
Download Lectures on Biostatistics (1971). Corrected and searchable version of Google books edition
Download review of Lectures on Biostatistics (THES, 1973).
David Colquhoun
Balance in reporting | Call You and Yours | Report on regulation | Cancer video
In the wake of the report by the Science and Technology Committee (STC) on the lack of evidence for homeopathy, and the Chinese medicine poisoning, the BBC carried at least three very bad reports. Being a strong supporter of the BBC that saddens me.
Nevertheless it has to be said that the BBC does not always do very well on science reporting. Too many of the reports are anonymous -you don’t know who to blame or who to write to. Worse still, the BBC’s reports on its web site usually fail to link to original sources. This is unforgiveable: the ability to link to sources is the huge advantage of the web over print media.
The problem of balance in media reports
The question of balance is important. Ofcom imposes an obligation that reporting should reflect the balance of viewpoints. Section 5 of Ofcom’s broadcasting code says (emphasis is mine).
“Section 5: Due Impartiality and Due Accuracy and Undue Prominence of Views and Opinions”
“To ensure that news, in whatever form, is reported with due accuracy and presented with due impartiality.”
“Meaning of “due impartiality”: “Due” is an important qualification to the concept of impartiality. Impartiality itself means not favouring one side over another. “Due” means adequate or appropriate to the subject and nature of the programme. So “due impartiality” does not mean an equal division of time has to be given to every view, or that every argument and every facet of every argument has to be represented.”
The BBC Trust has a very similar definition of "due impartiality".
It seems to me that in practice producers tend to use "equal time" too much, and that this often gives a quite misleading impression of the state of play of informed opinion. Nevertheless, inappropriate use of “equal time” is so common that it would not be worth a formal complaint. This post concerns cases of very unequal time,
Somebody said recently, it is as though after an air crash one gave equal time to the air accident investigator and a representative gravity-deniers association. That is scarcely an exaggeration of what happened on the BBC after the STC’s report.
Worse still, far more time was given (especially on ‘Call You and Yours’) to the viewpoint that any scientist, indeed any informed person, would regard as quackery.
This post gives details of three examples of highly partial reporting and it is the basis of complaints to the BBC. But since complaints to the BBC about science reporting rarely get far, a complaint
is being sent also to Ofcom.
(1) Call You and Yours: a platform for herbalists
You and Yours is often quite a good programme, They did an excellent job on a "snoring remedy" which I had unearthed. But on Tuesday 23 February they did a "Call You and Yours" phone-in programme which was badly researched and highly partial.
The presenter, Julian Worricker, didn’t know enough about the topic to ask the right questions, though I’d guess that the blame for the poor quality must lie more with the person who decided that the only "expert" on the programme was a herbalist, and with the people who screened the phone calls.
The programme was billed as being a reaction to the case of a Chinese medicine practitioner who poisoned a patient, and to the publication of the report of Science and Technology Select Committee which damned homeopathy.
The programme can be heard here (at you own risk of bursting a blood vessel) Download mp3 file (43.6 Mb)
The major mistake was that the only "expert" on the programme was Michael McIntyre who is chair of the European Herbal & Traditional Medicine Practitioners Association. McIntyre is a well known advocate of alternative medicine, who constantly fudges the need for proper evidence. He is very keen to increase the respectability of herbalists (like all alternative practitioners, he is desperate to be accepted as a real doctor). In fact McIntyre doesn’t even represent all herbalists. . He failed to mention, and the presenter apparently didn’t know, that 2553 herbalists (as of 24 Feb) signed a petition that opposes the sort of pseudo-regulation the McIntyre wants so desperately.
"We the undersigned strongly object to the Government’s proposals to statutorily regulate herbalists and change section 12(1) of the 1968 Medicines Act."
Not to mention this was a serious error on the part of the researchers for this programme.
This was a programme about alternative medicine in which the ONLY expert was a notorious alternative medicine advocate. It was one of the most highly biassed programmes I have ever heard from the BBC. McIntyre most certainly does not represent the views of science or medicine, as shown, for example, by the submission from Sense About Science, the Academy of Medical Royal Colleges, the Institute of Biomedical Science, the Medical Research Society, the Medical Schools Council, the Physiological Society and the Royal College of Pathologists. The opinion of these not insubstantial people was not mentioned anywhere in the programme.
Here is a summary of the main points in the programme. It shows the bias very clearly. Furthermore the people who selected the phone calls seemed to pick almost all people who advocated alternative medicine.
(1) A lengthy anecdote relating a miraculous “cure” of fibromyalgia with homeopathy. No challenge or alternative interpretation was offered.
(2) A pharmacist (for heavens sake) who said she’d "seen results" from homeopathy and didn’t care whether or not it was placebo. She wasn’t challenged on the problem of lying about whether or not is placebo. We’ve had cause before to worry about the quality of advice given my pharmacists.
(3) Another long anecdote from a nurse (!) claiming to have been "cured" if fibroids by acupressure and cupping. No challenge or alternative interpretation was offered.
(4) Then some emails read out, mostly pro-quack. Only one claiming no effect (in asthma) but that was an anecdote too. Mostly more miracle cures.
(5) Michael McIntyre has the first of several long speeches. advocating more research. There was an advertisement for his web site "promotes best practice" (allegedly). He talks quite seriously about "reflexology" and so on, as though it were real subject (it isn’t; its "principles" are made-up fantasies).
He said. "We need more research in how complementary medicine works". Notice the inbuilt assumption that it does work. This is directly contradicted by the fact that the USA has spent over a billion dollars on CAM research and come up with not a single useful treatment. Why did the researchers and the presenter not know about this, and challenge McIntyre? Once again, the programme researchers seem to be Incompetent.
(7) A caller was mildly critical of fact the Norwich council can’t to anything about claims made by TCM shops (actually Trading Standards could, but generally don’t, but this wasn’t pointed out to the caller).
(8) A caller from Somerset makes the good point that alternative medicine becomes just medicine once it is shown to work.
(9) Michael McIntyre is challenged about evidence, and gives a lengthy speech about why proper RCTs aren’t necessary. They are necessary, but he isn’t challenged. Plus the usual excuse about lack of money for trials. What about that billion dollars?
(10) The Somerset caller says why restrict yourself to herbs? Good point, but no response.
(11) McIntyre gives another long speech in which he propagates the myth that the impurities in herbal medicines are in some way helpful, or synergistic, This is the only justification that herbalists have for giving impure drugs, but there isn’t the slightest evidence to think it’s true. McIntyre should have been challenged about this, but wasn’t.
At no point was McIntyre challenged about the danger of giving drugs (herbal or otherwise) in unknown doses, as herbalists do. He should have been challenged.
(12) Worker (unspecified) in NHS psychiatry says placebos were used to get patients off drugs. The presenter misses the point by asking if the placebos should be paid for by the NHS. The question he should have asked is about ethics of deceiving patients, but presenter did not do this.
(13) A blatant advertisement from a "health food store" in Barnoldswick. The owners are "pharmacy technicians" (since most pharmacists seem to have difficulties about evidence,
this can’t be regarded as a high qualification). They plug the supplements (almost all unnecessary, a few dangerous) that they sell.
(14) McIntyre again. Says something more or less sensible about drug interactions.
(15) By this time I’d emailed and got in a quick bit about the valuelessness of anecdotes, but was .cut short before I could talk about regulation.
(16) McIntyre defends anecdotes, predictably enough. This time the presenter did raise a good point about how anecdotes should be verified by proper tests but McIntyre again evades the main point that most herbs have not been properly tested, and isn’t challenged.
(17) More emails. A man who takes sage for sore throats. One says "of course homeopathic remedies are placebos but placebos work"; "homeopathy is an extraordinary system for industrialising
the placebo effect, but used by responsible practitioners it has a valuable place". Once again the ethics of deceiving patients with hocus pocus in order to elicit a placebo effect was not raised.
And one caller raised the usual red herring about dogs responding. This, yet again, went unchallenged. Why wasn’t it pointed out that it is the human who reports the state of the dog who has the placebo response?
(18) Then on to regulation. The researchers and presenter seemed to be quite unaware of the near-unanimous opinion of scientists and also of the Royal College of Physicians, that regulation in the form
proposed by the Pittilo report will be ineffective, and will do more to harm patients than to safeguard them. There is more than one way to regulate, and this uninformed intervention was especially
unwelcome at a time when the government is considering the question.
(19) Lady with MS said that acupuncture didn’t do her any good at all, but she didn’t like to tell the acupuncturist. But the obvious conclusions were not drawn.
(20) Presenter asks McIntyre leading question "it does work for some and not for others ". No hint there that the ones it "works for" might be the ones who were going to get better anyway. McIntyre himself actual pointed out that some forms of MS (‘relapsing’) undergo spontaneous remissions but of course fails to draw the obvious conclusion that any. He apparent effect of acupuncture could well have been a spontaneous remission. He went on to say (without any evidence) that "acupuncture may help". He relied on the standard line that "more research needed", but failed to mention the vast amount of research that has already been done which shows that acupuncture is probably little more than a theatrical placebo. See, for example, the Nordic Cochrane Centre review and Barker Bausell’s book, Snake Oil Science.
(21) An email points out that anecdotes are no substitute for proper tests. McIntyre then misquotes Sir Michael Rawlins(chair of NICE). He claimed, as most quacks do, that Rawlins had endorsed anecdotes as an acceptable form of evidence in his lecture. This is not what he said at all. In fact Rawlins was referring to treatments that had already passed RCTs and saying that they should be followed up in the wider population of patients to see if they lived up to their initial promise. This interpretation of his words was published in the BMJ after I’d checked it was correct with Rawlins himself.
In the same lengthy speech McIntyre claimed "There really isn’t any dummy acupuncture". This is absolutely untrue, but was not challenged. Huge ingenuity has gone into devising retractable ‘stage dagger’ acupuncture needles, as well as trials that use real needles inserted in the "wrong" positions. One of the most consistent findings in CAM research is that sham acupuncture is not distinguishable from "real" acupuncture. McIntyre, needless to say, didn’t mention this, He should have been challenged but wasn’t.
(21) Declan Naughton (Kingston University) advocates greater "regulation". "If we have trained herbal practitioners" it will make it safer for everyone. Thw revelation of what is actually taught on these degrees shows that, on the contrary, they endanger patients, He claims that use of purified antibiotics leads to problems with drug resistance. There isn’t the slightest reason to think that resistance has anything to do with purification, This was a red herring but went unchallenged. I notice that Naughton has published in Medical Hypotheses, a journal for wild speculations that is not peer-reviewed
(22) Donald Kerr a TCM practitioner, supports McIntyre in looking for statutory regulation. "like the GMC". He is not challenged on the extent to which real medicine and TCM have a sound basis. Like most alternative medicine advocates, he goes for the usual diversionary tactic of criticising western medicine which he refers to as "prescriptive medicines" [sic]
(23) London herbalist Michael Simmons. His web site claims that "Medical Herbalists are trained in the same diagnostic skills as orthodox doctors b". This is simply not true, The fact that herbalists claim it is true mereyl shows how they endanger patients.
(24) Marc Seale, chair of the Health Professions Council (HPC) now appears. he says one very interesting thing "things like false advertising would be dealt with by the regulator". He also acknowledged that there is a strong feeling among scientists and physicians that statutory regulation would give a "false sense of legitimacy " to the area. This latter point was entirely missed by the programme and that seems like another example of incompetent research. But Seale still doesn’t seem to understand the problem, as outlined here and in a joint submission from Sense About Science, the
Academy of Medical Royal Colleges, the Institute of Biomedical Science, the Medical Research Society, the Medical Schools Council, the Physiological Society and the Royal College of Pathologists. This submission opposed regulation of the sort favoured by McIntyre and Seale, but wasn’t even mentioned. Once again, all the speakers were on the same side.
(25. Back once again to McIntyre, who lamented that after ten years of trying, he still hadn’t achieved statutory regulations for herbalists (to the joy of 2500 herbalists), That is simply because they have not fulfilled the requirements for statutory regulation, as laid out in the House of Lords report (2000). That was not mentioned either. Agani the researchers appear not to have done their job properly.
(26) The presenter, Julian Worricker, refers to Prof. Edzard Ernst as a “divisive figure in this field”. That is a highly partial way to refer to the person who has done more than any other individual to bring together objectively the evidence for the effectiveness of alternative medicine. Ernst has every scientist and every informed person behind him.
(27) McIntyre again. He misrepresents Ernst’s views and misrepresents the strength of the evidence for the efficacy of herbal medicines, which are mostly untested.. But he is not challenged.
McIntyre goes on to misrepresent the BMJ Clinical Evidence paper which, he says, shows that 46% of all treatments are not proven to be effective. It is hard to be believe that McIntyre is really unaware that a large proportion of those that were not shown to be effective are CAM treatments, herbal medicine and the like. Professor John Garrow has pointed this out (see, also Healthwatch)
“It is true they chortle, but they have got their facts wrong. The 46% of treatments which are not proven to be effective is 46% of all treatments for 240 common conditions – and very few are used in the NHS. The great majority are treatments used by alternative practitioners. “
If McIntyre was not aware of this he should have been, If he was aware of it he was being less than honest. In any case the programme’s researchers should have been aware of it and McIntyrere should have been challenged. He wasn’t.
(28) A bizarre phone call from someone who seems to think that real medicines are not labelled with their ingredients
(29) Seale is asked if alternative medicine can be regulated like real medicine He says they’ll check degrees. If the checking is done properly, he’ll find endless dangerous made-up material like that revealed here. No degrees on TCM would pass and the whole edifice would collapse.
(30) Another presenter says "it all depends on peoples’ experiences which side they are on".. No! That is simply not true. Well it may have been be true of the phone callers, but is both misleading and untrue in general, The divide is actually between those who are aware of, and care about, evidence and those who do not. Some people actually take the questions seriously, but this comment reduced the discussion to the level of the life style section in a downmarket women’s magazine. One expects more of the BBC.
(31) McIntyre pleads that herbal medicines must be all right because they are used widely on continental Europe. This non sequiter went unchallenged.
(32) Seale says we must wait for Department of Health consultation on Pittilo recommendations. Quite right. For the sake of patient safety, one must hope that the Department of Health will listen to the evidence, and not implement them, despite McIntyre’s success in putting one side of the story on this programme.
(33) McIntyre laments the fact that Europe is bringing in some very sensible regulations about herbal medicine. Again he had free rein to air the views of some (not all) herbalists, with nobody there to support these sensible measures.
(2) Guilty plea in Chinese herbal ‘cancer’ case
This BBC web page gave a very unbalanced account of the case for and against statutory regulation< of traditional Chinese medicine. It simply echoed the (uninformed) view of the judge that "more regulation is necessary" but it was apparently quite unaware that the form of this regulation is at present under consideration by the Department of Health.
The vast majority of scientific and medical opinion is against the particular form of statutory regulation recommended by the Pittilo steering group, and the author of this anonymous report should have been aware of that. Why was there no reference to the submission from Sense About Science, the Academy of Medical Royal Colleges, the Institute of Biomedical Science, the Medical Research Society, the Medical Schools Council, the Physiological Society and the Royal College of Pathologists? These are bodies whose views should not have been ignored, as also the individual submissions here and here. It may be acceptable for a judge to be unaware of this powerful body of opinion. It is not acceptable for BBC reporters to ignorant of it.
The web page does now contain a short statement from Sense about Science which goes a small way to redress the imbalance, That was inserted only after a phone call to the BBC from a member of parliament.
(3) Woman claims that homeopathy cured her cancer
On February 23rd 2010m the BBC showed a an utterly irresponsible item. A homeopath, Gemma Hoefkens, claimed to have been cured of cancer by taking homeopathic sugar pills. There was nobody to point out the utter impossibility of this claim, just some not-very-probing questions fromt the presenter.
Hoefkens promoted her own web site during the interview. It is illegal under the Cancer ACt 1939 to claim to be able to cure cancer and this video must come very close to breaking that law. Some interesting inconsistencies in Hoefken’s account have been pointed out on the Ministry of Truth web site . This was a new low point in science reporting.
Follow-up
This complaint has been sent to the BBC. But the Ofcome web site says
“However, we cannot consider complaints about accuracy in BBC TV and radio news or complaints about impartiality in BBC TV and radio programmes. These complaints have to be dealt with by the BBC.”
This seems to preclude any independent outside adjudication. Not good.
Mark Henderson wrote a nice piece about impartiality in The Times (Feb 4 2010), “Science Matters: The BBC’s balancing act“. He expresses views that are, in many ways, similar to mine.
Yes, it’s that most boring of non-medicine topics, homeopathy, again. At lunchtime on Thursday I got a call from a Times journallst, Fay Schopen, to ask if I could do 500 words on the Science and Technology Committee’s Evidence Check report on homeopathy. Bang goes another evening. The (im)balance was provided by Sara Eames, President of the Faculty of Homeopathy. As always the media insist on treating the matter as though it were an even argument. It’s not. The version I bashed out was three times the length they wanted, and it was skilfully pruned to length by Fay Schopen for the published version. Here is the original. longer, version, for what it’s worth.
Should the NHS fund homeopathy?
|
|
The problem with parliament is that there aren’t enough doctors in the House. Or at least there are too many people who seem not to be able to make a critical distinction between what you’d like to be true and what actually is true (no, I’m not talking about Iraq but about something far less important). Perhaps the prime example is David Tredinnick (Cons. Bosworth) who claimed £700 on expenses for his efforts to link astrology and alternative medicine.
