
Download Lectures on Biostatistics (1971). Corrected and searchable version of Google books edition
Download review of Lectures on Biostatistics (THES, 1973).
David Colquhoun
It’s hard to know what to make of David Tredinnick MP (Cons, Bosworth). He is certainly an extreme example of the scientific ignorance of our parliamentary representatives, but he isn’t alone in that. Our present minister of Education, Michael Gove, memorably referred to Newton’s Laws of Thermodynamics, blissfully unaware that thermodynamics was a 19th century development. And our present Minister of Health seems to think that magic water cures diseases.
But Mr Treddinick breaks every record for anti-scientific nonsense. That, no doubt, is why he was upset by the recent revision of come NHS Choices web pages, so that they now give a good account of the evidence (that’s their job, of course). They did that despite two years of obstruction by the Department of Health. which seemed to think that it was appropriate to take advice from Michael Dixon of the Prince’s Foundation for integrated Health. That shocking example of policy based evidence was revealed on this blog, and caused something of a stir.
Treddinick’s latest letter
A copy of a letter from Mr Tredinnick to the Minister of Health, Jeremy Hunt, has some into my possession by a tortuous route [download the letter]. It’s a corker. Here are a few quotations.
"1. UKIP moving onto our ground
Attached is an extract from a recent UKIP policy statement. The position which UKIP has taken is one with which most of our Daily Mail reading supporters of complementary medicine would agree."
It seems that Treddinick’s preferred authority on medicine is now Nigel Farage, leader of the UK’s far right party. UKIP’s policy on health is appended to the letter, and it’s as barmy as most of the other things they say.
"2. Herbal Medicine
. . .there is very real concern that the Government will not regulate Herbal Medicine and Traditional Chinese Medicine. The current situation is unacceptable, because herbal practitioners need regulation and cannot function as herbal therapists, nor can they cannot obtain stocks of their herbal remedies, without it.
This refers to a saga that has been running for at least 10 years. Herbalists are desperate to get a government stamp of approval by getting statutory regulation, much like real doctors have, despite the fact that they make money by selling sick people "an unknown dose of an ill-defined drug, of unknown effectiveness and unknown safety" (as quoted recently in the House of Lords).
Even the US National Center for Complementary and Alternative Medicine (NCCAM) doesn’t claim that a single herbal treatment is useful. The saga of herbal regulation is long and tedious. The short version is that a very bad report, The Pittilo report, recommended regulation of herbalists. After years of prevarication, Andrew Lansley ignored the impartial scientific advice and yielded to the pressure from the herbal industry to accept the Pittilo report. But still nothing has happened.
Could it be that even Jeremy Hunt realises, deep down, that the regulation of nonsense is a nonsense that would harm the public?
We can only hope that a letter from Mr Tredinnick is the kiss of death. Perhaps his continuous pestering will only reinforce the doubts that seem to exist at the Department of Health.
Then Tredinnick returns (yawn) to his obsession with magic water. He vents his rage at the now excellent NHS Choices page on homeopathy.
3. Homeopathy
"Recently this wording has been removed and instead a comment by the Chief Medical Officer that homeopathy is placebo inserted in its place, as well as links to external organisations which campaign against homeopathy. For instance, there is a link to the Sense About Science website, and Caroline Finucane, who is Editor of new content at NHS Choices, also writes for the Sense About Science website. This is an organisation which has no expertise in homeopathy and traces its roots back to the ultra-left Revolutionary Communist Party (RCP)."
"I respectfully suggest that the original wording be reinstated and these links to external organisations be removed or changed to ensure a balanced view.".
So it seems that he prefers the medical views of Nigel Farage and the Prince of Wales to those of the Chief Medical Officer and the government’s chief scientist. Disgracefully, Tredinnick picks out one particular employee of NHS Choices among many, and one who does an excellent job. And he raises the hoary old myth that Sense About Science is a communist organisation. Odd, since others accuse it of being neo-libertarian. The actual history is here. The organisation that is a bit too libertarian for my taste is Spiked Online. I haven’t agreed with every word that Sense about Science has printed, but they have a totally honest belief in evidence.
To drag in the name of one person out of many, and to justify it by a false history shows, once again, how very venomous and vindictive the advocates of delusional medicine can be when they feel cornered.
