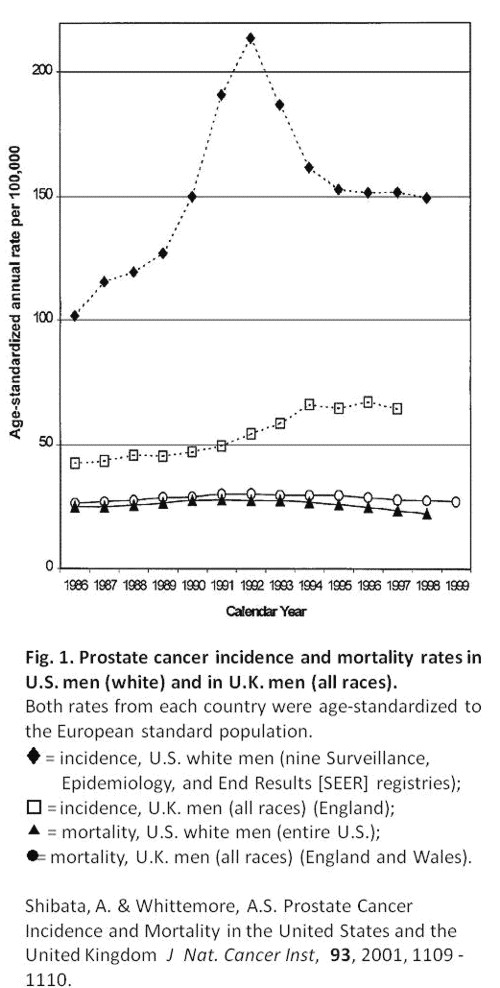
The first post was NICE falls for Bait and Switch by acupuncturists and chiropractors: it has let down the public and itself.
That was followed by NICE fiasco, part 2. Rawlins should withdraw guidance and start again.
Since then, something of a maelstrom has engulfed NICE, so it’s time for an update.
It isn’t only those who are appalled that NHS should endorse voodoo medicine on the basis of very slim evidence who are asking NICE to rethink their guidance on low back pain. Pain specialists are up in arms too, and have even started a blog, ‘Not Nearly as NICE as you think …‘, to express their views. Equally adverse opinions are being expressed in the Britsh Medical Journal. A letter there is signed by over 50 specialists in pain medicine. It ends thus
“Because of these new guidelines patients will continue to experience unnecessary pain and suffering and their rights to appropriately individually tailored treatment have been removed on the basis of a flawed analysis of available evidence. We believe the guidelines do not reflect best practice, remove patient choice and are not in our patients’ best interests.”
In a contribution headed “NICE misguidance”. Dr Michel Vagg ends
It seems to me that this guideline has been used as a propaganda vehicle to allow cherry-picked evidence to be enshrined as doctrine. This is an abuse of the guideline development process . . . ”
I have to say, though, that it seems to me that some of these people are promoting their own interests as much as chiropractors and acupuncturists. The evidence that spinal injections produce worthwhile benefits seems to be as thin as the evidence that chiropractic and acupuncture produce worthwhile benefits. But no doubt the injections are good for the budgets of PCTs or private practice doctors.. Could it perhaps be the case that some of the clinicians’ anger is being generated by doctors who are rushing to defend their own favourite ineffective treatment?
Why, oh why, can’t either NICE or the pain consultants bring themselves to state the obvious, that nothing works very well. The only thing that can be said for most of the regular treatments is that although they may not be much more effective than acupuncture or chiropractic, at least they don’t come with the intellectually-offensive hokum that accompanies the latter. Very sensible attempts have been made to identify the cause of low back pain [reviewed here], Occasionally they succeed. Mostly they don’t.
One clinician’s letter deserves special attention because it goes into the evidence, and the costs, in some detail. Its conclusions are very different from those in the NICE guidance.
The letter, a Review of NICE guidance, is from Dr C.J.D. Wells [download the whole letter]. He is a pain relief consultant from Liverpool.
Let’s look at some highlights.