Luckily there are a few MPs who are not convinced that healthcare depends on the phase of the moon, and most of them are on the parliamentary Science and Technology Committee (STC). That committee has been conducting ‘evidence checks’ in an effort to find out the extent to which government policy is based on good evidence. Last Monday they published Evidence Check 2: Homeopathy. The report restores ones faith in reason. It concluded that there is no reason to think homeopathic pills have more effect than a placebo, therefore they should not be paid for by the NHS, and neither was more research justified. The report also criticised the Medicines and Health Regulatory Authority (MHRA) for allowing misleading labelling of homeopathic pills, and the Department of Health for failing the take notice of evidence.
Let’s get one thing straight. Homeopathy is very simple indeed. The medicine (in dilutions beyond 12C) contains no medicine. Zero, zilch, nothing. That’s why it is a placebo. Arnica 30C contains not a single molecule of Arnica. It is like selling strawberry jam that has never seen a strawberry. Yet Trading Standards officers can do nothing about this gross mislabelling because loopholes in the law allow advocates of magic medicine to get away with it. It also involves the preposterous idea that the more you dilute a remedy the stronger it gets. If you want to get drunk quickly, put a drop of whisky in the Atlantic Ocean and take a drop. It is nothing sort of surreal that the matter is still being discussed after 200 years.
How did these absurd ideas ever take hold? Around 1800, when homeopathy started, conventional medicine barely existed, and giving nothing was better than being bled and poisoned. Bleeding patients had been standard medicine for hundreds of years in 1800 despite the fact that it killed people. It went on so long because it depended on anecdotes, clinical authority and wishful thinking. These are still the forms of evidence favoured by homeopaths, but real medicine has changed entirely now whereas homeopathy has remained stuck in 1800.
The problem is that homeopaths routinely misrepresent the evidence (if they didn’t they’d be out of business). The report says
”We regret that advocates of homeopathy, including in their submissions to our inquiry, choose to rely on, and promulgate, selective approaches to the treatment of the evidence base”.
The Society of Homeopaths has the nerve to offer you “An overview of positive homeopathy research”. They quite blatantly omit the very much stronger negative evidence. The only word for that is dishonesty.
A favourite with homeopaths is a 2005 study in which 6544 consecutive patients were asked how they felt after homeopathic treatment and 50% said they felt better or much better. That seems a surprisingly small proportion given that most of them would have been treated for minor self-limiting conditions, but we’ll never know because there was no comparison group at all. As evidence, this is utterly worthless,
Two other defences are commonly offered by homeopaths. One is patient choice. The other is that it doesn’t really matter if it’s a placebo if it makes you happy. Choice is fine as long as it’s informed choice. If the homeopath said “these pills contain nothing, but you might feel better after taking them anyway”, that would be fine. But homeopaths never say that. In any case to deceive the patient into thinking they are being offered real medicine when they are not poses deep ethical problems, and the Department of Health has refused to grasp that nettle. You might as well say that Chanel No 5 should be available on the NHS because it makes some people feel better. At the moment we are in the absurd position in which a doctor is not supposed to give placebo knowingly and honestly, but can refer patient to a homeopath for a dishonest placebo. The fact that the homeopath may genuinely believe in the magic is not a sufficient excuse.
If homeopaths limited themselves to minor self-limiting conditions, they wouldn’t do too much harm. But non-medical homeopaths (the vast majority, in the Society of Homeopaths) mostly have no idea of their limitations. They believe they can prevent and treat treat malaria, AIDS, cholera, yellow fever, even cancer.. At this point homeopathy ceases to be a harmless joke but becomes more like culpable homicide.
Recently two homeopaths in Australia were jailed for manslaughter after their own daughter died for want of proper treatment. That is the sort of thing that happens you put your faith in magic medicine,
Homeopathy is on a par with talking to trees. No decent health service should pay for it.
Follow-up
Goldacre has lovely piece in the Guardian.
Homeopathy doesn’t work. But are the claims for other medicines any better?
Drug ads that don’t back up their claims show how dumb doctors can be about evidence and how lax regulation has become
After the Commons science and technology committee report this week, and the stupidity of “we bring you both sides” media coverage, you are bored with homeopathy. So am I, but it gives a simple window into the wider disasters in medicine.
He sounds as bored with homeopathy as I am. He points out that while 100% of claims made by homeopaths’ advertisements are untrue, it is also the case that 30 – 60% of advertisements by Big Pharma can’t be justified by evidence. Once again we see the similarity between the alternative industry and the regular industry (though the former still comes out worse).
Michael Grayer (2 march 2010) , at nontoxic.org.uk has some trenchant comments about what the mainstream media call “balance”. What constitutes balanced coverage worries me too, and gave rise to a complaint to the BBC recently.
What follows is mostly from the press release for the report of the Science and Technology Select Committee’s report on homeopathy.
Comments on their hearings can be found in Comedy gold in parliament and tragedy from Prince of Wales: editorial in British Medical Journal (Although published before Christmas, the comments on this editorial are still going strong in the BMJ).
It seems that the attempts of the British Homeopathic Association to misrepresent the evidence (as documented by Martin Robbins in the Guardian) were not sufficient to fool the MPs.
Committee chairman. Phil; Willis, said
"We were seeking to determine whether the Government’s policies on homeopathy are evidence based on current evidence. They are not."
The NHS As well as recommending, as expected, that NHS funding of homeopathy should end. the report also recommends that no more money should be spent on clinical trials of homeoapthy. The evidence is in and it doesn’t work
The MHRA The Medicines and Health Regulatory Authority (the MHRA) came in for strong criticism when it allowed registering of homeopathic products, and allowed highly misleading labelling of them (see for example, The MHRA breaks its founding principle: it is an intellectual disgrace, and The MHRA loses the plot, and Learned Societies speak out against CAM, and the MHRA). During the committee’s hearings, the CEO of the MHRA, Kent Woods, seemed to say that the labelling of Arnica 30C had been tested to ensure that it did not mislead the public. However evidence subsequently submitted by the MHRA showed that this was not the case. This, rightly. elicited strong criticism in the report
"The MHRA’s user-testing of the label for Arnica Montana 30C—the only product currently licensed under the NRS—was poorly designed, with some parts of the test little more than a superficial comprehension test of the label and other parts actively misleading participants to believe that the product contains an active ingredient.”
With scientific papers it is not acceptable to cut and paste the press release, but for a report of this sort, it summarises the main points succinctly.
The summary of the report
In a report published today, the Science and Technology Committee concludes that the NHS should cease funding homeopathy. It also concludes that the Medicines and Healthcare products Regulatory Agency (MHRA) should not allow homeopathic product labels to make medical claims without evidence of efficacy. As they are not medicines, homeopathic products should no longer be licensed by the MHRA.
The Committee carried out an evidence check to test if the Government’s policies on homeopathy were based on sound evidence. The Committee found a mismatch between the evidence and policy. While the Government acknowledges there is no evidence that homeopathy works beyond the placebo effect (where a patient gets better because of their belief in the treatment), it does not intend to change or review its policies on NHS funding of homeopathy.
The Committee concurred with the Government that the evidence base shows that homeopathy is not efficacious (that is, it does not work beyond the placebo effect) and that explanations for why homeopathy would work are scientifically implausible.
The Committee concluded—given that the existing scientific literature showed no good evidence of efficacy—that further clinical trials of homeopathy could not be justified.
In the Committee’s view, homeopathy is a placebo treatment and the Government should have a policy on prescribing placebos. The Government is reluctant to address the appropriateness and ethics of prescribing placebos to patients, which usually relies on some degree of patient deception. Prescribing of placebos is not consistent with informed patient choice—which the Government claims is very important—as it means patients do not have all the information needed to make choice meaningful.
Beyond ethical issues and the integrity of the doctor-patient relationship, prescribing pure placebos is bad medicine. Their effect is unreliable and unpredictable and cannot form the sole basis of any treatment on the NHS.
The report also examines the MHRA licensing regime for homeopathic products. The Committee is particularly concerned over the introduction of the National Rules Scheme (NRS) in 2006, as it allows medical indications on the basis of study reports, literature and homeopathic provings and not on the basis of randomised controlled trials (RCTs) – the normal requirement for medicines that make medical claims.
The MHRA’s user-testing of the label for Arnica Montana 30C—the only product currently licensed under the NRS—was poorly designed, with some parts of the test little more than a superficial comprehension test of the label and other parts actively misleading participants to believe that the product contains an active ingredient.
The product labelling for homeopathic products under all current licensing schemes fails to inform the public that homeopathic products are sugar pills containing no active ingredients. The licensing regimes and deficient labelling lend a spurious medical legitimacy to homeopathic products.
The Chairman of the Committee, Phil Willis MP, said:
“This was a challenging inquiry which provoked strong reactions. We were seeking to determine whether the Government’s policies on homeopathy are evidence based on current evidence. They are not.
“It sets an unfortunate precedent for the Department of Health to consider that the existence of a community which believes that homeopathy works is ‘evidence’ enough to continue spending public money on it. This also sends out a confused message, and has potentially harmful consequences. We await the Government’s response to our report with interest.”
Follow-up
A lot of people gave written about the SciTech report. The report of the Parliamentary Select Committee appeared. Evidence check homeopathy damned the policy of both the Department of Health and of the MHRA. The main job, apart from a few talk shows, was a visit to the BBC News Channel for an interview about it. Here it is. The comment about Chanel Number 5 seemed to go down well on Twitter.
My ,main
|
I had never intended to write about climate. It is too far from the things I know about. But recent events have unleashed a Palin-esque torrent of comments from people who clearly know even less about it than I do. In any case, it provides a good context to think about trust in science, |
 Earthrise from moon. (click to enlarge) |
My interest in it, apart from little matters like the future of the planet, lies in the reputation of science and scientists.
I have been going on for years now about the lack of trust in science, and the extent to which it is a self-inflicted problem. The latest reactions to the developments at the University of East Anglia and the IPCC may show the nature of the problem with dreadful clarity,
Many of us came into science because, apart from the sheer beauty of nature, it seemed like one of the few honest ways of earning a living. Most scientists that I know still think like that, but recent
events invite some reexamination of honesty in science.
How dishonest is science?
The first thing to say is that I have never come across anything in my own field that would qualify as fraud, or even dishonest. I did once have a visit from a rather distressed postdoc (not in my area of work) who felt pressurised by her boss into putting an interpretation on her work that she did not agree with. In the end, the bit of work in question was left out of the paper. That could be held to be dishonest, in that the omission wasn’t mentioned, but it could also be held that the omitted result was too ambiguous to contribute much to the paper. It was just short of the point where I’d have felt compelled to do something about it. But only just. That is about the worst thing I’ve encountered in a lifetime.
There is, of course, an enormous difference between being wrong and being dishonest. Any research that is worth doing has an outcome that can’t be predicted before the work is done. At best, one can hope for an approximation to the truth. Mistakes in observations, analysis or interpretation will sometimmes mean the announced result is completely wrong, with no trace of dishonesty being involved. But when that happens, others soon fiind the mistake. It is that self-correcting characteristic of science that keeps it honest in the long run.
Of course there have been occasional cases of outright fraud, simple
falsification or fabrication of data. How often it occurs is not really known. There is a recent analysis in PLoS One, about verified cases of misconduct in the USA suggested that 1 in 100,000 scientists per year are to blame, but other ways of counting give larger numbers. For example, if asked around 2 in 100 scientists claim to be aware of misconduct by someone else., The numbers aren’t huge but they are much bigger than they should be.
It isn’t perhaps surprising that the Fanelli study found misconduct was most frequent in “medical (including clinical and pharmacological) research studies”, which are often funded by the pharmaceutical industry, Basic biomedical research and other subjects were better, though sadly that could be only because they are less often offered money.
What gives rise to dishonesty?
It seems obvious that one motive is money, as suggested by the worst rates of misconduct being found in the clinical pharmacological studies, It is well known that studies funded by industry are more likely to produce results that favour the product than those funded in other ways.
The other reason is presumably the human desire to win fame, promotion and to get grants.
It is no excuse, but it is perhaps a reason for misconduct that the pressure to publish and produce results is now enormous in academia. Even in good universities people are judged by the numbers (rather than the quality) of papers they produce and by what journal they happen to be published in. Contrary to public perception, even quite senior people have no guarantee that they can’t be fired, and life for postdoctoral fellows, who do a large fraction of experimental research, is harsh to the point of cruelty. They exist on a series of short term contracts, they work exceedigly hard and have poor prospects of getting a secure job. In conditions like that, the only surprising thing is that there is so little dishonesty.
The pressure to publish in particular journals is particularly invidious because it is known that the number of citations that a paper gets (itself a fallible measure of quality) is independent of the journal in which it appears. Bibliometrists are the curse of our age. (See, for example Challenging the tyranny of impact factors, 2003; and How to get good science, 2007 or its web version; and Peter Lawrence’s article, The mismeasurement of science)
The enormous competitive pressure under which academics work is imposed by vice-chancellors, research councils and other senior people who should know better, It is a self-inflicted wound.
In other words, the authorities provide a strong incentive to do poor, over-hurried and occasionally dishonest science. Perhaps the surprising thing in the circumstances is that there is so little outright fabrication. The very measures that have the aim of improving science actually have just the opposite effect. That is what happens when science is run by people who don’t do it.
For an idea of what life is like in science now, try Peter Lawrence’s Real Lives and White Lies in the Funding of Scientific Research. Or, for someone at the other end of their career, Jennifer Rohn’s account on Nature blogs.
Given the high degree of insecurity for young researchers, compounded by well-intentioned but vacuous “training” from daft Robert’s’ "training courses", or the dismaly ineffective Concordat, the only surprise is that so many people remain honest and devoted to good science. Nothing raises the ire of hard-pressed scientists more than the constant emails form HR trying to force people to go to gobbledygook courses on "wellbeing". Times Higher Education recently did a piece on "Get happy", The comments are worth reading.
So what about climate change?
Out of thousands of pages in the IPCC reports, a single mistake was found, On page 493 of the IPCC’s second 1000-page Working Group report on “Impacts, Adaptation and Vulnerability” (WGII) it was said that Himalayan glaciers were “very likely” to disappear by 2035. Glaciers are melting but that date can’t be justified. This single mistake has been blown out of all proportion. Furthermore it is important to notice that the mistake was found by scientists, not by ‘sceptics’. It is a good example of the self-correcting nature of science. Nevertheless this single mistake has provoked something close to hysteria among those who want to deny that something needs to be done.
On the other hand, the hacked emails from the University of East Anglia (UEA) look bad. It simply isn’t possible at the moment to say whether they are as bad as they seem at first sight, We just don’t know whether anything of importance was concealed, but we should know.
One thing can be said with certainty, and that is that the reaction to their revelation by Dr Phil Jones, and by the vice-chancellor of the University of East Anglia, was nothing short of disastrous. Fred Pearce put it very well in Climate emails cannot destroy proof that humans are warming the planet
Most unforgivably of all, UEA refused to comply with requests under the Freedom of Information Act, and there is some reason to think that relevant material was deleted. The deputy information commissioner, Graham Smith, said: in a statement that
“The emails which are now public reveal that Mr Holland’s requests under the Freedom of Information Act were not dealt with as they should have been under the legislation. Section 77 of the Freedom of Information Act makes it an offence for public authorities to act so as to prevent intentionally the disclosure of requested information.”.
That seems to me to be a matter that requires the resignation of the vice-chancellor. On this matter, I think George Monbiot is spot on in his article “Climate change email scandal shames the university and requires resignations“.
There was a big feature about academic freedom in Times Higher Education recently. One of the problems was what happens to someone who brings their own university into disrepute. But when that term is used, it is always used about junior partners in the organisation (you know, professors and the like). It should apply equally to heads of communications and vice-chancellors who bring their own university into disrepute, whether the disrepute is brought about by failing to comply with the Freedom of Information Act, or by promoting courses in junk medicine.
In general, conspiracy theories are wrong. I’m not sure how much of the distortion of climate data results from surreptitious funding of opposition to doing anything by the fossil fuel industry. The Royal Society is an organisation that is not usually prone to conspiritorialist views. That means one must take it seriously the fact that in 2006, the Royal Society wrote to ExxonnMobil to ask them to stop funding climate denialist organisations. This is a bit like the way Big Pharma has been caught funding “user groups” that endorse their products. Some newspapers like to stir up controversies about things that aren’t very controversial. For example there is a good analysis of a recent Sunday Times piece here.
Of course it is often alleged that "quackbusters" are funded by Big Pharma, though in fact the amounts of money involved are far too small for Big Pharma to bother. Climate deniers too like to suggest that there is some sort of conspiracy, arranged between hundreds of labs in the world to conceal the fact that there is no such thing as warming. I guess that shows only that deniers know little about how science works. it is an exceedingly competitive business, and getting hundreds of labs to say the same thing would be like trying to herd cats.
If there is a problem, it is the other way round. Labs are in such intense competition with each other, that it lcan lead to undesirable levels of secrecy.