A bit more information about Mr Treddinick
This is what the BBC News profile says about him.
|
David Tredinnick is an old style Conservative MP, being an Eton-educated former Guards officer, who has sat in the Commons since 1987. However, his ambition for high office was thwarted by his role in one of the sleaze stories which helped to sink the Major government. He accepted £1,000 from an undercover reporter to ask parliamentary questions about a fictitious drug. He was obliged to resign from his role as a PPS and was suspended from the Commons for 20 sitting days. He has not sat on the frontbench since. He is an orthodox Conservative loyalist, though he is more supportive of the European Union than many of his colleagues. He has, however, carved himself a niche as the Commons’ most enthusiastic supporter of complementary medicine. He has wearied successive health secretaries with his persistent advocacy of any and all homeopathic remedies. He has also supported their use in prisons and even suggested them as an aid in alleviating the foot and mouth crisis. |
|
Tredinnick has also asserted that he was aware of a psychiatric hospital that doubled its staff at full moon (this is an old urban myth, and is, of course, quite untrue). His advocacy of homeopathic borax as a way to control the 2001 epidemic of foot and mouth diease can be read here. Luckily it was ignored by the government. I hope his latest letter will be treated similarly. Picture of David Tredinnick MP from the Conservative Party |
 |
Follow-up
Today the Royal Society elected Andrew, Duke of York, as a “Royal Fellow”. Well, to be exact. 11% of them did. The numbers, which the Society has not made public, were as follows (as fraction of the electorate, 1300 Fellows)
Yes 147 (11%)
No 24 (2%)
Blank ballot 1 (0.08%)
Failed to vote 1128 (87%)
Hardly resounding support, then.
When I heard that the Society’s Council had nominated the Duke of York, I was sufficiently outraged to write a piece along the lines below. I was thinking about breaking the rules and going public with it before the election. I’m not particularly republican, but I do think that the Royal family still have too much influence on politics (as well as pernicious social effects).
On Monday 8th April I discussed the matter with the president, Paul Nurse. He was charm itself, but he didn’t explain what the advantages to the society were, and he didn’t agree to my proposal to mail my views to all Fellows. It seems odd that fellows have no way to communicate with each other , but that is how it is. But he did agree to set up an internal web site where Fellows could discuss the nomination in private. Most of them didn’t bother, but those who did were unanimous in supporting my views, apart from three members of Council, which had nominated him. Some people think that it is better to not to air disagreements in public. I don’t agree. I think it should be known that few people voted for this move. So here is what I wrote,
A curious fellow
The Royal Society has, on the whole, some pretty bright Fellows. It’s been around for 360 years and that, no doubt, is why it also has some quaintly archaic customs. One of them is the election of “Royal Fellows”. They are described as “Members of the Society by virtue of royal blood”, though ‘royal blood’ is a curiously unscientific idea.
The Royal Society was founded in 1660, and was granted a royal charter by Charles 2nd. The Society was a manifestation of the age of enlightenment. It might be seen as a harmless eccentricity that one of the present royal fellows said that he was rather proud to have been accused of being an enemy of the enlightenment. That, of course, was the Prince of Wales (known affectionately in the blogosphere as the Quacktitioner Royal).
The Royal Society was founded to advocate the idea that observation was what mattered, not deference to authority. The exception to that seems to be deference to “royal blood”.
But I believe it is taking deference too far to elect Prince Andrew. Not believing in science is one thing. Accusations of bribery and corruption in the sales of arms to dictators are quite another. From the leak of US diplomatic cables in 2010 we know, through cables from the US Ambassador to Kyrgyzstan, some unsavoury facts. During discussions of bribery in Kyrgyzstan and the investigation into the Al-Yamamah arms deal, the Duke “railed at British anti-corruption investigators, who had had the “idiocy” of almost scuttling the Al-Yamama deal with Saudi Arabia”. He was talking about kickbacks to a senior Saudi royal had allegedly received in exchange for a huge arms contract with BAE Systems. The cable went on “He then went on to ‘these (expletive) journalists, especially from the National [sic] Guardian, who poke their noses everywhere’ and (presumably) make it harder for British businessmen to do business. The crowd practically clapped!”. There could hardly be stronger evidence that bribery to sell arms had the approval of the Duke of York. The affair was hushed up when Tony Blair’s government shut down the investigation into the affair by the Serious Fraud Office, but the head of the SFO said that the decision to stop the investigation may have damaged “the reputation of the UK as a place which is determined to stamp out corruption”. The USA was less squeamish. A judge said that BAE’s conduct involved “deception, duplicity and knowing violations of law, I think it’s fair to say, on an enormous scale”. This is what the Duke of York was so eager to hide from the eyes of “these (expletive) journalists”.