Wells points out the absurdity of the cost estimates
“In the pricing section, they estimate that this will require an increase of facilities so that 3,500 patients can be treated instead of 1,000 at present (again see comments on pricing). This is not many treatments for the 20 million sufferers, of whom we can estimate that at least 2 million will have significant long-term disability and psychological distress”
And that is without even costing all the secondary costs of miseducating a new generation of students in fables about “Qi”, meridians, energy flow, subluxations and innate intelligence.
“The abysmal ignorance of the committee is reflected in the poor overall advice. So if you have a committee with special interests in Exercise, Manipulation, PMP’s, and Surgery, and you call an expert on Acupuncture, you get advice to use Exercise, Manipulation, Acupuncture, PMP’s and Surgery. Amazing.”
Another pain consutant, Charles Guaci, says in a comment in the Daily Mail.
I am a Pain Consultant of 30 years experience, have published two books (one translated into different languages).
NICE never asked me for my opinion.
This is the most ridicuculous pseudo-scientific document I have ever seen.
The panel consisted of a surgeon, psychologist, osteopath, acupuncturist a physiotherapist and an academic; not one pain consultant! The conclusions are simply a means of increasing the employment of their friends!
All evidence submitted to NICE was ignored.
It is almost certain than unless NICE rethink their ideas that Pain Consultants will be seeking a judicial review as well as full disclosure of how the panel arrived at their bizarre findings under the Freedom of information act.
Patients should realise that they are being taken for a ride.
Despite the outcry from opponents of magic medicine and from pain specialists, the assessment by the normally excellent NHS Choices site was disappointing. It made no mention at all of the secondary consequences of recommending CAM and described the assertions of the guidance group quite uncritically.
The reputation of NICE
NICE has been criticised before, though usually unjustly. In the past I have often supported them. For example. when NICE said that treatment of dementia with anticholinesterase drugs like galantamine was ineffective, there was a great outcry, but NICE were quite right. There is little or no rationale for such treatments, and more importantly, very little evidence that they work. But patients, especially when they are desperate, have greater faith in drug treatments than most pharmacologists, They want to clutch at straws. A bit like the NICE guidance committee, faced with a bunch of treatments most of which are almost ineffective, clutched at the straws of acupuncture and chiropractic. But this time it isn’t only the patients who are cross. It is most of the medical and scientific world too.
One interpretation of these bizarre events is that they represent a case of medical/scientific arrogance. Ben Goldacre wrote of another aspect of the same problem thus week, in Dodgy academic PR [download the paper on which this is based].
The first job of a scientist is to say openly when the answer to a question is not known. But scientists are under constant pressure to exaggerate the importance of their results. Last year we published an article which I feel may, if verified, turn out to be the second most important that I have ever been an author on. Because it happened to be published in Nature (not because of its quality), a press release was written (by an arts graduate!). It took some argument to prevent the distorted and exaggerated account being imposed on the public. This is typical of the sort of thing reported in Goldacre’s column. I reported a similar case a while ago, Why honey isn’t a wonder cough cure: more academic spin.
If NICE does not reconsider this guidance, it is hard to see how it can be taken seriously in the future. I hope that when NICE’s director, Professor Sir Michael Rawlins, returns from his trips abroad, he will find time to look at the case himself.
Indirectly, then, it can be argued that NICE’s bizarre guidance is just another manifestation of the management of science being passed from the hands of scientists into the hands of administrators and spin experts. It is yet another example of DC’s rule
Never trust anyone who uses the word ‘stakeholder’
Some bone-headed bureaucrat decides that any charlatan or quack is a ‘stakeholder’ in the provision of NHS care and gives them a quite disproportionate say in how taxpayers’ money is spent. The bureaucrats are so busy following processes and procedures, ticking boxes, and so deficient in scientific education, that they failed to notice that they’ve been caught out by the old trick of used car salesmen, bait and switch.
The consequences
The expected consequences have already started to materialise. The Prince of Wales’ Foundation for Magic Medicine is jubilant about having been endorsed by NICE. And I’m told that “The chiropractors have now just written letters to all health boards in Scotland asking for contracts for their services to deal with back pain”.
There could hardly have been a worse time for NICE to endorse chiropractic. We are in the middle of a storm about free speech because of the disgraceful action of the British Chiropractic Associaton in suing one of our best science writers, Simon Singh, for defamation because he had the temerity to express an opinion, Of course, even if the BCA wins in court, it will be the overall loser, because chiropractic claims are now being scrutinised as never before (just look at what they told me).