Blogs in which researches have a direct dialogue with the public are a big help. As always in the blogosphere, the problem is to find the reliable sources. Two excellent sites, in which scientists (not journalists or lobbyists) talk directly with the public are realclimate.org and Andrew Russell’s blog. The post on RealClimate, IPCC errors: facts and spin, is especially worth reading.
Total openness is the only cure
All the raw data and all emails have to be disclosed openly. Everything should be put on the web as soon as possible. By appearing to go to ground, UEA has made enormous problems for itself and for the rest of the world. Some people object to total openness on the grounds that the other side tells lies. In the case of climate change (and in the case of junk medicine too) that is undoubtedly true. The opponents are ruthlessly dishonest about facts. The only way to counter that is by being ruthlessly and visibly honest about what you know, and why.
The UK’s Meteorological Office has, to its great credit, put raw data on line. That policy has already paid off, because a science blogger found a mistake in the way that some Australian data had been incorporated into forecasts. The Met Office thanked him and corrected the mistake. In fact the error makes no substantial difference to the warming trend, but the principle is just great. The more people who can check analyses and eliminate slip-ups the better.
Putting raw data on the web is an idea that has been gathering force for a while, in all areas of work, not just climate change. In my own are (stochastic properties of single ion channel molecules) our analysis programs have always been available on the web, free to anyone who wants them, despite the large amount of work that has gone into them. And we run a course. almost free, on the theory that underlies our analyses. Within the last couple of months we have been discussion ways of making public all our raw data (in any case, we would always have sent it to anyone who asked). Digitised single channel records are big files (around 100 Mb) and it is only recently that the web has been able to deal with such large amounts of raw data. There are also problems of how to format data so other people can read it, The way we are all heading is clear, and the fact that some people in climate science appeared to be hiding raw data is a disgrace.
Public relations is not the cure
,
It is not uncommon to read that science needs better PR. That is precisely what is not needed. PR exists to put only one side of the story. That makes it an essentially dishonest occupation. Its aims are the very opposite of those of science. The public aren’t stupid: often they recognise when they are getting half the story.
It is particularly unfortunate that many universities have developed departments with names like "corporate communications". Externally they are seen as giving information about science, and indeed some of the things they do are successful public engagement in science. Only too often, though, it is made clear internally that an important aim of these departments is to improve the image of the university.
But you have to choose. You can engage the public in science or you can be a PR image-builder. You can’t be both.
The matter came to a head in 2008 when, according to a report in Times Higher Education, the University of Nottingham issued a memo that defined public engagement as: “The range of activities of which the primary functions are to raise awareness of the university’s capabilities, expertise and profile to those not already engaged with the institution”.
The mainstream media and political blogs
The biggest problem of all with climate change is that it has become more about politics than about facts. It has become an essential credential for any conservative to deny that climate is changing. It is part of their public image, and most conservatives neither know nor care about evidence. Like Sarah Palin, they just know. In the USA especially, the argument is not really about climate at all. It is really about discrediting Barack Obama -a sort of swift-boat treatment that uses whatever lies are needed.
Just as with the great MMR fiasco and the promotion of its false link to autism, reports in newspapers and blogs must bear much of the blame for failing to inform readers of the actual underlying facts and, just as important, the uncertainties. Of course some papers have done a pretty good job, particularly the Guardian and the Independent in the UK, and the New York Times.. The political blogs, by and large, haven’t. The Huffington Post has made little effort (and publishes some appalling nonsense about medicine too).
The problem with political blogs and tabloid newspapers is that they are much more interested in sensation and circulation than they are in giving accurate news and information. Take, for example, the Guido Fawkes blog. To be fair, the blog itself says "The primary motivation for the creation of the blog was purely to make mischief at the expense of politicians and for the author’s own self-gratification. Its writer", so you know not to expect much, Paul Staines, was at the Westminster Skeptics event, Does Political Blogging Make a Difference? He makes no pretence of taking the news seriously, which, I guess, is why I don’t read his blog. After the talks I asked why his blog did little about climate change. His answer was "where are your sandals?". On the way home I tweeted, from a very overcrowded train (most trains from Euston being cancelled that night),
"On way home from #sitp political blogging. Learned that Guido serious about nothing but Guido. Narcissist not journalist."
At least one other person there agreed (thanks, Dave Cole).
It was good to hear Sunny Hundall of Liberal Conspiracy (the only one I read), but I found myself agreeing mostly with the chair, Nick Cohen. It would be a tragedy if the great national and local papers were to vanish. Guido Fawkes and Huffington Post are not remotely like proper newspapers.
Specialist blogs like this one are fine if you are interested in the topics we write about, but we don’t begin to supplant proper newspapers. Bloggers can and do occasionally get good stories. Those that are written by scientists can analyse more critically than most journalists have either the knowledge or the time to do. Bur they don’t come close to supplanting the detailed reporting in good newspapers of local events, what happens in law courts or in parliament. That’s why it is vital to buy newspapers, not just read them free on the web.
Follow-up
James Hayton, who is in nanoscience has posted his thoughts obout trust in science on his blog. I discovered this via Twitter (@James_Hayton). He also posted a beautiful clip from the Ascent of Man, in which Jacob Bronowski speaks, from Auschwitz, of the consequences of irrational dogma. I’m old enough to remember Bronowski on a 1950s radio programme, the Brains Trust, though James Hayton clearly isn’t. Now I enjoy equally his daughter, Lisa Jardine‘s talks about science and history.
1 March 2010. Phil Jones, and the vice-chancellor of the University of East Anglia, appeared before a parliamentary committee. I found their responses to questions very disappointing. The evidence submitted by the Institute of Physics was strongly worded, but spot on.
“The CRU e-mails as published on the internet provide prima facie evidence of determined and co-ordinated refusals to comply with honourable scientific traditions and freedom of information law. The principle that scientists should be willing to expose their ideas and results to independent testing and replication by others, which requires the open exchange of data, procedures and materials, is vital.”
7 March 2010. Thanks to some kind remarks from Michael Kenward (see first comment). I sought wider coverage of this item in the mainstream media. Consequently, on Thursday 4 March, a much shortened version of this article appeared on the Guardian environment site. That piece has accumulated so far, 230 comments. The discussion of it has spread to the two blogs that I recommended, Andy Russell’s blog and RealClimate.org, though it has been diverted onto the side-issue of the letter from the Institute of Physics. The seemingly innocent idea that total openness would increase trust has, to my real astonishment, resulted in hysterical accusations that I’m a crypto-denialist. The constant politically-motivated attacks on climate science seem to have induced a paranoid siege mentality in some of them. There is a real danger that such people will harm their own cause, and that would be tragic.
Every single request for information about course materials in quack medicine that I have ever sent has been turned down by universities,
It is hardly as important as as refusal of FoI requests to see climate change documents, but it does indicate that some vice-chancellors are not very interested in openness. This secretiveness is exactly the sort of thing that leads to lack of trust in universities and in science as a whole.
The one case that I have won took over three years and an Information Tribunal decision against the University of Central Lancashire (UCLAN) before I got anything.
UCLAN spent £80,307.95.(inc VAT at 17.5%) in legal expenses alone (plus heaven knows how much in staff time) to prevent us from seeing what was taught on their now defunct “BSc (Hons) homeopathy”. This does not seem to me to be good use of taxpayers’ money. A small sample of what was taught has already been posted (more to come). It is very obvious why the university wanted to keep it secret, and equally obvious that it is in the public interest that it should be seen.
UCLAN had dropped not only its homeopathy "degree" before the information was revealed, They also set up an internal inquiry into all the rest of their courses in magic medicine which ended with the dumping of all of them.
Well, not quite all, There was one left. An “MSc” in homeopathy by e-learning. Why this was allowed to continue after the findings of UCLAN’s internal review, heaven only knows. It is run by the same Kate Chatfield who ran the now defunct BSc. Having started to defend the reputation against the harm done to it by offering this sort of rubbish, I thought I should finish. So I asked for the contents of this course too. It is, after all, much the same title as the course that UCLAN had just been ordered to release. But no, this request too was met with a refusal
Worse still, the refusal was claimed under section 43(2) if the Freedom of Information Act 2000. That is the public interest defence, The very defence that was dismissed in scathing terms by the Information Tribunal less than two months ago,
To add insult to injury, UCLAN said that it would make available the contents of the 86 modules in the course under its publication scheme, at a cost of £20 per module, That comes to £1,720 for the course, Some freedom of information.
Because this was a new request, it now has to go through the process of an internal reviw of the decision before it can ne referred to the Information Commissioner. That will be requested, and since internal reviews have, so far, never changed the initial judgment. the appeal to the Information Commissioner should be submitted within the month. I have been promised that the Information Commissioner will deal with it much faster this time than the two years it took last time.
And a bit more unfreedom
Middlesex University
I first asked Middlesex for materials from their homeopathy course on 1 Oct 2008. These courses are validated by Middlesex university (MU) but actually run by the Centre for Homeopathic Education. Thw MU site barely mentions homeopathy and all I got was the usual excuse that the uninsersity did not possess the teaching materials. As usual, the validation had been done without without looking at what was actually being taught. The did send me the validation document though [download it] As usual, the validation document shows no sign at all of the fact that the usbject of the "BSc" is utter nonsense. One wonderful passage says
“. . . the Panel were assured that the Team are clearly producing practitioners but wanted to explore what makes these students graduates? The Team stated that the training reflects the professional standards that govern the programme and the graduateness is achieved through developing knowledge by being able to access sources and critically analyse these sources . . . “
Given that the most prominent characteristic of homeopaths (and other advocates of magic medicine) is total lack of critical ability, this is hilarious. If they had critical ability they wouldn’t be homeopaths. Hilarious is not quite the right word, It is tragic that nonsense like this can be found in an official university document.
Middlesex, though it doesn’t advertise homeopathy, does advertise degrees in Traditional Chinese Medicine, Herbal Medicine and Ayurveda. On 2nd February 2010 I asked for teaching materials from these courses. Guess what? The request was refused. In this case the exemptions under FOIA were not even invoked but I was told that "All these materials are presently available only in one format at the University – via a student-only accessed virtual learning environment. ". Seems that they can’t print out the bits that I asked for, The internal review has been requested, then we shall see what the Information Commissioner has to say.
Two other cases are at present being considered by the Information Commissioner (Scotland), after requests under the Scottish FoIA were refused. They are interesting cases because they bear on the decision, currently being considered by the government, about whether they should implement the recommendations of the execrable Pittilo report.
Napier University Edinburgh. The first was for teaching material form the herbal medicine course at Napier University Edinburgh. I notice that this course no longer appears in UCAS or on Napier’s own web site, so maybe the idea that its contents might be disclosed has been sufficient to make the university do the sensible thing.
Robert Gordon University Aberdeen The second request was for teaching material from the “Introduction to Homeopathy” course at the Robert Gordon University Aberdeen. The particular interest that attaches to this is that the vice-chancellor of Robert Gordon university is Michael Pittilo. The fact that he is willing to tolerate such a course in his own university seems to me to disqualify him from expressing any view on medical subjects.
Michael Pittilo, Crohn’s disease and Andrew Wakefield
Michael Pittilo has not been active in science for some time now, but Medline does show scientiifc publications for Pittilo RM, between 1979 anf 1998. Between 1989 and 1995 there are five papers published jointly with one Andrew Wakefield. These papers alleged a relationship between measles virus and Crohn’s disease. The papers were published before tha infamous 1998 paper by Wakefield in the Lancet (now retracted) that brought disgrace on Wakefield and probably caused unnecessary deaths.. The link between measles and Crohn’s disease is now equally disproved.
The subject has been reviewed by Korzenik (2005) in Past and Current Theories of Etiology of IBD. Toothpaste, Worms, and Refrigerators
“Wakefield et al proposed that Crohn’s results from a chronic infection of submucosal endothelium of the intestines with the measles virus [Crohn’s disease: pathogenesis and persistent measles virus infection. Wakefield AJ, Ekbom A, Dhillon AP, Pittilo RM, Pounder RE., Gastroenterology, 1995, 108(3):911-6]”
"This led to considerable media interest and< public concern over use of live measles vaccine as well as other vaccines. A number of researchers countered these claims, with other studies finding that titers to measles were not increased in Crohn’s patients, granulomas were not associated with endothelium 49 , measles were not in granulomas50 and the measles vaccine is not associated with an increased risk of Crohn’s disease51–55 "
This bit of history is not strictly relevant to the Pittilo report, but I do find quite puzzling how the government chooses people from whom it wishes to get advice about medical problems.
Follow-up
I notice that the Robert Gordon university bulletin has announced that
“Professor Mike Pittilo, Principal of the University, has been made an MBE in the New Year Honours list for services to healthcare”.
That is a reward for writing a very bad report that has not yet been implemented, and one hopes, for the sake of patients, will never be implemented. I do sometimes wonder about the bizarre honours system in the UK.
Postcript.
On 16th February, the death of Michael Pittilo was announced. He had been suffeing from cancer and was only 55 years old. I wouldn’t wish that fate on my worst enemy.
I don’t know about you, but I’m bored stiff with homeopathy. There are a lot more important things. Nevertheless, it remains a gross insult to reason, and there has been such enormous success in combating it over the last five years so, this is not the moment to stop.
|
Hats off to the Merseyside Skeptics Society. I admit that when I first heard about the 10:23 campaign, it seemed to be a bit of a gimmick, but in fact it turned out to be an enormous success., not just in the UK but also in Canada, Australia and New Zealand |

|
The campaign was focussed on Boots, the UK’s biggest pharmacy chain, In particular the fact that Boots sell homeopathic pills. and regularly gives appallingly bad advice about all forms of quackery that they stock.
I’ve been criticising Boots for years now, starting with Mis-education at Boots the Chemist in May 2006. was largely about homeopathy, but Boots’ quackery is not restricted to homeopathy, In November 2007, Don’t Trust Boots described Boots’ promotion of vitamin pills that were
advertised by Boots to increase your energy, and also the appallingly bad advice given by shop staff on this product.
In March 2008, Boots did it again, with a big promotion written up as Boots reaches new level of dishonesty with CoQ10 promotion. The strategy seems clear by now. Launch an enormous publicity effort, and rely on journalists to parrot the press release. Put mendacious advertisements in every newspaper. Eventually the advertisements are found to be inaccurate by the Advertising Standards Authority. Boots are told to stop using the advertisement, but suffer no penalty at all. By that time the advertising campaign is over anyway, and they can rely now on inaccurate advice from "Boots expert team"; face to face in the store, to continue the promotion in a way that evades all regulation.
Boots is deeply involved too in the great ‘detox’ scam, as recounted, for example, in “Detox”: nonsense for the gullible, along with the Prince of Wales. And, most recently, Lactium: more rubbish from Boots the Chemists. And a more serious problem.
The nauseating hypocrisy of Boots’ Corporate Social Responsibility statement beggars belief. The same stuff is repeated on the current Alliance Boots site.
“Trust – The essence of the way we do business. We are trusted because we deliver on our promises.”
You must be joking.
Who owns Boots?
Boots started in 1849 as a single shop in Nottingham. Within my lifetime, they were rather ethical pharmacies (my recollection is that they didn’t sell homeopathic pills). They were also an ethical pharmaceutical company. They developed ibuprofen, which was launched in 1969. But since then the company was involved in a complicated series of acquisitions. Now it is a supranational conglomerate with presence in 20 countries, and almost beyond the reach of the law. Boots’ executive chairman is Stefano Pessina, who, with private equity firm Kohlberg Kravis Roberts in a £11.1 billion deal last year, took the firm private in 2007. In 2008 they announced a 20% increase in profits, to £771 million In 2008 they moved their headquarters out of the UK, to Geneva, partly, it seems, so they can be closer to other giants of Big Pharma, and partly, no doubt, to put pressure on the UK government not to tax them too much, On the other hand, tax may not be a big consideration because, according to The Times, the ultimate owners of Boots are based in Gibralter
The disgraced head of HBOS, Andy Hornby, was appointed as chief executive of Alliance Boots in June 2009. Before playing his part in ruining the UK economy he used to work for grocery chain, Asda. I’d guess that he has limited interest in pharmacology.
The economics of such organisations are beyond most people. a bit like the two cow economics joke perhaps.
"VENTURE CAPITALISM – AN ICELANDIC CORPORATION
You have two cows.You sell three of them to your publicly listed company, using letters of credit opened by your brother-in-law at the bank, then execute a debt/equity swap with an associated general offer so that you get all four cows back, with a tax exemption for five cows. The milk rights of the six cows are transferred via an intermediary to a Cayman Island Company secretly owned by the majority shareholder who sells the rights to all seven cows back to your listed company. The annual report says the company owns eight cows, with an option on one more. You sell one cow to buy a new president of the United States, leaving you with nine cows. No balance sheet provided with the release. The public then buys your bull."
Clearly there is not the slightest chance of an organisation like this will have any sort of conscience about selling useless pills, The only way that they can be influenced is by public mockery of their outrageous behaviour. If the publicity harms their image enough they may decide to cut their losses, because it pays, not because it is right.
10:23 a great success
The campaign was a success because it got good coverage in the newspapers, radio and TV. Boots, rather like vice-chancellors, seems to be uninterested in reason or morals, but will certainly be sensitive about its public image, There is a partial list of coverage at the 10.23 site.