Earlier in 2010 it was discovered that the billionaire son-in-law of Kazakhstan’s President paid the Duke of York’s representatives £15m via offshore companies, for the Duke’s mansion, Sunninghill Park. That was investigated by prosecutors in Italy and Switzerland.
It doesn’t end there. In 2011 the Duke of York got yet more bad press after revelation of his close friendship with Jeffrey Epstein, who was convicted in Florida for soliciting an underage girl for prostitution. In July 2011, the Duke’s role as a trade representative was ended.
As recently as 2012, the Duke was criticised for his close friendship with the president of Azerbaijan, Ilham Aliyev, who is regarded as one of the most brutal and corrupt rulers in the world. By this time, Prince Andrew had He lost the support of even the most Royalist newspapers.
A record like that makes the Duke of York an unsuitable person to be a member of any club, never mind election as a fellow of the Royal Society.
There is one section of society which regards scientists as amoral automatons, willing to shut their eyes to wrongdoing if it is in their own interest to do so. I have met very few such people, but the election of Prince Andrew can only reinforce that view.
The citation sent to me by the Royal Society mentioned none of his unsavoury history. It referred only to the ‘benefits’ that election would have for the Society. What exactly these benefits are has never been explained. They seem to amount to chairing a few meetings and dinners. Many of us would prefer not to have dinner with him. The nomination was a good example of that prime scientific crime, cherry-picking the evidence.
The proposal was accompanied by a ballot form. The form had a single box, labelled “I support the election of HRH the Duke of York KG GCVO as a Royal Fellow of the Royal Society”.
That’s the sort of ballot form used for senior posts in the Royal Society. It would be popular in Kazakhstan or Saudi Arabia.
Here is the ballot form that I returned [download pdf]
Follow-up
5 May 2013. The Sunday Times was on to this story quickly, and it was on their front page.

The story [download pdf] quotes past president Robert May, and Peter Lawrence (prof of Molecular Biology, LMB, Cambridge) who supported my views.
5 May 2013. I had the best laugh for years when I read the post by James Wilsdon who is now professor of science and democracy at the University of Sussex, but was previously director of science policy at the Royal Society, so he has had an inside view. His post makes mine look gentle.
“But now, Prince Andrew has been invited into the Royal Society’s ranks. And a fair number of his fellow Fellows aren’t happy. First off the blocks was David Colquhoun, UCL’s most famous pipe-smoking pharmacologist, who on Friday launched a full-frontal attack on his blog on what he called a “right Royal cock-up”. And today, the story has hit the front pages of the Sunday Times, with even the society’s former president, Bob May, reportedly “dismayed” over Andrew’s election. ”
“Controversy surrounding his role as a UK trade envoy, and his equally unsavoury association with a convicted US sex offender led to him resigning his role as “Airmiles Andy” in July 2011. Ministers and senior officials within the Foreign Office privately breathed a sigh of relief.
It was around this time that Prince Andrew started popping up more regularly at Royal Society events, offering to chair meetings and lend his support. (I was still working there at the time as director of science policy). The sensible response would have been to steer well clear, but as I witnessed at first hand, for such an incredibly clever bunch of people, elected themselves on merit (the very antithesis of hereditary royal privilege) many fellows of the Royal Society were susceptible to feudal levels of swooning at the merest flash of royal ermine. The centrepiece of its 350th anniversary celebrations in 2010 was an orgy of obsequiousness at the Festival Hall, with no fewer than seven Royals and 2000 guests in attendance to see Prince William receive his Royal Fellowship (no doubt for his outstanding services to art history, geography and steering helicopters).”
“Full credit to David Colquhoun for shining a light into one of the darker recesses of the scientific establishment. Of course, defenders of the decision will point out that this is the “Royal” Society, and a bit of old-fashioned bowing and scraping is part of its unique British charm. But there are plenty of equally prestigious institutions with a rich royal history that have modernised those networks of patronage, and aren’t spending the 21st century with their heads rammed quite so firmly up the Windsor arse. Nullius in verba, old chaps, nullius in verba…”
As we say in the blogosphere, ROFL.
The Guardian had a lot of coverage too. James Wilsdons piece appeared also in Guardian blogs: Royal society row over election of Prince Andrew as fellow. There is also a piece on the same topic by Peter Walker, “Royal Society scientists angered by Prince Andrew’s election as fellow“.