Follow-up
A much-cited paper. The paper that is most often cited by chiropractors who claim to be able to cure colic by spinal manipulation is Klougart N, Nilsson N and Jacobsen J (1989) Infantile Colic Treated by Chiropractors: A Prospective Study of 316 Cases, J Manip Physiol Ther,12:281-288. This is not easy to get hold of but Steve Vogel has sent me s scanned copy which you can download here. As evidence it is about as useless as the infamous Spence study so beloved of homeopaths. There was no control group at all. It simply follows 316 babies and found that most of them eventually got better. Well, they do, don’t they? It is a sign of the pathetic standard of reaearch in chiropractic that anyone should think this paper worth mentioning at all.
June 6 2009. More flak for NICE from the Royal College of Anaesthetists, and more adverse comment in the BMJ. And of course the blogs. for example, “If this is “evidence based medicine” I want my old job back“.
“Acupuncture on the NHS: a dangerous precedent”: a good analysis at counterknowledge.com.
June 6 2009, Comment sent to the BMJ. The comment was submitted, as below, early on Friday 5th June. The BMJ said it was a “sensitive issue” and for the next five days lawyers pondered over it.
Underwood and Littlejohns describe their guidance as being a “landmark”. I can only agree with that description. It is the first time that NICE has ever endorsed alternative medicine in the face of all the evidence. The guidance group could hardly have picked a worse moment to endorse chiropractic. Chiropractors find it so hard to find evidence for their practices that, when one of our finest science writers, Simon Singh, asked to see the evidence they sued him for defamation. I suggest that the guidance group should look at the formidable list of people who are supporting Singh, after his brave decision to appeal against this iniquitous persecution.
Of course I’m sure this bizarre decision has nothing to do with the presence on the guidance group of Peter Dixon, chair of the General Chiropractic Council. Nevertheless, I am curious to know why it is that when I telephoned two of the practices belonging to Peter Dixon Associates, I was told that they could probably treat infantile colic and asthma. Such claims have just been condemned by the Advertising Standards Authority.
The low back pain guidance stands a good chance of destroying NICE’s previously excellent reputation for dispassionate assessment of benefits and costs. Yes, that is indeed a landmark of sorts.
If NICE is ever to recover its reputation, I think that it will have to start again. Next time it will have to admit openly that none of the treatments work very well in most cases. And it will have to recognise properly the disastrous cultural consequences of giving endorsement to people who, when asked to produce evidence, resort to legal intimidation.
Eventually, on Wednesday 10 June the comment appeared in the BMJ, and it wasn’t greatly changed. Nevertheless if is yet another example of legal chill. This is the final version.
Underwood and Littlejohns describe their guidance as being a “landmark”. I can only agree with that description. It is the first time that NICE has ever endorsed alternative medicine in the face of all the evidence. The guidance group could hardly have picked a worse moment to endorse chiropractic. Chiropractors are so sensitive about criticisms of their practices that, when one of our finest science writers, Simon Singh, queried the evidence-base for their therapeutic claims they sued him for defamation. I suggest that the guidance group should look at the formidable list of people who are supporting Singh, after his brave decision to appeal against an illiberal court ruling in this iniquitous persecution.
One wonders whether this bizarre decision by NICE has anything to do with the presence on the guidance group of Peter Dixon, chair of the General Chiropractic Council. I am also curious to know why it is that when I telephoned two of the practices belonging to Peter Dixon Associates, I was told that chiropractic could be effective in the treatment of infantile colic and asthma. Similar claims about treating colic have just been condemned by the Advertising Standards Authority.
The low back pain guidance stands a good chance of destroying NICE’s previously excellent reputation for dispassionate assessment of benefits and costs. Yes, that is indeed a landmark of sorts.
If NICE is ever to recover its reputation, I think that it will have to start again. Next time it will have to admit openly that none of the treatments works very well in most cases. And it will have to recognise properly the disastrous cultural consequences of giving endorsement to people who, instead of engaging in scientific debate, resort to legal intimidation.
Bait and switch. Oh dear, oh dear. Just look at this. British Chiropractic Association tell their members to hide their sins from prying eyes.