Laura Donnelly had a good account in the Telegraph, "Homeopathy: medicine that’s hard to swallow?". And Hadley Freeman in the Guardian showed that fashion journalists can spot nonsense too, in "Me and my homeopathic overdose. How I knocked back a bottle of homeopathic ‘medicine’ and lived to tell the tale"
The spoof published on the NewsArse site (despite the name, it is excellent) hit the nail on the head, because it uses exactly the naive sort of post ho ergo propter hoc argument that homoeopaths love.,
Homeopathy proven to work after overdosing protesters eventually fall asleep
Homeopathic practitioners are today claiming victory for the efficacy of their remedies, after a protest by the 10:23 group who overdosed on homeopathic sleeping pills, left each participant asleep within just 36 hours of taking the remedy.
Funniest of all though, was the bleating by homeopaths themselves. Try, for example, Homeopathy Heals. Like all the others it alleges a conspiracy by big Pharma: “it seems to be driven by those working for Pharma behind the scenes”. It seems to have escaped the attention of these conspiritorialists that the demonstration was aimed at Boots and Boots IS Big Pharma. The two are inextricably linked and both use the same tactics to increase sales.
My small contribution
Apart form contributing to Laura Donnelly’s piece in the Telegraph, "Homeopathy: medicine that’s hard to swallow?"., I had a few more calls.
Mary English, homeopath and astrologer
The most interesting was a talk show on Radio 5 live, where I was was pitted against a homeopath, Mary English [play the mp3 file, 4.4
Mb]. Having come across Mary English before, I was well-prepared to talk about her record not only in homeopathy, but also in astrology. The presenter didn’t give me time to raise these points but he did a pretty good job himself in asking her the relevant questions.
Mary English’s website is a delight. "Homeopathy and Astrology can heal you".
" If you eat a whole bottle of them it wouldn’t make any difference because it’s the dose that you have, not the quantity of the tablets"
"It’s the frequency of dose . . .because it’s vibrational medicine"
The host asked "what’s vibrational medicine?"
"it works with your bodies systems as opposed to against it"
No doubt Mary English is quite sincere, She just, like so many homeopaths, seems to be quite unaware that these words don’t mean anything at all. Just pure gobbeldygook.
Some of her claims are bizarre, even by the standards of homeopaths. She has researched the birth charts of Indigo Children, and written a book, "How to survive a Pisces" Her claim to homeopathic fame is that she has done "provings" of "remedies" including thunderstorm, and shipwreck and Stanton Drew Stone Circle, and Old Wardour Castle. Ahem, suddenly Arnica 30C sounds quite sane.
Less excusably, Mary English went on to claim that there is good evidence that homeopathy works. She just hasn’t read, or hasn’t understood the evidence. But since she earns her living as a homeopath
and astrologer, she hasn’t got much incentive to read the evidence. if she did, her income would dry up.
The presenter put directly to Mary English the recommendation of homeopathy for malaria prevention. "You wouldn’t condone that would you?". Quite disgracefully that question was avoided. She
changed the subject without answering the question. The quackometer’s classic post on The Gentle Art of Homeopathic Killing came to mind (see also here for links to full text)
Some herbal stuff
Herbal medicine rather than homeopathy was the topic of the other two weekend gigs. That arose from the Pittilo proposals for statutory regulation of herbalists and Chinese medicine.
The BBC TV interview, together with a herbalist, Rhona Edmonds, is now in YouTube. A Welsh member of the European parliament, Jill Evans (Plaid Cymru) , has been backing herbalists on the grounds that they are a “well-respected profession”. Oh yes? The Prince of Wales has also had support from another MEP. Mike Nattrass (UKIP). It seems that our fringe parties have even more trouble with science than the Labour and Conservative parties (and, tragically, that includes the Green party too).
There was also an early morning talk show interview on Sunday 31 January, against the same herbalist [play mp3 file] She claims "we treat all sorts of conditions",. Yes indeed, that’s the problem. "If we were recognised it would give the public even more confidence". And that is the problem too. They don’t deserve that confidence.
The analogy between alternative medicine and religion is often striking. Both involve blind faith, and both are characterised by tendency to split into sects that war with each other even more viciously than they war with unbelievers. All the discussions of herbalism ignore the fact that an enormous number of herbalists (2536 as of 4th February) have signed a petition opposing the idea of statutory regulation, even in the ineffective form that is being proposed.
The Prince of Wales declares war on . . . the Enlightenment
That was the headline of an article in The Times (February 4th, 2010). There can be no more high profile propagandist for every form of magic medicine than the Prince of Wales. Nothing seems to stretch his credulity. But even I was taken aback by his latest pronouncement. It seems he’s been called an enemy of the enlightenment (yes, by me among many others).
“I was accused once of being the enemy of the Enlightenment,” “I felt proud of that.”
“We cannot go on like this, just imagining that the principles of the Enlightenment still apply now. I don’t believe they do. But if you challenge people who hold the Enlightenment as the ultimate answer to everything, you do really upset them.”
So it seems he wants to return medicine not just to 1800, but to 1500, the dark ages. Can he really think that life in 1500 was some sort of utopia? Of course one suspects that his disapproval of the enlightenment is restricted to medical matters. He hasn’t been seen to reject other products of the enlightenment, like cars, aircraft, telephones, radio, TV and the internet.
I suspect that the Prince of Wales needs a history lesson.
Follow-up
Thanks to a colleague for pointing out an excellent sketch from the Newsjack show on BBC Radio 7, broadcast on 4th February 2009. [play mp3 file, 2.4 Mb]. I quote.
“Last weekend, people up and down rhe country engaged in a mass anti-homeopathy protest, swallowing whole bottles of remedies outside Boots.”
“It’s very easy to sneer at homeopathy but we at Newsjack believe it’s important to listen to both sides of the debate. So to put the case for homeopathy we have invited on a ridiculous charlatan who extorts money from innocent people while providing no services of any actual value.”
“Will you please welcome His Royal Highness, the Prince of Wales”
The purpose of this post is to reveal a few samples of things that are taught on a homeopathy ‘degree’ course. The course in question was the "BSc Hons homeopathy course at the University of Central Lancashire (UCLAN). Entry to this course was closed in 2008 and, after an internal review, UCLAN closed almost all of the rest of its courses in alternative medicine too. The university is to be commended for this .
The purpose of making public some of what used to be taught is not to embarrass UCLAN, which has already done the sensible thing, but to make it clear that the sort of thing taught on such courses is both absurd and dangerous, in the hope of discouraging other courses
|
.Three years after I first asked for teaching materials, the Information Commisioner ruled that all the reasons given for refusal were invalid, and they must be handed over. However UCLAN then appealed against the decision, so the appeal went to an Information Tribunal. That appeal was lost decisively and UCLAN was.obliged to provide the whole of the course material. On Christmas Eve I got five large box files, 13.7 kg of documents, or 30 pounds, in old money. |

|
Because these documents are copyright, I rely on the twin defences of fair quotation (only a tiny proportion is being quoted) and public interest. The Information Tribunal decided very firmly that it was in the public interest that it should be known what is taught on such courses, and that can be achieved if some of it is made public. Here are a few extracts.
Code of ethics
The students are given a copy of the code of ethics of the Society of Homeopaths. This is 25 pages long, but paragraph 48 is especially interesting.
48 Advertisements, stationery and name plates maintain a high standard of propriety and
integrity to enhance the reputation of homeopathy.
- Advertising shall not contain claims of superiority.
- No advertising may be used which expressly or implicitly claims to cure named diseases.
- Advertising shall not be false, fraudulent, misleading, deceptive, extravagant or sensational.
No mention though, of the fact that this code of ethics has been repeatedly breached by the Society of Homeopaths itself, on its own website. See, for example, here in 2007 and again in 2009. as well as Ernst’s article on this topic.
Anyone who has followed dialogues among homeopaths knows that "claims to cure named diseases" is the norm not the exception. The code of ethics is just a bad joke. And the (late) course at UCLAN was no exception. Take, for example, course HP3002, Therapeutic Homeopathy, module leader Jean Duckworth.
Homeopathic treatment of cancer
There was a lecture on HP3002 called "A Homeopathic Approach to Cancer (Ramakrishnan methodology [sic])".. Here are 10 slides from that lecture. It is illegal to claim to be able to cure cancer under the Cancer Act 1939. If a homeopath were to make claims like these in public they’d be open to prosecution, not to mention in breach of the SoH’s code of ethics. If cancer is not a "named disease", what is?
Specific treatments for a named disease are recommended.
What happened to treating the whole person? Now specific organs are being treated. The term "affinity", as used here, is of course sheer hocus pocus.
It is easy to forget when reading this that none of the “medicines” contain any medicine whatsoeever.
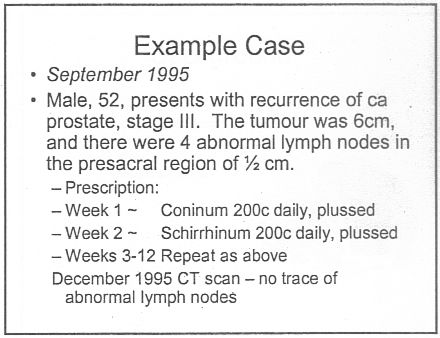
Notice that the term "remedy" is used throughout. Any reasonable person would interpret "remedy" to imply "cure", though no doubt a homeopath, if challenged, would claim that "remedy" carried no such implication. The last slide is typical of junk medicine: the personal testimonial, supplied with no detail whatsoever. Just an anecdote which is useless as evidence.
This lecture alone strikes me as a cruel (and possibly illegal) hoax perpetrated on desperate patients. Of course a true believer might get some solace from taking the sugar pills, but that is not sufficient justification.
The same course dealt with quite a lot of other "named diseases", autism, ADHD and coping with a heart attack. And, you are asked, did you think arnica is just a first aid remedy?
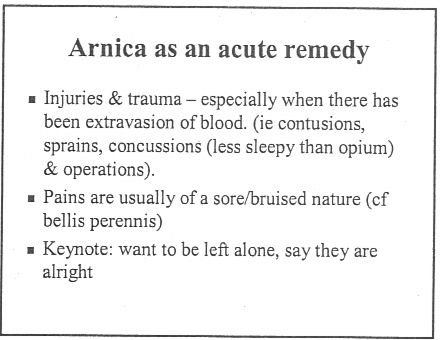
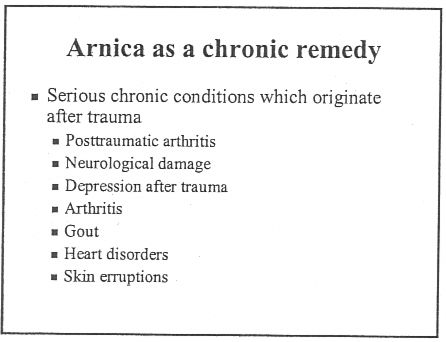
If that isn’t a list of "named diseases", what is? The code of ethics appears to be a total sham.
And of course never forget that the “arnica” doesn’t contain any arnica anyway. And if you don’t believe that you can read the words of Kate Chatfield, module leader on thie very course, as recorded in the minutes of evidence to the Select Committee on Science and Technology .
Q538 Lord Broers: I have a simple, technical question about homeopathy and drugs. Is it possible to distinguish between homeopathic drugs after they have been diluted? Is there any means of distinguishing one from the other?
Ms Chatfield: Only by the label.
You can read a lovely analysis of the views of Kate Chatfield by physicist A.P. Gaylard here.
Follow-up
The Daily Telegraph. January 8th 2009 Ian Douglas reported on this post: The workings of a BSc in homeopathy
The Lancashire Evening Post carried a big spread on January 15th, Professor seeks out the truth about ‘quackery’.
River’s Edge. News and thoughts from Preston, Lancashire reviewed the Lancashire Evening Post article on Saturday January 16th: Homeopathy at UCLAN, a degree in quackery.
The cost of trying to stop this material being revealed. UCLAN told me on 5 February 2010 that the legal costs alone were £80,307.94 (inc. VAT). That doesn’t include staff time and photocopying. I’m not convinced that this was a good way to spend taxpayers’ money.
Can’t resist another bit of straight plagiarism. In this week’s Times Higher Education, the inimitable Laurie Taylor wrote this.
|
Rock around the clock Professor Georgina Kunzite, the Head of our Department of Crystal Healing, has reacted strongly to the recent High Court ruling that the University of Central Lancashire must hand over teaching materials from its defunct homeopathy course to a campaigning sceptic. Speaking to our reporter, Keith Ponting (30), she said she had no intention of acceding to any similar request for materials from her own oversubscribed course in crystal therapy. Such a move, she argued, risked undermining the power of the crystals, which were notoriously wary of attempts to question their curative validity. She had initially been disconcerted by the court’s decision. “But since then I’ve taken to sleeping with a large lump of pink rhodochrosite crystal under my pillow. This does mildly disturb my partner, but it has certainly helped to rebalance my chakra.” |
Well well, where could he have got that idea?
There is no topic more widely discussed than what one should eat in order to stay healthy. And there are few topics where there evidence is so lacking in quality. This post isn’t about quackery, but about something much more important. it is about the real science (if it merits that description) behind dietary advice. I’m not an expert in nutrition, but I do know a bit about the nature of evidence. I’m continually astonished by the weakness of the evidence for some things that have become received truths, and nowhere is that more true than in nutrition.
|
The BMJ used my review of Gary Taube’s book, The Diet Delusion, to start off their new Round Table feature [full text link to BMJ]. The published version had some big cuts so I publish the original version here. Taubes was kind enough to send me a copy of the book after I’d mentioned his wonderful New York Times piece in my previous excursion into the murky world of diet and health, Diet and health. What can you believe: or does bacon kill you? |
|
The biggest omission in the BMJ version was Taubes’ own ten point summary of his conclusions (on page 454).
"“As I emerge from this research, though, certain conclusions seem inescapable to me, based on existing knowledge
- Dietary fat, whether saturated or not, is not a cause of obesity, heart disease, or any other chronic disease of civilization
- The problem is the carbohydrates in the diet, their effect on insulin secretion, and thus the hormonal regulation of homeostasis – the entire harmonic ensemble of the human body. The more easily digestible and refined the carbohydrates, the greater the effect on our health, weight, and well-being.
- Sugars – sucrose and high-fructose corn syrup specifically – are particularly harmful, probably because the combination of fructose and glucose simultaneously elevates insulin levels while overloading the liver with carbohydrates.
- Through their direct effect on insulin and blood sugar, refined carbohydrates, starches, and sugars are the dietary cause of coronary heart disease and diabetes. They are the most likely dietary causes of cancer, Alzheimer’s disease, and the other chronic diseases of civilization.
- Obesity is a disorder of excess fat accumulation, not overeating, and not sedentary behaviour.
- Consuming excess calories does not cause us to grow fatter, any more than it causes a child to grow taller. Expending more energy than we consume does not lead to long-term weight loss; it leads to hunger.
- Fattening and obesity are caused by an imbalance – a disequilibrium – in the hormonal regulation of adipose tissue and fat metabolism. Fat synthesis and storage exceed the mobilization of fat from the adipose tissue and its subsequent oxidation. We become leaner when the hormonal regulation of the fat tissue reverses this balance.
- Insulin is the primary regulator of fat storage. When insulin levels are elevated – either chronically or after a meal – we accumulate fat in our fat tissue. When insulin levels fall, we release fat from our fat tissue and use it for fuel.
- By stimulating insulin secretion, carbohydrates make us fat and ultimately cause obesity. The fewer carbohydrates we consume, the leaner we will be.
- By driving fat accumulation, carbohydrates also increase hunger and decrease the amount of energy we expend in metabolism and physical activity.”
It is on these bases that Taubes suggests that the increase in obesity is, in part, a consequence of the recommendation of a low fat, and hence high sugar diet.
|
The Diet Delusion [ pp 601] (published in the USA as Good Calories, Bad Calories) Gary Taubes 2008 There is no topic more widely discussed than what one should eat in order to stay healthy. And there are few topics where the evidence is so lacking in quality. It is also a topic that is besieged by gurus, cranks and supplement hucksters. You need to beware of misleading titles. Dietitians are good. Nutritionists are sometimes good. But titles like ‘nutritional therapist’ and ‘nutritional medicine’ are usually warning signs of alternative therapists and/or pill salespeople. Gary Taubes is a journalist, but he is quite an exceptional journalist. His account of the importance of randomisation for the establishment of causality is one of the best ever and it was published not in an academic journal, but in the New York Times [1]. His book, The Diet Delusion, is in the same mould. It is more complete and more scholarly than most professional scientists could manage. Not only does it cover the literature right back to Samuel Johnson, but it is also particularly good at unravelling what one might call the politics of science. And by politics I don’t mean the vast lobbying industry that has built up with the aim of selling you unnecessary supplements, but the politics of academia. Obesity sounds simple. If you are fat it is because you eat too much or exercise too little, right? Well no, it’s not as simple as that. For a start, it has been shown time and time again that low fat diets, and exercise, have small and temporary effects on weight. The problem with diet and health revolves round causality. The law of conservation of energy is an inevitable truth, but says nothing about causality. It could imply that you get fat because you eat too much, or equally the causal arrow could point the other way and “we eat more, move less and have less energy to expend because we are metabolically or hormonally driven to get fat”. The assumption that positive caloric balance is the cause of weight gain has predominated since the 1970s and “this simple misconception has led to a century of misguided obesity research”. At the heart of the problem is the paucity of randomised trials, which are the only way to establish causality. Those that there are have usually shown that diet does not matter as much as we are told. Taubes concludes
I think it can certainly be argued that the problem of causality has been greatly underestimated. We are warned constantly of the dangers of processed meat, on the basis of very unconvincing evidence [2]. This is one reason why we still know so little about the causes of obesity, diabetes and heart disease. For Taubes, a major villain was the US nutritionist Ancel Keys (1904 – 2004). His It is quite possible that there was rather more to be said for the Atkins diet than was apparent at the time. The fact that Atkins was not a university scientist, that his views were extreme and that he was so obviously out to make a lot of money from it, gave him all the appearance of being yet another profiteering diet guru. He was dismissed by the medical establishment as a quack. Taubes points out that conflict of interest cuts both ways. Atkins’ sternest critics at Harvard were funded by General Foods, Coca-Cola and the sugar industry. It adds up to a sorry story of a conflict of vested interests and scientific vanity. Taubes’ final judgement is harsh. He quotes Robert Merton’s description [4] of what science is, or should be.