6 May 2013. There is an account in the Daily Mail by Nick Fagge. I won’t link to it because it is a shameless cut and paste job from the Sunday Times, with several mistakes added. The Mail at its worst.
The Independent asked for an op-ed column from me on Sunday. It appeared the next day. Mostly it was a shortened version of this blog, with the links removed (I wish they wouldn’t do that). But I did get in a comment that I often make in private.
“Certainly monarchs in recent times have shown little interest in science. If I wanted a tip for the winner of the 14.30 at Newmarket, I’d ask a royal. For most other questions, I wouldn’t.”
The Independent also carried a piece by Kate Morris on the same topic.
The Times had an interesting piece, by Hannah Devlin. They quote James Wilsdon
“James Wilsdon, Professor of Science and Democracy at the University of Sussex and formerly head of policy at the Royal Society, described the appointment on Twitter as “needless establishment toadying”. “Plenty of institutions with a royal history that aren’t spending the 21st century with their heads lodged quite so firmly up the Windsor a***,” he tweeted yesterday.”
and
“Richard Horton, editor of the medical journal The Lancet said that the decision to “grovel to royal patronage” was an “embarrassment for science” and “symptomatic of Britain’s corrupt honours system”.”
The Financial Times had a short report too.
International coverage
The story quickly went international. Stories appeared in the Gulf Times, the Economic Times, the Statesman (India), the Kashmir Times, the Indian Express
USA News Online reproduced both the Guardian article and James Wilsdon’s feisty piece in the Guardian.
7 May 2013
There is a report today in Paris Match “Andrew trop Royal pour la Royal Society”
8 May 2013.
Alice Thomson writes in the Times “One more reform for the Queen: her family. She needs to streamline ‘the Firm’, especially when the Royal Society treats a minor royal with absurd deference”.
Here are a few quotations.
“Yet the Fellows (or rather 11 per cent of these illustrious academics) have elected the grand young Duke of York to their number, a man who may have many hidden talents but who paddles at the shallower end of the intellectual pool.”
“it seems extraordinary that they have elected a minor member of the Royal Family who once piloted helicopters and knows more about golf than genomes.
The RS is obviously royal as well as a society but they already have Prince Philip, the Prince of Wales, the Princess Royal and Prince William. Any more and they will start looking like the Sandringham Christmas shoot. They stopped electing prime ministers after Margaret Thatcher but seem incapable of excluding the fourth in line to the throne.
This makes the Fellows appear antiquated and obsequious; but the bigger problem is what to do with these minor Royals.”
“But his tenure as special trade envoy has not been a success. He managed to turn the fairytale of the Princess and the Pea into the nightmare of the Prince and the Paedophile when he befriended the sex offender Jeffrey Epstein. ”
“No 10 increasingly don’t know what to do with him. “No one knows whether to bow, shake his hand or quietly slip out of the room when he arrives,” says one minister. The Queen tried to make amends by bestowing on him the Knight Grand Cross of the Royal Victorian Order, which allows him to wear a red, white and blue sash. ”
“The Royal Society was set up as a manifestation of the age of enlightenment. Nearly 360 years later, we should be enlightened enough to enjoy our constitutional monarchy — but we should not be bowing and scraping to the minor players in the Royal Family. They should have retired from the national stage long ago.”
This all seems very sensible to me. Incidentally, Alice Thomson is great-granddaughter of the famous physicist, J. J. Thomson, who was president of the Royal Society from 1915 to 1920.
10 May 2013 The affair has even reached Have I Got News for You. Here is the clip.
The Daily Mirror also weighed in, in fine tabloid style
Cack Andy-ed
The Royal Society, Britain’s top scientists’ club, has elected Prince Andrew a member.
Why? Nobody would ever accuse the Duke of York of being an intellectual. He’s as dim as a Toc H lamp.
The ballot paper permitted only a “Yes” vote, and 90% of members declined to back him.
A right royal farce. Only really clever people could make such common fools of themselves.
The nation’s best brains should stop tugging their forelock and drop “royal” from their title.
The royals don’t know a hypotenuse from a hyphen. Why not just call it The Science Society?
An interview on Voice of Russia Listen here
This article has been re-posted on The Winnower, so it now has a digital object identifier: DOI: 10.15200/winn.142935.50603
The latest news: eating red meat doesn’t do any harm. But why isn’t that said clearly? Alarmism makes better news, not only for journalists but for authors and university PR people too.