Excellent round-up of the recent outburst of writing about “chiroquacktic” (Tut, tut, is there no respect?).
Dr Crippen writes “NICE recommends a cure for all known disease” [Ed some exaggeration, surely]
The National Health Executive (“the Independent Journal for Senior Health Service Managers) asked for an article about quackery. This is a version of that article with live links.
Download the pdf version.
There is a Russian translation here (obviously I can’t vouch for its accuracy).
On May 23 th 2006 a letter was sent to the chief executives of 467 NHS Trusts. It was reported as a front page story in the Times, and it was the lead item on the Today programme. The letter urged the government not to spend NHS funds on “unproven and disproved treatments”. Who can imagine anything more simple and self-evident than that? But in politics nothing is simple.
It turns out that quite a lot of patients are deeply attached to unproven and disproved treatments. They clamour for them and, since “patient choice” is high on the agenda at the moment, they quite often get them. Unproven and disproved treatments cost quite a lot of money that the NHS should be spending on things that work.
In January 2007, the Association of Directors of Public Health issued its own list of unproven and disproved treatments. It included, among others, tonsillectomy and adenoidectomy, carpal tunnel surgery and homeopathy. They all matter, but here I’ll concentrate on alternative treatments, of which homeopathy is one of the most widespread.
It should be simple. We have a good mechanism for deciding which treatments are cost-effective, in the form of the National Institute for Clinical Excellence (NICE). If homeopathy and herbalism are not good ways to spend NHS money, why has NICE not said so? The answer to that is simple. NICE has not been asked. It can consider only those questions that are referred to it by the Department of Health (DoH).
The government often says that it takes the best scientific advice, but the DoH seems to have something of a blank spot when it comes to alternative medicine. Nobody knows why. Perhaps it is the dire lack of anyone with a scientific education in government. Or could there be something in the rumour that the DoH lives in terror of being at the receiving end of a rant from the general direction of Clarence House if it doesn’t behave? Whatever the reason, the matter has still not been referred to NICE, despite many requests to do so.
A judgement from NICE would be useful, but it is hardly essential. It isn’t hard to understand. At its simplest the whole problem can be summed up very briefly.
- Homeopathy: giving patients medicines that contain no medicine whatsoever.
- Herbal medicine: giving patients an unknown dose of a medicine, of unknown effectiveness and unknown safety.
- Acupuncture: a rather theatrical placebo, with no real therapeutic benefit in most if not all cases.
- Chiropractic: an invention of a 19 th century salesmen, based on nonsensical principles, and shown to be no more effective than other manipulative therapies, but less safe.
- Reflexology: plain old foot massage, overlaid with utter nonsense about non-existent connections between your feet and your thyroid gland.
- Nutritional therapy: self-styled ‘nutritionists’ making unjustified claims about diet to sell unnecessary supplements.
Of these, ‘nutritional therapy’, or ‘nutritional medicine’, is a relative newcomer. At their worst, they claim that Vitamin C can cure AIDS, and have been responsible for many deaths in Africa. There isn’t the slightest need for them since the nutrition area is already covered by registered dietitians who have far better training.
There have been several good honest summaries of the evidence that underlies these interpretations, written in a style quite understandable by humanities graduates. Try, for example, Trick or Treatment (Singh & Ernst, Bantam Press 2008): a copy should be presented to every person in the DoH and every NHS manager. In some areas the evidence is now quite good. Homeopathy, when tested properly, comes out no different from placebo. That is hardly surprising because the ‘treatment’ pill contains no medicine so it is the same as the placebo pill.
Acupuncture has also been tested well in the last 10 years. A lot of ingenuity has been put into designing sham acupuncture to use as a control. There is still a bit of doubt in a few areas, but overwhelmingly the results show that real acupuncture is not distinguishable from sham. Acupuncture, it seems, is nothing more than a particularly theatrical placebo. All the stuff about meridians and “Qi” is so much mumbo-jumbo. In contrast, herbal medicines have hardly been tested at all.
It is quite easy to get an impression that some of these fringe forms of medicine work better than they do. They form efficient lobby groups and they have friends in high places. They long for respectability and they’ve had a surprising amount of success in getting recognised by the NHS. Some (like chiropractic) have even got official government recognition.