He then comments
It took Taubes five years to write this book, and he has nothing to sell apart from his ideas. No wonder it is so much better than a scientist can produce. Such is the corruption of science by the cult of managerialism that no university would allow you to spend five years on a book [5]. I find all ten points in his summary convincing. But his most important conclusion is that you cannot have any certainty without randomised trials. The business of nutrition is greatly at fault for not having put more effort into organising randomised trials. Until they are done, we’ll never really know, and we shouldn’t pretend that we do. 1. Taubes G. Do we really know what makes us healthy? New York Times 2007 Sep 16.[full text link] [pdf file] 2. Colquhoun, D. (3 May 2009) Diet and health. What can you believe: or does bacon kill you?. 3. Greenberg, S.A.. 2009 How citation distortions create unfounded authority: analysis of a citation network. BMJ ;339:b2680 [pdf file]. 4. Merton, R. K. Behavior Patterns of Scientists . Leonardo, Vol.3 1970; 3(2):213-220. From Jstor [or pdf file] 5. Lawrence PA. The mismeasurement of science. Curr Biol 2007; 17(15):R583-R585.PM:17686424 [pdf file] [commentary] |
If length had allowed, there should certainly have been a reference here to Robert Lustig of UCSF. He is an academic nutritionist who supports the main thesis of Taubes’ book. See, for example, his 2005 review, Childhood obesity: behavioral aberration or biochemical drive? Reinterpreting the First Law of Thermodynamics [full
text link]. Lustig’s slide show, The Trouble with Fructose is available in the NIH web site.
There are a couple of other articles by Taubes that are well worth reading. The Scientist and the Stairmaster Why most of us believe that exercise makes us thinner—and why we’re wrong. Gary Taubes, in New York Magazine, and We can’t work it out, in the Guardian.
You can see Taubes in action on YouTube, for example in “on Cholesterol and Science Practices“, and “on Carbohydrates and Degenerative Diseases“. There is also a video of Taubes on medical grand rounds at Dartmouth-Hitchcock Medical Center in June 2009. You can see Robert Lustig on YouTube too: “Sugar: The Bitter Truth“.
Follow-up
22 December.2009, Unlike the serious questions dealt with in the Diet Delusion, this concerns merely another bit of the ubiquitous nutribollocks that crops up in the media, While writing this I was listening to the excellent early evening news programme, PM, run by Eddie Mair, when a diet-related topic came up, it was nonsense about how a cocktail made with vodka, cointreau, acai juice and pomegranate juice would not give you a hangover. I suppose it was meant as christmas fun but whenever I hear the words ‘antioxidant‘ or ‘superfood; I feel an email coming on. It seems that Eddie Mair liked the fact that the email contained the words ‘quack’ and ‘codswallop’ because the next thing I knew I was asked to give an interview on next day’s programme. The mp3 is here.


Snow on December 18th Roaring fire
Lindy contributes acute comments regularly here. She is also an accomplished musician. She has kindly allowed me to post here four of her re-written carols.
Adam lay ybounden | Hark the Herald | Holly and the Ivy | Merry Gentlemen
Adam lay ybounden
The Middle English dialect is not easy to follow. In fact Wikipedia reveals that it is oit even standard Middle English, but Macaronic English. The original words are reproduced in the right hand column. The original, sung by choir of King’s College Chapel, is on YouTube.
| Atoms lay y’bounden In primordial soup; Six billion years did pass A’fore they could regroup. For first had bin a big bang The universe was shook; Though through milennia For god it was mistook. Then particles of light did shine, ema- -nating from the sun. Out of soup arose archaea And so life was begun. Thanks be to the man This mystery did solve; Through him we celebrate how we Did from the bugs evolve. |
Adam lay ybounden, Bounden in a bond: Four thousand winter Thought he not too long. And all was for an apple, An appil that he took, As clerkè finden Written in their book. Ne had the apple taken been, The appil taken been, Ne had never our lady Abeen heavenè queen. Blessèd be the time That appil taken was, Therefore we moun singen, Deo gracias! . |
Hark the Herald Angels sing.
This version is for Simon Singh. If you haven’t yet signed the new peition, please do it here.
Mark this very dang’rous thing,
Story is of Simon Singh.
He got chiropractors riled,
“Sod it! We have been defiled!
Ployful all ye woosters rise,
Join us to defend our lies,
With us loudly please proclaim,
Subluxations are our game”
Christ, they all with one accord
Took young Simon off to court.
“We’ll put you before a judge,
Since we always bear a grudge
‘Gainst all those who say our modus
Operandi is all bogus;
Mark the words of justice Eady,
Gave his ruling oh so speedy.
Mark the case of Simon Singh
With support the web does ring.
Ditch draconian libel laws,
Without which they’d have no cause
To sue those who would speak freely,
Truth, opinion-and reason really
Should prevail o’er all such things,
Surely he his case must win.
The Holly and the Ivy
Dedicated to the Prince of Wales, certain vice-chancellors and other champions of the endarkenment.
The folly and the lies, see
How they’ve become full-blown;
The braying of th’quackti’tioner Roy-
Al, th’enlightenment has flown.
Refrain: For deriding all the data
(Such stunning stuff we hear)!
The displaying of such cherry pick-
-Ing, beats bringing in Chi square.
The folly hears no critics
It makes you quite struck dumb,
Just put a poison substance in,
And dilute to kingdom come.
For deriding all the data etc.
The folly so does blossom,
Beguiles you with its charm,
Just make some movements with your wrist
And it will do no harm.
For deriding all the data etc.
The folly’s given credence
If you are qualified
With a BSc in pseudosci-
-Ence, th’endarkenment is nigh!
For deriding all the data etc.
The folly bears a burden
Now it has fallen down;
F.O.I requests and publicity
Have giv’n D.C. the crown.
For deriding all the data etc.
The folly is so fickle,
How did they have the gall
To tell us how their remedies
Were here to treat us all?
For deriding all the data etc.
The folly and the lies, see
How they must surely fail
We’ll drink a toast to good evidence
And let real science prevail!
Alternative refrain:
Oh the rising of the Reiki,
Of acupuncture too,
All Rolfering* and Tuina-ish,
They all amount to woo.
*The names Rolf and Roger seem remarkably similar in some circumstances so I get a little confused.
Merry gentlemen.
Here is Lindy’s version of "god rest ye merry gentleman", composed in the wake of the admission by the Professional Standards director of Boots the Chemists that they sell homeopathic pills despite being aware of the fact that there is no reason to think they work.
I arrest you merry gentlemen,
Please kindly step this way.
For you are selling sugar pills
For which the people pay;
We’re from the Trading Standards and through courts we’ll find a way
To stop your profit-making ploy, Profiting ploy,
We’ll stop your profiteering ploy”!
The chemists calmly did defend
Themselves though they were riled;
“The people do demand these pills
Because they’re not defiled
With molecules (nor ‘owt at all), despite the claims so wild;
We’ll continue our profiteering ploy, Profiting ploy,
We’ll continue our profiteering ploy”.
So Trading Standards did respond
“We understand your aim
To make more money, though if you
Persist with bogus claim
To cure disease with sugar pills,
We’ll put you all to shame!
We are stopping your profiteering ploy, Profiting ploy,
We are stopping your profiteering ploy”.
“You breach the regulations by selling pills, you see,
Which claim to contain ‘aqua’ (dilute to 30C),
Or ‘dolphin song’ or ‘canine testes’ – even ‘ATP’!
So you’ll stop all this profiteering ploy, profiting ploy,
So you’ll stop all this profiteering ploy”.
The Dept of Health bangs on and on
About a patient’s choice,
But all good people must condemn
These lies with one great voice.
We dream of days when fibs are gone and we can all rejoice
‘Cos they’ve stopped all their profiteering ploy, Profiting ploy,
‘Cos they’ve stopped all their profiteering ploy
The Yuletide edition of the BMJ carries a lovely article by Jeffrey Aronson, Patent medicines and secret remedies. (BMJ 2009;339:b5415).
I was delighted to be asked to write an editorial about it, In fact it proved quite hard work, because the BMJ thought it improper to be too rude about the royal family, or about the possibility of Knight Starvation among senior medics. The compromise version that appeared in the BMJ is on line (full text link).
The changes were sufficient that it seems worth posting the original version (with links embedded for convenience).
The cuts are a bit ironic, since the whole point of the article is to point out the stifling political correctness that has gripped the BMA, the royal colleges, and the Department of Health when it comes to dealing with evidence-free medicine. It has become commonplace for people to worry about the future of the print media, The fact of the matter is you can often find a quicker. smarter amd blunter response to the news on blogs than you can find in the dead tree media. I doubt that the BMJ is in any danger of course. It has a good reputation for its attitude to improper drug company influence (a perpetual problem for clinical journals) as well as for clinical and science articles. It’s great to see its editor, Fiona Godlee, supporting the national campaign for reform of the libel laws (please sign it yourself).
The fact remains that when it comes to the particular problem of magic medicine, the action has not come from the BMA, the royal colleges, and certainly not from the Department of Health, It has come from what Goldacre called the “intrepid, ragged band of bloggers”. They are the ones who’ve done the investigative journalism, sent complaints and called baloney wherever they saw it. This article was meant to celebrate their collective efforts and to celebrate the fact that those efforts are beginning to percolate upwards to influence the powers that be.
It seems invidious to pick on one example, but if you want an example of beautiful and trenchant writing on one of the topics dealt with here, you’d be better off reading Andrew Lewis’s piece "Meddling Princes, Medical Regulation and Licenses to Kill” than anything in a print journal.
I was a bit disappointed by removal of the comment about the Prince of Wales. In fact I’m not particularly republican compared with many of my friends. The royal family is clearly good for the tourist industry and that’s important. Since Mrs Thatcher (and her successors) destroyed large swathes of manufacturing and put trust in the vapourware produced by dishonest and/or incompetent bankers, it isn’t obvious how the UK can stay afloat. If tourists will pay to see people driving in golden coaches, that’s fine. We need the money. What is absolutely NOT acceptable is for royals to interfere in the democratic political process. That is what the Prince of Wales does incessantly. No doubt he is well-meaning, but that is not sufficient. If I wanted to know the winner of the 2.30 at Newmarket, it might make sense to ask a royal. In medicine it makes no sense at all. But the quality of the advice is irrelevant anyway. The royal web site itself says “As a constitutional monarch, the Sovereign must remain politically neutral.”. Why does she not apply that rule to her son? Time to put him over your knee Ma’am?
Two of the major bits that were cut out are shown in bold, The many other changes are small.
BMJ editorial December 2009
Secret remedies: 100 years onTime to look again at the efficacy of remedies Jeffrey Aronson in his article [1] gives a fascinating insight into how the BMA, BMJ and politicians tried, a century ago, to put an end to the marketing of secret remedies. They didn’t have much success. The problems had not improved 40 years later when A.J. Clark published his book on patent medicines [2]. It is astounding to see how little has changed since then. He wrote, for example, “On the other hand the quack medicine vendor can pursue his advertising campaigns in the happy assurance that, whatever lies he tells, he need fear nothing from the interference of British law. The law does much to protect the quack medicine vendor because the laws of slander and libel are so severe.”> Clark himself was sued for libel after he’d written in a pamphlet “ ‘Cures’ for consumption, cancer and diabetes may fairly be classed as murderous”. Although he initially tried to fight the case, impending destitution eventually forced him to apologise [3]. If that happened today, the accusation would have been repeated on hundreds of web sites round the world within 24 hours, and the quack would, with luck, lose [4]. As early as 1927, Clark had written “Today some travesty of physical science appears to be the most popular form of incantation” [5]. That is even more true today. Homeopaths regularly talk utter nonsense about quantum theory [6] and ‘nutritional therapists’ claim to cure AIDS with vitamin pills or even with downloaded music files. Some of their writing is plain delusional, but much of it is a parody of scientific writing. The style, which Goldacre [7] calls ‘sciencey’, often looks quite plausible until you start to check the references. A 100 years on from the BMA’s efforts, we need once again to look at the efficacy of remedies. Indeed the effort is already well under way, but this time it takes a rather different form. The initiative has come largely from an “intrepid, ragged band of bloggers” and some good journalists, helped by many scientific societies, but substantially hindered by the BMA, the Royal Colleges, the Department of Health and a few vice-chancellors. Even NICE and the MHRA have not helped much. The response of the royal colleges to the resurgence in magic medicine that started in the 1970s seems to have been a sort of embarrassment. They pushed the questions under the carpet by setting up committees (often populated with known sympathizers) so as to avoid having to say ‘baloney’. The Department of Health, equally embarrassed, tends to refer the questions to that well-known medical authority, the Prince of Wales (it is his Foundation for Integrated Health that was charged with drafting National Occupational Standards in make-believe subjects like naturopathy [8]. Two recent examples suffice to illustrate the problems. The first example is the argument about the desirability of statutory regulation of acupuncture, herbal and traditional Chinese medicine (the Pittilo recommendations) [9]. Let’s start with a definition, taken from ‘A patients’ guide to magic medicine’ [10]. “Herbal medicine: giving patients an unknown dose of an ill-defined drug, of unknown effectiveness and unknown safety”. It seems to me to be self-evident that you cannot start to think about a sensible form of regulation unless you first decide whether what you are trying to regulate is nonsense, though this idea does not seem to have penetrated the thinking of the Department of Health or the authors of the Pittilo report. The consultation on statutory regulation has had many submissions [11] that point out the danger to patients of appearing to give official endorsement of treatments that don’t work. The good news is that there seems to have been a major change of heart at the Royal College of Physicians. Their submission points out with admirable clarity that the statutory regulation of things that don’t work is a danger to patients (though they still have a blank spot about the evidence for acupuncture, partly as a result of the recent uncharacteristically bad assessment of the evidence by NICE [12]). Things are looking up. Nevertheless, after the public consultation on the report ended on November 16th, the Prince of Wales abused his position to make a well-publicised intervention on behalf of herbalists [13]. Sometimes I think his mother should give him a firm lesson in the meaning of the term ‘constitutional monarchy’, before he destroys it. The other example concerns the recent ‘evidence check: homeopathy’ conducted by the House of Commons Science and Technology Select Committee (SCITECH). First the definition [10]: “Homeopathy: giving patients medicines that contain no medicine whatsoever”. When homeopathy was dreamt up, at the end of the 18th century, regular physicians were lethal blood-letters, and it’s quite likely that giving nothing saved people from them. By the mid-19th century, discoveries about the real causes of disease had started, but homeopaths remain to this day stuck in their 18th century time warp. In 1842 Oliver Wendell Holmes said all that needed to be said about medicine-free medicine [14]. It is nothing short of surreal that the UK parliament is still discussing it in 2009. Nevertheless it is worth watching the SCITECH proceedings [15]. The first two sessions are fun, if only for the statement by the Professional Standards Director of Boots that they sell homeopathic pills while being quite aware that they don’t work. I thought that was rather admirable honesty. Peter Fisher, clinical director of the Royal Homeopathic Hospital, went through his familiar cherry-picking of evidence, but at least repeated his condemnation of the sale of sugar pills for the prevention of malaria. But for pure comedy gold, there is nothing to beat the final session. The health minister, Michael O’Brien, was eventually cajoled into admitting that there was no good evidence that homeopathy worked but defended the idea that the taxpayer should pay for it anyway. It was much harder to understand the position of the chief scientific advisor in the Department of Health, David Harper. He was evasive and ill-informed. Eventually the chairman, Phil Willis, said “No, that is not what I am asking you. You are the Department’s Chief Scientist. Can you give me one specific reference which supports the use of homeopathy in terms of Government policy on health?”. But answer came there none (well, there were words, but they made no sense). Then at the end of the session Harper said “homeopathic practitioners would argue that the way randomised clinical trials are set up they do not lend themselves necessarily to the evaluation and demonstration of efficacy of homeopathic remedies, so to go down the track of having more randomised clinical trials, for the time being at least, does not seem to be a sensible way forward.” Earlier, Kent Woods (CEO of the MHRA) had said “the underlying theory does not really give rise to many testable hypotheses”. These two eminent people seemed to have been fooled by the limp excuses offered by homeopaths. The hypotheses are testable and homeopathy, because it involves pills, is particularly well suited to being tested by proper RCTs (they have been, and when done properly, they fail). If you want to know how to do it, all you have to do is read Goldacre in the Guardian [16]. It really isn’t vert complicated. “Imagine going to an NHS hospital for treatment and being sent away with nothing but a bottle of water and some vague promises.” “And no, it’s not a fruitcake fantasy. This is homeopathy and the NHS currently spends around £10million on it.” That was written by health journalist Jane Symons, in The Sun [17]. A Murdoch tabloid has produced a better account of homeopathy than anything that could be managed by the chief scientific advisor to the Department of Health. And it isn’t often that one can say that. These examples serve to show that the medical establishment is slowly being dragged, from the bottom up, into realising that matters of truth and falsehood are more important than their knighthoods. It is all very heartening, both for medicine and for democracy itself. David Colquhoun. Declaration of interests. I was A.J. Clark chair of pharmacology at UCL, 1985 – 2004. 1. Aronson, JK BMJ 2009;339:b5415 2. Clark, A,J, (1938) Patent Medicines FACT series 14, London. See also Patent medicines in 1938 and now https://www.dcscience.net/?p=257 3. David Clark “Alfred Joseph Clark, A Memoir” (C. & J. Clark Ltd 1985 ISBN 0-9510401-0-3) 4. Lewis, A. (2007) The Gentle Art of Homeopathic Killing 5. A.J. Clark (1927) The historical aspect of quackery, BMJ October 1st 1927 6. Chrastina, D (2007) Quantum theory isn’t that weak, (response to Lionel Milgrom). 7 Goldacre, B. (2008) Bad Science. HarperCollins 8. Skills for Health web site 9. A very bad report: gamma minus for the vice-chancellor 10. A Patients’ Guide to Magic Medicine, and also in the Financial Times. 12. NICE fiasco, part 2. Rawlins should withdraw guidance and start again 13. BBC news 1 December 2009 Prince Charles: ‘Herbal medicine must be regulated’. 14. Oliver Wendell Holmes (1842) Homeopathy and Its Kindred Delusions. 15. House of Commons Science and technology committee. Evidence check: homeopathy. Videos and transcripts available at http://www.viewista.com/s/fywlp2/ez/1 16. Goldacre, B. A Kind of Magic Guardian 16 November 2007. 17. Homeopathy is resources drain says |
Follow-up
There is a good account of the third SCITECH session by clinical science consultant, Majikthyse, at The Three Amigos.