One can argue about whether it was money well-spent, but in the USA almost a billion dollars has been spent on research on alternative medicine by their National Center for Complementary and Alternative Medicine (NCCAM), which was set up as a result of political pressure from the (huge) alternative medicine industry. That has produced not a single effective alternative treatment, but at least it has shown clearly that most don’t work.
The letter of 23 May 2006 proved to be remarkably effective. Tunbridge Wells Homeopathic Hospital has closed and commissioning of homeopathic services has fallen drastically. That has released money for treatments that work, and providing treatments that work is the job of the NHS.
It is sometimes asked, what is wrong with placebo effects as long as the patient feels better? First it must be said that much of the apparent benefit of placebos like homeopathy isn’t a placebo effect, but merely spontaneous recovery. Echinacea cures your cold in only seven days when otherwise it would have taken a week. But when there is a genuine psychosomatic placebo effect, it can be a real benefit. As always, though, one must consider the cost as well as the benefit.
And there are a lot of hidden costs in this approach. One cost is the need to lie to patients to achieve a good placebo effect. That contradicts the trend towards more openness in medicine. And there is a major cost to the taxpayer in the training of people. If the NHS employs homeopaths or spiritual healers because they are nice people who can elicit a good placebo effect, the Human Resources department will insist that they are fully-qualified in myths. ““Full National Federation of Spiritual Healer certificate. or a full Reiki Master qualification, and two years post certificate experience” (I quote). That is one reason why you can find in UK universities, undergraduates being taught at taxpayers’ expense, that “amethysts emit high Yin energy”.
There is a solution to all of this. There is room in the NHS for nice, caring people, to hold the hands of sick patients. They might be called ‘healthcare workers in supportive and palliative care’. They could do a good job, without any of the nonsense of homeopathy or spiritualism. Likewise, manipulative therapists could get together to dispense with the nonsense elements in chiropractic, and to make a real attempt to find out what works best.
All that stands in the way of this common sense approach is the rigidity of Human Resources departments which demand formal qualifications in black magic before you can cheer up sick patients. The over-formalisation of nonsense has done great harm. You have only to note that Skills for Health has listed ‘competences’ in Distant Healing (in the presence of the client or in the absence of the client).
When I asked Skills for Health if they would be defining a ‘competence’ in talking to trees, I was told, in all seriousness, ““You’d have to talk to LANTRA, the land-based organisation for that”.
I’m not joking. I wish I were.
Follow-up
Jump to follow-up: Brian Kaplan
| Obama wins! Bush and Blair have gone. Could this mark the beginning of the end of the fashion for believing things that aren’t true? |
Trinity College Dublin: the Phil. “Creationism is a valid world view”
This is the 324th year of the Trinity College Philosophical Society (known locally as the ‘Phil’). Its former members include Bishop Berkeley, Dean Jonathan Swift, Oscar Wilde, Bram Stoker, Samuel Beckett, and E.T.S. Walton . It was founded for “discourse of philosophy, mathematics, and other polite literature ”, and is now a debating society.
The motion was Creationism is a Valid World view. At the dinner before the debate, the students all dutifully stood as one of them recited long graces in Latin both before and after eating. All very Oxbridge. So I wasn’t optimistic. However I hadn’t taken into account the conformist tendencies of undergraduates. Notwithstanding the Latin graces, the result of the debate was very clear indeed.
Result. The Creationists were totally wiped out. Almost the only vote for the motion was a young born-again student, who made a desperately sincere speech.
I don’t need to give the details of what happened, because the opposer of the motion, Bob Bloomfield (of the Natural History Museum) has given an excellent account (The Discovery Institute send big guns to Ireland but only manage to fire blanks) on the Beagle project blog. Two of the proposers were Americans, from the Discovery Institute, and they said what you’d expect: nothing that would impress anyone with any education. I’ll settle for Bloomfield’s description of me as “charmingly irascible”. Irascible, moi? Well it would make anyone mildly irritated to have to spend time arguing about creationism in 2008.
Religion, all religion, seems to me to be boring and not a thing worth wasting good time on thinking about, but the rise of barmy fundamentalism has made it essential, if only so that genetics can be taught without accusations of racism, I’m entirely with Dawkins, I can’t prove that there is no god, and I can’t guarantee
that the bottom of my garden is free of fairies. Both questions merit about the same amount of time, though if pressed, I’d go for the fairies. They are, allegedly, rather better behaved than gods.
The 24th president of the USA said, when asked for his thoughts on evolution, said
“of course like every other man of intelligence and education I do believe in organic evolution. It surprises me that at this late date such questions should be raised”.
Woodrow Wilson, 1922
That, of course, was from a president who has been described as ” leading intellectual of the Progressive Era”.
How things have changed in the time of Tony Blair, George Bush and Sarah Palin. Very few people had such barmy beliefs in 1960, never mind 1922. My thesis is much the same as that of Francis Wheen in “How mumbo-jumbo conquered the world” Sometime around 1980, with the conjunction of Thatcher, Reagan and Khomeini it came into fashion to believe things that aren’t true, just because you wished they were (actually I’d put it a bit earlier than Wheen: arguably it started when the Beatles went to that guru), It was after that when suddenly people started to believe in magic medicine, religious fundamentalism. weapons of mass destruction, and, ahem, that the market would make us rich if only we would remove all the regulations.
Tony Blair defended in parliament the Emmanuel School which is run by a young earth creationist and used car dealer, Peter Vardy. The head of the school, Nigel McQuoid, features strongly on the web site of the Christian Institute, This curious organisation seems to be devoted largely to creationism, homophobia and the virtue of beating children (a search of the site for “corporal punishment” gives 43 hits). An essay by Burns & McQuoid says
“There are those who argue that Science and Christianity can be harmoniously reconciled . ; ;. We cannot subscribe to this view”
The former head of science (yes, of science) at McQuoid’s school, Steven Layfield, had an article on the Christian Institute web site. It vanished as soon as it got some publicity but you can read it at http://www.darwinwars.com/lunatic/liars/layfield.html.
Try this quotation.
“Note every occasion when an evolutionary/old-earth paradigm (millions or billions of years) is explicitly mentioned or implied by a text-book, examination question or visitor and courteously point out the fallibility of the statement. Wherever possible, we must give the alternative (always better) Biblical explanation of the same data.”
| These guys are really at the fruit-cake end of the religious spectrum. In contrast, the young anglican chaplain of Trinity, Darren McCallig, spoke against creationism, eloquently and sensibly. His religiousness did seem at times to be diluted almost to homeopathic extremes, but all the better for that. He seems to have a sense of humour too, judging by the poster for his services. |  click to enlarge |
There is, of course, a very healthy opposition to creationists in the USA too, I like particularly Gerald Weissman’s article “The facts of evolution: fighting the Endarkenment” (it may have been the first time that I saw the wonderful word endarkenment, which describes so well the last 30 years). It starts thus.
“Those of us who practice experimental science are living in the best of times and the worst of times, and I’m not talking about A Tale of Two Cities, but a tale of two cultures. “
Here are a couple of pictures of the meeting.
Chris Stillman (geologist)

Berlinski (left) Luke Ryder (speaking), Bloomfield, DC, Stillman (right)
And some pictures of Dublin here

James Joyce, TCD quadrangle and Molly Malone. Click to view
UCL homeopathy debate
This was organised by the UCL students’ debating society. The Darwin Lecture theatre was surprisingly full for this debate, but they weren’t all students. As usual on these occasions, the homeopaths tried to pack the audience, but this time they failed. That tactic is fair enough I suppose, but it means that the vote failed to tell us anything much about the opinion of students, beyond the fact that not many of them opposed the motion.
There are a few though. To the horror of some of our pharmacology and neuroscience undergraduates, a student society devoted to medicines that don’t work has been started at UCL, for the first time ever. Luckily, it seems to be a rather small society. I was fascinated to see that they are going to hear about the evidence base for complementary therapies, from George Lewith. I had occasion a while ago to look at Dr Lewith’s attitude to evidence: see Lewith’s private clinic has curious standards.