16 December 2009.. Recorded an interview for BBC Radio 5 Live. It was supposed to go out early on 17th.
17 December 2009. The editorial is mentioned in Editor’s Choice, by deputy editor Tony Delamothe. I love his way of putting the problem "too many at the top of British medicine seem frozen in the headlights of the complementary medicine bandwagon". He sounds remarkably kind given that I was awarded (by the editor, Fiona Godlee, no less) a sort of booby prize at the BMJ party for having generated a record number of emails during the editing of a single editorial (was it really 24?). Hey ho.
17 December 2009. More information on very direct political meddling by the Prince of Wales in today’s Guardian, and in Press Association report.
17 December 2009. Daily Telegraph reports on the editorial, under the heading “ ‘Nonsense’ alternative medicines should not be regulated“. Not a bad account for a non-health journalist.
17 December 2009. Good coverage in the excellent US blog, Neurologica, by the superb Steven Novella.’ “Intrepid, Ragged Band of Bloggers” take on CAM‘ provides a chance to compare and contrast the problems in the UK and the USA.’
18 December 2009. Article in The Times by former special advisor, Paul Richards. “The influence of Prince Charles the lobbyist is out of hand. Our deference stops us asking questions.”
“A good starting point might be publication of all correspondence over the past 30 years. Then we will know the extent, and influence, of Prince Charles the lobbyist.”
Comments in the BMJ Quite a lot of comments had appeared by January 8th, though sadly they were mostly from the usual suspects who appear every time one suggests evidence matters. A reply was called for, so I sent this (the version below has links).
After a long delay, this response eventually appeared in the BMJ on January 15 2010.
It’s good to see so many responses, though somewhat alarming to see that several of them seem to expect an editorial to provide a complete review of the literature. I ‘ll be happy to provide references for any assertion that I made.
I also find it a bit odd that some people think that an editorial is not the place to express an opinion robustly. That view seems to me to be a manifestation of the very sort of political correctness that I was deploring. It’s a bit like the case when the then health minister, Lord Hunt, referred to psychic surgery as a “profession” when he should have called it a fraudulent conjuring trick. Anything I write is very mild compared with what Thomas Wakley wrote in the Lancet, a journal which he founded around the time UCL came into existence. For example (I quote)
“[We deplore the] “state of society which allows various sets of mercenary, goose-brained monopolists and charlatans to usurp the highest privileges…. This is the canker-worm which eats into the heart of the medical body.” Wakley, T. The Lancet 1838-9, 1
I don’t think it is worth replying to people who cite Jacques Benveniste or Andrew Wakefield as authorities. Neither is it worth replying to people who raise the straw man argument about wicked pharmaceutical companies (about which I am on record as being as angry as anyone). But I would like to reply directly to some of the more coherent comments.
Sam Lewis and Robert Watson. [comment] Thank you for putting so succinctly what I was trying to say.
Peter Fisher [comment]. I have a lot of sympathy for Peter Fisher. He has attempted to do some good trials of homeopathy (they mostly had negative outcomes). He said he was "very angry" when the non-medical homeopaths were caught out recommending their sugar pills for malaria prevention (not that this as stopped such dangerous claims which are still commonplace). He agreed with me that there was not sufficient scientific basis for BSc degrees in homeopathy. I suppose that it isn’t really surprising that he continues to cherry pick the evidence. As clinical director of the Royal London Homeopathic Hospital and Homeopathic physician to the Queen, just imagine the cognitive dissonance that would result if he were to admit publicly that is all placebo after all. He has come close though. His (negative) trial for homeopathic treatment of rheumatoid arthritis included the words "It seems more important to define if homeopathists can genuinely control patients’ symptoms and less relevant to have concerns about whether this is due to a ‘genuine’ effect or to influencing the placebo response” [2]. [download
the paper]. When it comes to malaria, it matters a lot.
Adrian White [comment] seems to be cross because I cited my own blog. I did that simply because if he follows the links there he will find the evidence. In the case of acupuncture it has been shown time after time that "real" acupuncture does not differ perceptibly from sham. That is true whether the sham consists of retractable needles or real needles in the "wrong" places. A non-blind comparison between acupuncture and no acupuncture usually shows some advantage for the former but it is, on average, too small to be of much clinical significance [3]. I agree that there is no way to be sure that this advantage is purely placebo effect but since it is small and transient it really doesn’t matter much. Nobody has put it more clearly than Barker Bausell in his book, Snake Oil Science [4]
White also seems to have great faith in peer review. I agree that in real science it is probably the best system we have. But in alternative medicine journals the "peers" are usually other true believers in whatever hocus pocus is being promoted and peer reveiw breaks down altogether.
R. M. Pittilo [comment] I’m glad that Professor Pittilo has replied in person because I did single out his report for particular criticism. I agree that his report said that NHS funding should be available to CAM only where there is evidence of efficacy. That was not my criticism. My point was that in his report, the evidence for efficacy was assessed by representatives of Herbal Medicine, Chinese Medicine and Acupuncture (four from each). Every one of them would have been out of work if they had found their subjects were nonsense and that, no doubt, explains why the assessment was so bad. To be fair, they did admit that the evidence was not all that it might be and recommended (as always) more research I’d like to ask Professor Pittilo how much money should be spent on more research in the light of the fact that over a billion dollars has been spent in the USA on CAM research without producing a single useful treatment. Pittilo says "My own view is that both statutory regulation and the quest for evidence should proceed together" but he seems to neglect the possibility that the quest for evidence might fail. Experience in the USA suggests that is exactly what has, to a large extent, already happened.
I also find it quite absurd that the Pittilo report should recommend, despite a half-hearted admission that the evidence is poor, that entry to these subjects should be via BSc Honours degrees. In any case he is already thwarted in that ambition because universities are closing down degrees in these subjects having realised that the time to run a degree is after, not before, you have some evidence that the subject is not nonsense. I hope that in due course Professor Pittilo may take the same action about the courses in things like homeopathy that are run by the university of which he is vice-chancellor. That could only enhance the academic reputation of Robert Gordon’s University.
George Lewith [comment] You must be aware that the proposed regulatory body, the Health Professions Council, has already broken its own rules about "evidence-based practice" by agreeing to take on, if asked, practitioners of Herbal Medicine, Chinese Medicine and Acupuncture. They have (shamefully) excluded the idea that claims of efficacy would be regulated. In other word they propose to provide exactly the sort of pseudo-regulation which would endanger patients They are accustomed to the idea that regulation is to do only with censoring practitioners who are caught in bed with patients. However meritorious that may be, it is not the main problem with pseudo-medicine, an area in which they have no experience. I’m equally surprised that Lewith should recommend that Chinese evaluation of Traditional Chinese medicine should be included in meta-analyses, in view of the well-known fact that 99% of evaluations from China are positive: “No trial published in China or Russia/USSR found a test treatment to be ineffective” [5]. He must surely realise that medicine in China is a branch of politics. In fact the whole resurgence in Chinese medicine and acupuncture in post-war times has less to do with ancient traditions than with Chinese nationalism, in particular the wish of Mao Tse-Tung to provide the appearance of health care for the masses (though it is reported that he himself preferred Western Medicine).
1. Lord Hunt thinks “psychic surgery” is a “profession”. https://www.dcscience.net/?p=258
2. Fisher, P. Scott, DL. 2001 Rheumatology 40, 1052 – 1055. [pdf file]
3. Madsen et al, BMJ 2009;338:a3115 [pdf file]
4. R, Barker Bausell, Snake Oil Science, Oxford University Press, 2007
5. Vickers, Niraj, Goyal, Harland and Rees (1998, Controlled Clinical Trials, 19, 159-166) “Do Certain Countries Produce Only Positive Results? A Systematic Review of Controlled Trials”. [pdf file]
15 January 2010. During the SciTech hearings, Kent Woods (CEO of the MHRA) made a very feeble attempt to defend the MHRA’s decision to allow misleading labelling of homeopathic products. Now they have published their justification for this claim. It is truly pathetic, as explained by Martin at LayScience: New Evidence Reveals the MHRA’s Farcical Approach to Homeopathy. This mis-labelling cause a great outcry in 2006, as documented in The MHRA breaks its founding principle: it is an intellectual disgrace, and Learned Societies speak out against CAM, and the MHRA.
22 January 2010 Very glad to see that the minister himself has chosen to respond in the BMJ to the editorial
|
Rt Hon. Mike O’Brien QC MP, Minister of State for Health Services I am glad that David Colquhoun was entertained by my appearance before the Health Select Committee on Homeopathy. But he is mistaken when he says, “you cannot start to think about a sensible form of regulation unless you first decide whether or not the thing you are trying to regulate is nonsense.” Regulation is about patient safety. Acupuncture, herbal and traditional Chinese medicine involve piercing the skin and/or the ingestion of potentially harmful substances and present a possible risk to patients. The Pittilo Report recommends statutory regulation and we have recently held a public consultation on whether this is a sensible way forward. Further research into the efficacy of therapies such as Homeopathy is unlikely to settle the debate, such is the controversy surrounding the subject. That is why the Department of Health’s policy towards complementary and alternative medicines is neutral. Whether I personally think Homeopathy is nonsense or not is besides the point. As a Minister, I do not decide the correct treatment for patients. Doctors do that. I do not propose on this occasion to interfere in the doctor-patient relationship. |
Here is my response to the minister
|
I am very glad that the minister himself has replied. I think he is wrong in two ways, one relatively trivial but one very important. First, he is wrong to refer to homeopathy as controversial. It is not. It is quite the daftest for the common forms of magic medicine and essentially no informed person believes a word of it. Of course, as minister, he is free to ignore scientific advice, just as the Home Secretary did recently. But he should admit that that is what he is doing, and not hide behind the (imagined) controversy. Second, and far more importantly, he is wrong, dangerously wrong, to say it I was mistaken to claim that “you cannot start to think about a sensible form of regulation unless you first decide whether or not the thing you are trying to regulate is nonsense". According to that view it would make sense to grant statutory regulation to voodoo and astrology. The Pittilo proposals would involve giving honours degrees in nonsense if one took the minister’s view that it doesn’t matter whether the subjects are nonsense or not. Surely he isn’t advocating that? The minister is also wrong to suppose that regulation, in the form proposed by Pittilo, would do anything to help patient safety. Indeed there is a good case to be made that it would endanger patients (not to mention endangering tigers and bears). The reason for that is that the main danger to patients arises from patients being given “remedies” that don’t work. The proposed regulatory body, the Health Professions Council, has already declared that it is not interested in whether the treatments work or not. That in itself endangers patients. In the case of Traditional Chinese Medicine, there is also a danger to patients from contaminated medicines. The HPC is not competent to deal with that either. It is the job of the MHRA and/or Trading Standards. There are much better methods of ensuring patient safety that those proposed by Pittilo. In order to see the harm that can result from statutory regulation, it is necessary only to look at the General Chiropractic Council. Attention was focussed on chiropractic when the British Chiropractic Association decided, foolishly, to sue Simon Singh for defamation. That led to close inspection of the strength of the evidence for their claims to benefit conditions like infant colic and asthma. The evidence turned out to be pathetic, and the result was that something like 600 complaints were made to the GCC about the making of false health claims (including two against practices run by the chair of the GCC himself). The processing of these complaints is still in progress, but what is absolutely clear is that the statutory regulatory body, the GCC, had done nothing to discourage these false claims. On the contrary it had perpetrated them itself. No doubt the HPC would be similarly engulfed in complaints if the Pittilo proposals went ahead. It is one thing to say that the government chooses to pay for things like homeopathy, despite it being known that they are only placebos, because some patients like them. It is quite another thing to endanger patient safety by advocating government endorsement in the form of statutory regulation, of treatments that don’t work. I would be very happy to meet the minister to discuss the problems involved in ensuring patient safety. He has seen herbalists and other with vested interests. He has been lobbied by the Prince of Wales. Perhaps it is time he listened to the views of scientists too. |
Both the minister’s response, and my reply, were reformatted to appear as letters in the print edition of the BMJ, as well as comments on the web..
A momentous decision was promulgated (as lawyers say) by the Information Tribunal on December 8th 2009. It marks a step forward in Freedom of Information about how universities spend your money. It has taken 3.5 years to get to this point. Perhaps now there will be an end to the attempts of every single university that I’ve
approached to conceal what they teach.
Decision
"The Tribunal upholds the decision notice dated 30th. March, 2009, dismisses the appeal and directs that all the steps required by the Decision Notice be taken within 28 days of the date of this Decision"
Back story for this case
24th July 2006. I asked the University of Central Lancashire (UCLAN) for copies of teaching materials and validation documents for their "BSc" degree in homeopathy (this degree no longer exists: it was abolished in 2008). A year later, UCLAN shut the rest of its courses in alternative medicine, after an internal review.
21 August 2006. I was sent the validation documents but refused the teaching materials as UCLAN claimed they were exempt under section 43(2) of the Freedom of Information Act (FOIA)(commercial interests). Two days later I sent a request for the mandatory internal review of the refusal.
4th October 2006. The internal review confirmed the original decision (it always does), and cited, as well as section .43(2) of FOIA, section 21.
21 October 2006. I appealed to the Information Commissioner. The basis of the appeal was that the university might have financial interests in the outcome, but not commercial interests, because universities are not commercial organisations as defined in section 43(2) of the FOIA. In addition, even if the commercial argument was not allowed, the public interest in knowing what was taught was sufficient to justify release of the requested materials.
21 January 2008. The Information Commissioner finally got round to starting on the case.
29 September 2008 The vice-chancellor, Malcolm McVicar, raised an objection to complying with my request under s.36(2)(c) of FOIA. This states that “In the reasonable opinion of a qualified person, disclosure of the information under this Act” “(c) would otherwise prejudice, or would be likely otherwise to prejudice, the effective conduct of public affairs..”
30 March 2009. The decision of the Information Commissioner was published. It has already been described here. Apart from one trivial matter, my appeal was upheld, and UCLAN was ordered to release the requested material within 35 days. However UCLAN did not release the material, but rather launched an appeal against the Information Commissioner. The appeal was heard by an Information Tribunal.
The full text of the Freedom of Information Act is here.
The Information Tribunal
The Tribunal heard the case of University of Central Lancashire v Information Commissioner in Manchester on November 3, 4 and 5. I was an ‘additional party’ to the proceedings and attended in person for the first two days, with the aim of helping the Information Commissioner’s case. This is what the tribunal looked like.
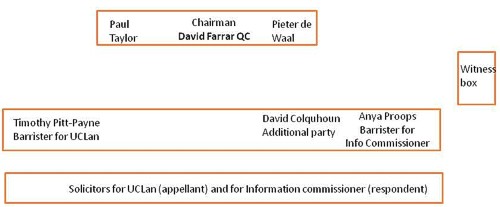
I was amazed to find myself sitting next to the barrister for the Information Commisioner, and still more amazed to be invited to cross-question the witnesses, after she had questioned them.
The witnesses were Malcom McVicar (vice-chancellor of UCLAN), Peter Hyett, (executive director of finance at UCLAN) and David Phoenix (Deputy vice-chancellor, UCLAN).