| The proposers were Simon Singh and me. Simon is author of, among other things, Fermat’s Last Theorem and Trick or Treatment. I thought he did an excellent job. Singh pointed out that, contrary to the view propagated by quacks, science likes wacky ideas, as long as you can produce the evidence for them He cited dark matter as an example. |
 |
The main opposer was my old friend Peter Fisher, homeopathic physician to the Queen. It was a pleasure to show the video of Fisher agreeing with me that there is not enough science in homeopathy to justify a BSc degree in it. Fisher, in his papers, strikes me as one of the most honest of homeopaths. He was “very angry” when homeopaths were caught out recommending their sugar pills to prevent malaria. But is his speech, he struck me as less than honest. He cherry-picked the evidence quite shamelessly as usual. And his suggestion that there was an analogy between the ‘memory of water’ and a DVD was disposed of ably by a physics student who spoke from the floor.
The results were too close for comfort, 65 for, 53 against and an amazing 37 abstentions,
Sadly we’ll never know how the students voted, because of the imported homeopaths.
| Dr Brian Kaplan was there. He had given the meeting some advance publicity, in a web posting that also kindly gave publicity to our 2006 letter to the Times. He didn’t like the letter, which is unsurprising given that it turned out to be more effective than we could ever have hoped (see also here). |  |
On the second row, getting very excited, was homeopath Grace Da Silva-Hill and her husband, She runs the ‘Healing with Grace’ business. On her web site she makes the ludicrous claim that
“Homeopathy will treat the cause of your health problem, not just alleviate your symptom”
She also says, inter alia, that
“Homeopathy is effective in treating a wide range of conditions such as: asthma, . . . “
In contrast, the Cochrane review says
“There is not enough evidence to reliably assess the possible role of homeopathy in asthma. “
I have been sent her account of the debate (a reply to a query from the ubiquitous Dana Ullman).
“Hello Dana, The debate, on monday 20th Oct., organised by UCL debating society, was poorly managed, and biased, attended mostly by students, who appear to have gone there to practice their debating skills. The motion was lost by 12 (65 for and 53 against), with 37 abstentions. Peter Fisher put on a good show, and so did his second, in comparison with the rather stale and poor presentation of Simon and Qulquoun (sorry, can never spell this). My husband Ken did a rather
good caricature of him, unfortunately can’t share it here. Pity there were not more homeopaths/supporters there. Kind regards,”
Uhuh. Well, I guess she would say that.
You can judge the critical faculties of Mrs Da Silva-Hill from a comment she left on a piece in the Daily Telegraph, ‘Homeopathy putting lives at risk with claims’. I quote from it verbatim.
“The public does not care about the research available, the public care about having their health problem sorted, where conv. medicine has failed,”
(I apologise for attributing to Mrs Da Silva in the original post a quotation from the Telegraph that appeared above her name but was actually written by somebody else. I apologise also for using a picture of her without permission.)
On the way out of the debate, I walked back to Euston Road with another homeopath, William Alderson, who had come all the way from Kings Lynn to cast his vote. He was earnest and sincere, the conversation was amicable but his idea of evidence was so different from mine that no progress was made. You can read more about Alderson on Dr Aust’s blog.
It’s fascinating stuff.
Follow-up
Dr Brian Kaplan has posted some splenetic comments on this post. I suppose the paranoid tone is an indication that we are winning, but I do wish he’d be a bit more careful about the facts. Let me correct some of them.
(1)Neither the letter of May 2006, nor its follow up in May 2007, was written under the NHS letterhead. The follow-up letter of May 2007 contained the words
“If you have not already reviewed your own trust’s provision, you might find it useful to consider, in conjunction with your Director of Public Health, the paper that we have enclosed which, while not a full review of the scientific position, has been used by other trusts to promote evidence based commissioning.”
The enclosed form was a sample commissioning letter which reproduced the NHS logo with a notice saying “insert your NHS logo here”. The accompanying letter made it perfectly clear that the enclosed form was simply an example to help those who wanted to save money and not an official NHS communication.
(2) Kaplan says I accuse him of lying to his patients, but his reference is to (an old version of) my Dilemmas at the heart of alternative medicine. It says nothing of the sort. I have said many times that I believe homeopaths are perfectly sincere, but they are just deluded. The reference to lying in the ‘dilemmas’ concerns how to get the maximum placebo effect when you know it is a placebo. Homeopaths have not reached that stage yet.
All this information has been available since May 2007. He should have checked.