The outcome
The decision in full can be read here.
|
Decision The Tribunal upholds the decision notice dated 30th. March, 2009, dismisses the appeal and directs that all the steps required by the Decision Notice be taken within 28 days of the date of this Decision. |
So we won.
The details of the decision contain some matters of great interest for universities, in particular the dismissal of the idea that the public can be reassured by either internal or external (e.g. QAA) validation procedures. I’ll try to summarise them (paragraph numbering as in the decision
notice).
Commercial interests
The one disappointing thing about the Tribunal’s decision was that it contradicted the Information Commissioner’s decision on the meaning of commercial interests.
31 "Therefore, whether on a broad or narrow construction of the statutory words, we are satisfied that UCLAN `s interests in teaching material produced for its degree courses are properly described as “commercial”.
However, that does not affect the outcome because the Tribunal decided that there was no reason to think that the course materials actually had the commercial value that UCLAN said they did. For
example:
36 We were not impressed by the claim that third parties with copyright in the disclosed materials would be alienated by UCLAN `s compliance with a decision that this information must be provided. None gave evidence to that effect.
37 It was not clear to us how a competitor could significantly exploit access to this material, without infringing UCLAN `s copyright or brazenly aping the content of a course, which would surely attract the scorn of the wider academic community. Moreover, it seemed to us likely that most potential students would be attracted to a particular course by the reputation of the teaching staff and a range of extra – curricular factors at least as much as by a comparative study of the powerpoint presentations and notes provided to current students.
and
39 Finally, in this particular case, we doubt whether this course had a significant commercial value, given the limited enrolment and the virtual absence of overseas interest.
At this point, the appeal is essentially dismissed. Nevetheless, the Tribunal went on to discuss the other defences offered by UCLAN, and some of their conclusions are more interesting than the subtle distinction between ‘financial interests’ and ‘commercial interests’.
40 In the light of this finding, it is not strictly necessary to decide the balance of public interest as to disclosure. Nevertheless, since the issue has been carefully and very fully argued, we shall shortly indicate our view, had the likelihood of prejudice been established.
Public Interest
The commercial interest defence is subject to the public interest argument in s.1(2((b) of the FOIA’
(b) in all the circumstances of the case, the public interest in maintaining the exclusion of the duty to confirm or deny outweighs the public interest in disclosing whether the public authority
holds the information.
Hence, the decision notice says
41 As ever, the question is whether the public interest in maintaining the exemption outweighs the interest in disclosure.
On the question of public interest, the Tribunal comes down strongly on the side of the Commissioner and me.
46 The public interest in disclosure seems to us appreciably stronger. Apart from the universal arguments about transparency and the improvement of public awareness, we find that there are particular interests here, arising from the nature of a university and the way it is funded.
It is particularly interesting that the Tribunal dismissed the role of internal and external validation as a substitute for transparency. As part of their case (para 18) UCLAN had argued
"Moreover, standards were ensured by the validation procedures which were required before a course was launched and which involved independent expert external monitors and by quality assurance (Q.A.A.) which demands a continuing compliance with national standards."
This cut no ice with the Tribunal. In one of his few direct interjections the Tribunal Chairman, David Farrar Q.C., questioned a witness directly about the internal validation processes, Evidently he was not impressed by the answers. During my own cross questioning of the deputy vice-chancellor, I put to him the view that since the QAA [Quality Assurance Agency] was not allowed to take any notice of the content of courses, that getting a high mark from the QAA was not a substitute for seeing what was actually taught. The deputy vice-chancellor did not seem to disagree strongly with that view.
47 First, the public has a legitimate interest in monitoring the content and the academic quality of a course, particularly a relatively new course in a new area of study, funded, to a very significant extent, by the taxpayer. It is no answer, we consider, to say that this function is performed by the process of validation or the continuing monitoring of standards with external input. Whether or not these processes are conducted with critical rigour, it must be open to those outside the academic community to question what is being taught and to what level in our universities. The apparent perception in some quarters that the intellectual demands of some or many degree courses have been relaxed, that higher classes of degree are too lightly earned, may be largely or entirely unfounded. But it is highly important that the material necessary to a fair judgement be available. That material will often, if not always, include the basic content of the course, such as is requested here.
48 Secondly, this is especially the case where, as with the BSc. (Homeopathy), there is significant public controversy as to the value of such study within a university. In this case, that factor standing alone would have persuaded us that the balance of public interest favoured disclosure.
49 We are not attracted by the somewhat patrician argument that the general public, uninstructed in the specialist subject under scrutiny, would be incapable of forming a proper judgement. That might be so, were it impossible to seek independent expertise to assist in making an assessment. Happily, it is not.
50 Finally, there is a public interest in opening up new methods of teaching and new insights as to the content of courses, so as to stimulate the spread of good practice.
So, a hands down win on the public interest argument.
Prejudice to effective conduct of public affairs
I found incomprehensible the argument that disclosure would ‘prejudice the effective conduct of public affairs’. But it was raised (at the last minute) by UCLAN, and it was considered by the Tribunal. This defence refers to s.36(2)(c) of FOIA. It states that “In the reasonable opinion of a qualified person, disclosure of the information under this Act” “(c) would otherwise prejudice, or would be likely otherwise to prejudice, the effective conduct of public affairs..”
As noted at paragraph 17, it is common ground, established as to (iii), by the jurisprudence of the Tribunal, that this exemption is engaged if three requirements are met. They can be shortly labelled
(i) qualified person
(ii) reasonable opinion
(iii) reasonably arrived at.
The Tribunal seemed to be distinctly unimpressed by the arguments presented by UCLAN.
56 A reasonable opinion may be one with which the Tribunal emphatically disagrees, provided it is based on sound argument and evidence. With great respect to Professor McVicar, whose sincerity is not in question, we can find no adequate evidential basis for this opinion and consider that it rests on two misconceptions as to the application of FOIA. We do not find that it passes the required test of objective reasonableness.
57 We considered separately whether the opinion was reasonably arrived at. Again, our answer is no.
58 Section 36 provides for an exceptional exemption which the public authority creates by its own action, albeit subject to scrutiny of its reasonableness, the likelihood of prejudice and the question of the public interest. That factor of itself justifies a requirement that the authority provide substantial evidence as to the advice (other than legal advice) and the arguments presented to the qualified person upon which his opinion was founded. We emphasise that no set formula is required, just a simple clear record of the process.
59 The need for such evidence is all the greater where, as here, the authority invokes s.36 for the first time after the complaint to the IC [Information Commissioner].
60 The evidence consists of a briefly argued email from Dr. Bostock suggesting that s.36(2)(c) be invoked on the very broadly argued grounds already reviewed. The tone implicitly acknowledges that the claim is rather speculative. We are not concerned with the slightly uncertain use of possibility and likely but the impression left is of a last minute idea, not really thought through or investigated
but merely discussed with solicitors to tie it in to the FOIA. It was sent to the Vice Chancellor at 3.20pm. on a Friday afternoon, 26th. September, 2008, asking for the Vice Chancellor’s agreement. That agreement was forthcoming in a single sentence without further comment in an email reply timed at 12.05pm.on the following Monday.61 We find that the process of forming the necessary opinion was, to say the least, perfunctory, indeed far short of the careful assessment and investigation that normally supports a qualified opinion for the purposes of s.36.
62 Accordingly, we do not find that it was reasonably arrived at.
Conclusion
62 It is for these reasons that we uphold the Decision Notice. We record our gratitude for the helpful and succinct submissions of counsel on both sides and the incisive contribution of Professor Colquhoun. We wish to add that, whilst we have not accepted the great majority of the arguments advanced by UCLAN, we do not in any way seek to cast doubt on the veracity of the evidence of its witnesses, nor the honesty and loyalty with which they have sought to serve its interests.
63 Our decision is unanimous.
Signed David Farrar Q.C.
Watch this space to see what can now be revealed.
Follow-up
We have listed many reasons hear why you should never trust Boots. Here are the previous ones.
Can you trust Boots?
Don’t Trust Boots
Boots reaches new level of dishonesty with CoQ10 promotion
This post is about a "functional food". That is about something a bit more serious than homeopathy, though I’ll return to that standing joke in the follow-up, because of Boots’ latest shocking admission..
Alternative medicine advocates love to blame Big Pharma for every criticism of magic medicine. In contrast, people like me, Ben Goldacre and a host of others have often pointed out that the differences seem to get ever smaller between the huge Alternative industry (about $60 billion per year), and the even huger regular pharmaceutical industry (around $600 billion per year),
Boots are as good an example as any. While representing themselves as ethical pharmacists, they seem to have no compunction at all in highly deceptive advertising of medicines and supplements which are utterly useless rip-offs.
The easiest way to make money is to sell something that is alleged to cure a common, but ill-defined problem, that has a lot of spontaneous variability.. Like stress, for example.
The Times carried a piece Is Boots’s new Lactium pill the solution to stress?. Needless to say the question wasn’t answered. It was more like an infomercial than serious journalism. Here is what Boots say.
 |
What does it do? This product contains Lactium, a unique ingredient which is proven to help with the stresses of every day life, helping you through a stressful day. Also contains B vitamins, magnesium and vitamin C, which help to support a healthy immune system and energy levels. Why is it different? This one a day supplement contains the patented ingredient Lactium. All Boots vitamins and suppliers are checked to ensure they meet our high quality and safety standards. |
So what is this "unique ingredient", Lactium? It is a produced by digestion of cow’s milk with trypsin. It was patented in 1995 by the French company, Ingredia, It is now distributed in the USA and Canada by Pharmachem. which describes itself as “a leader in the nutraceutical industry.” Drink a glass of milk and your digestive system will make it for you. Free. Boots charge you £4.99 for only seven capsules.
What’s the evidence?
The search doesn’t start well. A search of the medical literature with Pubmed for "lactium" produces no results at all. Search for "casein hydrolysate" gives quite a lot, but "casein hydrolysate AND stress" gives only seven, of which only one looks at effects in man, Messaoudi M, Lefranc-Millot C, Desor D, Demagny B, Bourdon L. Eur J Nutr. 2005.
There is a list of nineteen "studies" on the Pharmachem web site That is where Boots sent me when I asked about evidence, so let’s take a look.
Of the nineteen studies, most are just advertising slide shows or unpublished stuff. Two appear to be duplicated. There are only two proper published papers worth looking at, and one of these is in
rats not man. The human paper first.
Paper 1 Effects of a Bovine Alpha S1-Casein Tryptic Hydrolysate (CTH) on Sleep Disorder in Japanese General Population, Zara de Saint-Hilaire, Michaël Messaoudi, Didier Desor and Toshinori Kobayashi [reprint here] The authors come from France, Switzerland and Japan.
This paper was published in The Open Sleep Journal, 2009, 2, 26-32, one of 200 or so open access journals published by Bentham Science Publishers.
It has to be one of the worst clinical trials that I’ve encountered. It was conducted on 32 subjects, healthy Japanese men and women aged 25-40 and had reported sleeping disorders. It was double blind and placebo controlled, so apart from the fact that only 12 of the 32 subjects were in the control group, what went wrong?
The results were assessed as subjective sleep quality using the Japanese Pittsburg Sleep Quality Index (PSQI-J). This gave a total .score and seven component scores: sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction.
In the results section we read, for total PSQI score
"As shown in Table 2, the Mann-Whitney U-test did not show significant differences between CTH [casein tryptic hydrolysate] and Placebo groups in PSQI-J total scores at D0 (U=85; NS), D14 (U=86.5; NS), D28 (U=98.5; NS) and D35 (U=99.5; NS)."
Then we read exactly similar statements for the seven component scores. For example,. for Sleep Quality
As shown in Table 3, the Mann-Whitney U-test did not show significant differences between the sleep quality scores of CTH and Placebo groups at D0 (U=110.5; NS), D14 (U=108.5; NS), D28 (U=110; NS) and D35 (U=108.5; NS).
The discussion states
"The comparisons between the two groups with the test of Mann-Whitney did not show significant differences, probably because of the control product’s placebo effect. Despite everything, the paired comparisons with the test of Wilcoxon show interesting effects of CTH on sleep disorders of the treated subjects. "
Aha, so those pesky controls are to blame! But despite this negative result the abstract of the paper says
"CTH significantly improves the PSQI total score of the treated subjects. It particularly improves the sleep quality after two weeks of treatment, decreases the sleep latency and the daytime dysfunction after four weeks of treatment.
Given the antistress properties of CTH, it seems possible to relate the detected improvement of sleep aspects to a reduction of stress following its’ chronic administration."
So there seems to be a direct contradiction between the actual results and the announced outcome of the trial. How could this happen? The way that the results are presented make it hard to
tell. As far as I can tell, the answer is that, having failed to find evidence of real differences between CTH and placebo, the authors gave up on the placebo control and looked simply at the change
from the day 0 basleine values within the CTH group and, separately, within the placebo group. Some of these differences did pass statistical significance but if you analyse it
that way. there is no point in having a control group at all.
How on earth did such a poor paper get published in a peer-reviewed journal? One answer is that there are now so many peer-reviewed journals, that just about any paper, however poor, can get published
in some journal that describes itself as ‘peer-reviewed’. At the lower end of the status hierarchy, the system is simply broken.
Bentham Science Publishers are the publishers of the The Open Sleep Journal. (pity they saw fit to hijack the name of UCL’s spiritual founder, Jeremy Bentham). They publish 92 online and print journals, 200 plus open access journals, and related print/online book series. This publsher has a less than perfect reputation. There can be no scientist of any age or reputation who hasn’t had dozens of emails begging them to become editors of one or other of their journals or to write something for them. They have been described as a "pyramid scheme” for open access. It seems that every Tom, Dick and Harry has been asked. They have been described under the heading Black sheep among Open Access Journals and Publishers. More background can be found at Open Access News..
Most telling of all, a spoof paper was sent to a Bentham journal, The Open Information Science Journal. . There is a good account of the episode the New Scientist, under the title “CRAP paper accepted by journal”. It was the initiative if a graduate student at Cornell University. After getting emails from Bentham, he said “”It really painted a picture of vanity publishing”. The spoof paper was computer-generated rubbish, but it was accepted anyway, without comment. Not only did it appear that is was never reviewed but the editors even failed to notice that the authors said the paper came from the "Center for Research in Applied Phrenology", or CRAP. .The publication fee was $800, to be sent to a PO Box in the United Arab Emirates. Having made the point, the authors withdrew the paper.
Paper 5 in the list of nineteen stidies is also worth a look. It’s about rats not humans but it is in a respectable journal The FASEB Journal Express Article doi:10.1096/fj.00-0685fje (Published online June 8, 2001) [reprint here].
Characterization of α-casozepine, a tryptic peptide from bovine αs1-casein with benzodiazepine-like activity. Laurent Miclo et al.
This paper provides the basis for the claim that digested milk has an action like the benzodiazepine class of drugs, which includes diazepam (Valium). The milk hydrolysate, lactium was tested in rats and found to have some activity in tests that are alleged to measure effects on anxiety (I haven’t looked closely at the data, since the claims relate to humans).. The milk protein, bovine αS1 casein contains 214 amino acids. One of the many products of its digestion is a 10-amino-acid fragment (residues 91 -100) known as α-casozepine and this is the only product that was found to have an affinity for the γ-amino-butyric acid (GABA) type A receptors, which is where benzodiazepines are thought to act. There are a few snags with this idea.
- The affinity of α-casozepine peptide had 10,000-fold lower affinity for the benzodiazepine site of the GABAA than did diazepam, whereas allegedly the peptide was 10-fold more potent than diazepam in one of the rat tests.
- The is no statement anywhere of how much of the α-casozepine peptide is present in the stuff sold my Boots, or whether it can be absorbed
- And if digested milk did act like diazepam, it should clearly be callled a drug not a food.
What’s the conclusion about lactium?
Here is what I make of it.
Does it relieve stress? The evidence that it works any better than drinking a glass of milk is negligible. Tha advertising is grossly misleading and the price is extortionate.
Corruption of science. There is a more interesting aspect than that though. The case of lactium isn’t quite like the regular sort of alternative medicine scam. It isn’t inherently absurd, like homeopathy. The science isn’t the sort of ridiculous pseudo-scientific ramblings of magic medicine advocates who pretend it is all quantum theory The papers cited here are real papers, using real instruments and published in real journals,
What is interesting about that is that they show very clearly the corruption of real science that occurs at its fringes, This is science in the service of the dairy industry and in the service of the vast supplements industry. These are people who want to sell you a supplement for everything.
Medical claims are made for supplements, yet loopholes in the law are exploited to maintain that they are foods not drugs. The law and the companies that exploit it are deeply dishonest. That’s bad enough. but the real tragedy is when science itself is corrupted in the service of sales.
Big Pharma and the alternative industry. Nowhere is the slose alliance between Big Pharma and the alternative medicine industry more obvious than in the supplement and nutriceutical markets. Often the same companies run both. Their aim is to sell you thinks that you don’t need, for conditions that you may well not have, and to lighten your wallet in the process. Don’t believe for a moment that the dark-suited executives give a bugger about your health. You are a market to be exploited.
If you doubt that, look from time to time at one of the nutraceutical industry web sites, like nutraingredients.com. They even have a bit to say about lactium. They are particularly amusing at the moment because the European Food Safety Authority (EFSA) has had the temerity to demand that when health claims are made for foods, there is actually some small element of truth in the claims. The level of righteous indignation caused in the young food industry executives at the thought that they might have to tell the truth is everywhere to see. For example, try Life in a European health claims wasteland. Or, more relevant to Lactium, Opportunity remains in dairy bioactives despite departures. Here’s
a quotation from that one.
“Tage Affertsholt, managing partner at 3A Business Consulting, told NutraIngredients.com that the feedback from industry is that the very restrictive approach to health claims adopted by the European Food Safety Authority (EFSA) will hamper growth potential.”
“Affertsholt said: “Some companies are giving up and leaving the game to concentrate on more traditional dairy ingredients.”
Science and government policy
It may not have escaped your notice that the sort of low grade, corrupted, fringe science described here, is precisely the sort that is being encouraged by government policies. You are expected to get lots of publications, so never mind the details, just churn ’em out; The hundreds of new journals that have been created will allow you to get as meny peer-reviwed publications as you want without too much fuss, and you can very easily put an editorship of one of them on your CV when you fill in that bit about indicators of esteem. The box tickers in HR will never know that it’s a mickey mouse journal.
Follow-up
Boots own up to selling crap
Although this post was nothing to do with joke subjects like homeopathy, it isn’t possible to write about Boots without mentioning the performance of their professional standards director, Paul Bennett, when he appeared before the Parliamentary Select Committee for Science and Technology.. This committee was holding an “evidence check” session on homeopathy (it’s nothing short of surreal that this should be happening in 2009, uh?). The video can be seen here, and an uncorrected transcript. It is quite fun in places. You can also read the written evidence that was submitted.
Even the Daily Mail didn’t misss this one. Fioana Macrae wrote Boots boss admits they sell homeopathic remedies ‘because they’re popular, not because they work’
“It could go down as a Boot in Mouth moment.
Yesterday, the company that boasts shelf upon shelf of arnica, St John’s wort, flower remedies and calendula cream admitted that homeopathy doesn’t necessarily work.
But it does sell. Which according to Paul Bennett, the man from Boots, is why the pharmacy chain stocks such products in the first place.
Mr Bennett, professional standards director for Boots, told a committee of MPs that there was no medical evidence that homeopathic pills and potions work.
‘There is certainly a consumer demand for these products,’ he said. ‘I have no evidence to suggest they are efficacious.
‘It is about consumer choice for us and a large number of our customers believe they are efficacious.’
His declaration recalls Gerald Ratner’s infamous admission in 1991 that one of the gifts sold by his chain of jewellers was ‘total crap’.”
The Times noticed too, with Boots ‘labels homeopathy as effective despite lack of evidence‘.
Now you know that you can’t trust Boots. You heard it from the mouth of their professional standards director.
A commentary on the meeting by a clinical scientist summed up Bennett’s contribution thus
"Paul Bennett from Boots had to admit that there was no evidence, but regaled the committee with the mealy-mouthed flannel about customer choice that we have come to expect from his amoral employer."
Well said
The third session of the Scitech evidence check can be seen here, and the uncorrected transcript is here. It is, in a grim way, pure comedy gold, More of that later.
You want to achieve inner peace? While still working on my latest piece about Boots the Chemists, I thought I should pass on at once some advice.to maintain your wellness levels I have no idea of its origin but it was passed on to me by Lindy (who regularly contributes excellent comments here)
.
|
I am passing this on to you because it definitely worked for me and we all could use more calm in our lives. By following the simple advice I heard on a Medical TV show, I have finally found inner peace. A Doctor proclaimed the way to achieve inner peace is to finish all the things you have started. So I looked around my house to see things I’d started and hadn’t finished,and, before leaving the house this morning, I finished off a bottle of Merlot, a bottle of shhardonay, a bodle of Baileys, a butle of vocka, a pockage of Prunglies, tha mainder of bot Prozic and Valum scriptins, the res of the Chesescke an a box a choclits. Yu haf no idr hou fkin gud I feal. Peas sen dis orn to dem yu fee AR in ned ov inr pis. |
Too bad that laughing is still a bit painful.
This is a post about Markovian queuing theory. But hang on, don’t run away. It isn’t so hard.
|
The idea came from my recent experience. On Friday 23 October, I was supposed to have a kidney removed at the Royal Marsden Hospital. At the very last minute the operation was cancelled. That is more irritating than serious. A delay of a few weeks poses no great risk for me. . |

|
The cancellation arose because there was no bed available in the High Dependency Unit (HDU), which is where nephrectomy patients go for a while after the operation. Was this a failure of the NHS? I think not and here’s why
The first reaction of a neighbour to this news was to say "that’s why I have private insurance". Well, wrong actually. For a start, at the Marsden private patients and NHS patients get identical treatment (the only difference on the NHS is that "you don’t get hot and cold running margaritas at your bedside", my surgeon said). And secondly, the provision of emergency beds poses a really difficult problem, which I’ll attempt to explain.
Bed provision raises a fascinating statistical question. How many beds must be available to make sure nobody is ever turned away? The answer, in principle, is an infinite number. In practice it is more than anyone can afford.
The HDU has eleven beds but let’s think about a simpler case to start with. If patients arrived regularly at a fixed rate, and each patient stayed for a fixed length of time. there would be no problem. Say, for example, that a patient arrived regularly at 10 am and 4 pm each day, and suppose that each patient stayed for exactly 46 hours. It’s pretty obvious that you’d need four beds. Each bed could take a patient every two days and there are two patients per day coming in. Allowing two hours for changing beds, all four beds would be occupied for essentially 100 percent of the time, actually 95% = 46 hours/48 hours).
Random arrivals
The problem arises because patients don’t arrive regularly and they don’t stay for a fixed length of time. What happens if patients arrive at random and stay for a random length of time? (We’ll get back to the meaning of ‘random’ in this context later.)
Suppose again that two patients per day arrive on average, and that each patient stays in the HDU for 46 hours on average. So the mean arrival rate, and the mean length of stay in the HDU are the same as in the first example. When there was no randomness, four beds coped perfectly.
But with random arrivals and random length of stay the situation is very different. With four beds, if a queue were allowed to build up, the average number of patients in the queue would be 21 and the average length of time a patient would spend waiting to get a bed would be 10.5 days. This would be an efficient use of resources because every time a bed was vacated it would be filled straight away from the queue. The resources would be used to the maximum possible extent:, 95%. But it would be terrible for patients. The length of the queue would, of course, fluctuate, as shown by this distribution (see below) of the queue length. Occasionally it might reach 100 or more.
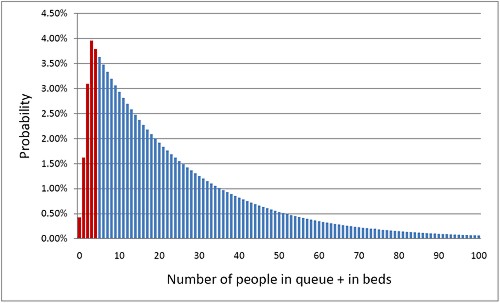
The histogram shows the total number of people in the system.The first five bins (red) represent the probabilities of 0, 1, 2, 3 or 4 beds being occupied. All the rest are in the queue.
What if you can’t queue?
For a High Dependency Unit or an Intensive Care Unit you can’t have a queue. If there is no bed, you are turned away. In the example just described, 91% of patients would have to wait, and that’s impossible in an HDU or ICU. The necessary statistical theory has been done for this case too (it is described as having zero queue capacity). Let’s look at the same case, with 4 beds, mean time between arrival of patients, 0.5 days, mean length of stay 1.917 days (46 hours).
|
In this case there is no queue so the only possibilities are that 0, 1, 2, 3 or all 4 beds are occupied. The relative probabilities of these cases are shown on the right (they add up to 100% because there are no other possibilities). |
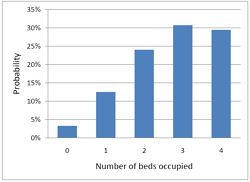
|
Despite the pressure on the unit, the randomness ensures that beds are by no means always occupied. All four are occupied for only 29% of the time and the average occupancy is 2.7 so the resources are used only 68% of the time (rather than 95% when a queue was allowed to form). Worse still, there is a 29% chance of the system being full, so you would be turned away.
So how many beds do you need? Clearly the more beds you have, the smaller the chance of anyone being turned away. But more beds means more cost and less efficiency. This is how it works out in our case.
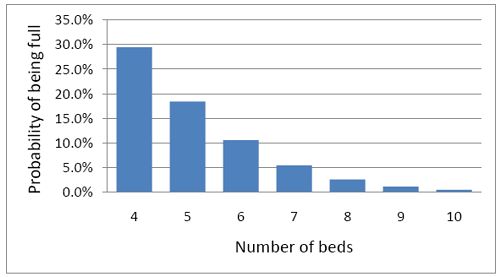
To get the chance of being turned away below 5%, rather than 29%, you’d have to double the number of beds from 4 to 8. But in doing so the beds would not be in use 68% of the time as with 4 beds, but for only 47% of the time.
|
Looked at another way, if you try to increase the utilisation of beds, above 50 or 60%, then the rate at which patients get turned away goes shooting up exponentially. |
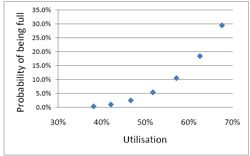
|
This isn’t inefficiency. It is an inevitable consequence of randomness in arrival times and lengths of stay.
A real life example
McManus et al. (2004) looked at all admissions to the medical–surgical Intensive Care Unit (ICU) of a large, urban children’s hospital in the USA during a 2-year period. (Anesthesiology 2004; 100:1271–6. Download pdf). Their Figure 2 shows the monthly average rejection rates mostly vary between 10 and 20%, so there is nothing unusual in there being no bed available in the private US medical system. For a period the rate of rejection reaches disastrous values, up to 47%. This happens, unsurprisingly, at times when the utilisation of beds was high.
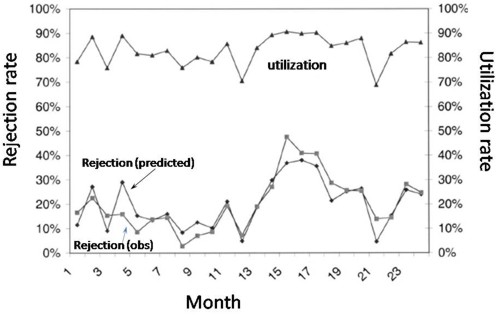
The observed relationship (McManus, Fig. 3) is very much as predicted above.with a very steep (roughly exponential) rise in rejection rate when the beds are in use for more than half the time.
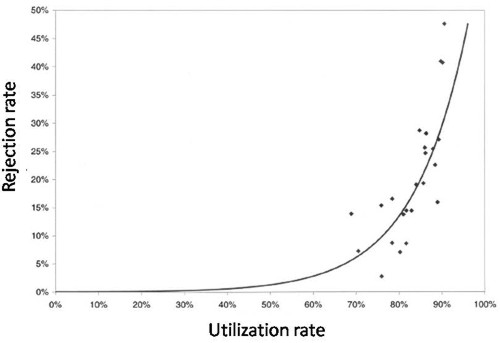
How to do the calculations
You can get the message without reading this section. It’s included for those who want to know a bit more about what we mean when we say that patients arrive at random rather than at fixed intervals, and that durations of stay in the unit have random rather than fixed durations.
Consider the durations of stay in the unit. They are variable in length and the usual way to represent variability is to plot a distribution of the variable quantity. The best known sort of probability distribution is the bell-shaped curve known as the Gaussian distribution. This is shown at the top of the Figure (note that pdf stands for probability density function, not portable document format).
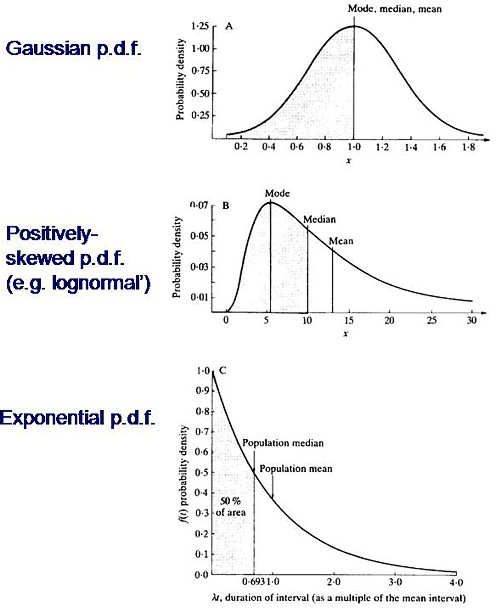
Not every sort of variability is described by a symmetrical bell-shaped curve. Quite often distributions with a positive skew are seen, like the middle example in the Figure. The distribution of incomes in the population have this sort of shape. Notice that more people earn less than average than earn more than average (the median is less than the mean). This can happen because those that earn less than average can’t get much less than average (unless we allow negative incomes), whereas bankers can earn (or at least be paid) a great deal more than average. The most frequent income (the peak of the distribution) is still smaller than the median.
An extreme form of a positively-skewed distribution is shown at the bottom. It is called the exponential distribution (because it has the shape of a decaying exponential curve). If this described personal incomes (and we are heading that way) it would mean that the most frequent income was zero and 63.2% of people earn less than average.
It is this last, rather unusual, sort of distribution that, in the simplest case, describes the lengths of random time intervals. This is getting very close to my day job. If an ion channel has a single open state, the lengths of individual ion channel openings is described by an exponential distribution.
|
The observation of an exponential distribution of durations is what would be predicted for a memoryless process, or Markov process. In the case of an ion channel, memoryless means that the probability of the channel shutting in the next microsecond is the same however long the channel has been open, This is exactly analogous to the fact that the probability of throwing a six with a die is exactly the same at each throw, regardless of how many sixes have been thrown before. |
Andrei A. Markov, 1856-1922 |
It is the simplest definition of a random length of time. For those who have done a bit of statistics, it is worth mentioning that if the number of events per unit time is described by a Poisson distribution, then the interval between events are exponentially-distributed. They are different ways of saying the same thing.
|
The lengths of stays in ICU in the McManus paper were roughly exponentially-distributed (right). The monthly average duration of stay ranged from 2.4 to 5.5 days, and average monthly admission rates to the 18 bed unit ranged from 4.6 to 6.2 patients per day. |
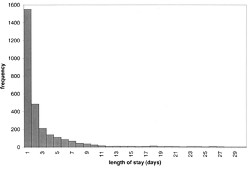
|
The monthly average percentage of patients who were turned away because there were no vacant beds varied widely, ranging from 3% up to a disastrous 47%
A technical note and an analogy with synapses
It’s intriguing to note that, in the simplest case, the time you’d spend waiting in a queue would have a simple exponential distribution (plus a discrete bit for the times when you don’t have to wait at all). The time you have to wait is the sum of all the lengths of stay of the people in front of you, and each of these lengths, in the case we discussing, is exponentially-distributed. If the queue was constant in length you can use a mathematical method known as convolution to show that the distribution of waiting time would follow a gamma distribution, a sort of distribution that goes through a peak, and eventually becomes Gaussian for long queues), However the queue is not fixed in length but its length is random (geometrically-distributed). It turns out that the distribution of the sum of a random number of exponentially distributed times is itself exponential. It is precisely this beautiful theorem that shows why the length of a burst of ion channel openings (which consists of the sum of a random number of exponentially-distributed open times, if you neglect the time spent in short shuttings) is, to a good approximation itself exponential, And that explains why the decay of synaptic currents is often close to following a simple exponential time course.
The calculations
The calculations for these graphs were done with a set of Excel add-in functions, Queueing Toolpak 4.0, which can be downloaded here. If this had been a paper of my own, rather than a blog post written in one weekend, I’d have done the algebra myself, just to be sure, The theory has much in common with that of single ion channels. Transitions between different states of the system can be described by transition rates or probabilities that don’t vary with time. The table, or matrix, of transition probabilities can be used to calculate the results, And if you want to know about the algebra of matrices, you could always apply for our summer workshop. There are some pictures from the workshop here.
Follow-up
Of course it is quite impossible for anyone who was around in the 60s to hear the name of a Russian mathematician without thinking of Tom Lehrer’s totally unjustified slur on another great Russian mathematician, Nicolai Ivanovich Lobachevsky. If you’ve never heard ‘Plagiarize’, you can hear it on Youtube. Sheer genius.
Why the size of the unit matters
This section was added as a result of a comment, below, from a statistician
At first glance one might think that if we quadruple the number of beds to 16 beds rather than 4, and we also quadruple the arrival rate to 8 rather than 2 per day, then the arrival rate per bed is the same and one might expect everything would stay the same.
As you say, it doesn’t.
If queueing was allowed, the mean queue length would be only slightly shorter, 18,7 rather than 20.9, but the mean time spent in the queue would fall from 10.5 days to 2.3 days.
In the more realistic case, with no queuing allowed, the rejection rate would fall from 29.4% to 15.5% and bed utilisation would increase from 68% to 81%. The rejection rate seems to fall roughly as the square root of the number of beds.
Clearly there is an advantage to having a big hospital with a big HDU.
Stochastic processes quite often behave unintuitive ways (unless you’ve spent years developing the right intuition).