I’ve already written twice about red meat.
In May 2009 Diet and health. What can you believe: or does bacon kill you? based on the WCRF report (2007).
In March 2012 How big is the risk from eating red meat now? An update.
In the first of these I argued that the evidence produced by the World Cancer Research Fund (WCRF) for a causal relationship was very thin indeed. An update by WCRF in 2010 showed a slightly smaller risk, and weakened yet further the evidence for causality, though that wasn’t reflected in their press announcement.
The 2012 update added observations from two very large cohort studies. The result was that the estimates of risk were less than half as big as in 2009. The relative risk of dying from colorectal cancer was 1.21 (95% Confidence interval 1.04–1.42) with 50 g of red or processed meat per day, whereas in the new study the relative risk for cancer was only 1.10 (1.06-1.14) for a larger ‘dose’, 85 g of red meat. Again this good news was ignored and dire warnings were issued.
This reduction in size of the effect as samples get bigger is exactly what’s expected for spurious correlations, as described by Ioannidis and others. And it seems to have come true. The estimate of the harm done by red meat has vanished entirely in the latest study.
The EPIC study
This is the European Prospective Investigation into Cancer and Nutrition, another prospective cohort study, so it isn’t randomised [read the original paper]. And it was big, 448,568 people from ten different European countries. These people were followed for a median time of 12.7 years, and during follow-up 26,344 of them died.
The thing that was different about this paper was that red meat was found to pose no detectable risk, as judged by all-cause mortality. But this wasn’t even mentioned in the headline conclusions.
Conclusions: The results of our analysis support a moderate positive association between processed meat consumption and mortality, in particular due to cardiovascular diseases, but also to cancer.
To find the result you have to dig into Table 3.
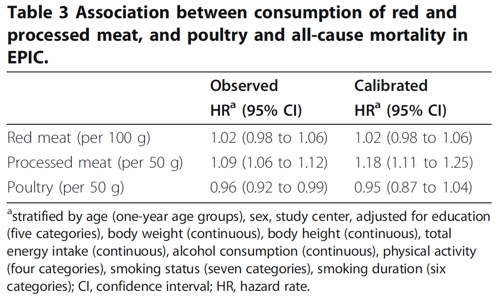
So, by both methods of calculation, the relative risk from eating red meat is negligible (except possibly in the top group, eating more than 160 g (7 oz) per day).
There is still an association between intake of processed meat and all-cause mortality, as in previous studies, though the association of processed meat with all-cause mortality, 1.09, or 1.18 depending on assumptions, is, if anything, smaller than was observed in the 2012 study, in which the relative risk was 1.20 (Table 2).
Assumptions, confounders and corrections.
The lowest meat eaters had only 13% of current smokers, but for the biggest red meat eaters it was 40%, for males. The alcohol consumption was 8.2 g/day for the lowest meat eaters but 23.4 g/day for the highest-meat group (the correlations were a bit smaller for women and also for processed meat eaters).
These two observations necessitate huge corrections to remove the (much bigger) effects of smoking and drinking if we want find the association for meat-eating alone. The main method for doing the correction is to fit the Cox proportional hazards model. This model assumes that there are straight-line relationships between the logarithm of the risk and the amount of each of the risk factors, e.g smoking, drinking, meat-eating and other risk factors. It may also include interactions that are designed to detect whether, for example, the effect of smoking on risk is or isn’t the same for people who drink different amounts.
Usually the straight-line assumption isn’t tested, and the results will depend on which risk factors (and which interactions between them) are included in the calculations. Different assumptions will give different answers. It simply isn’t known how accurate the corrections are when trying to eliminate the big effect of smoking in order to isolate the small effect of meat-eating. And that is before we get to other sorts of correction. For example, the relative risk from processed meat in Table 3, above, was 9% or 18% (1.09, or 1.18) depending on the outcome of a calculation that was intended to increase the accuracy of food intake records ("calibration").
The Conclusions of the new study don’t even mention the new result with red meat. All they mention is the risk from processed meat.
In this population, reduction of processed meat consumption to less than 20 g/day would prevent more than 3% of all deaths. As processed meat consumption is a modifiable risk factor, health promotion activities should include specific advice on lowering processed meat consumption.
Well, you would save that number of lives if, and only if, the processed meat was the cause of death. Too many epidemiologists, the authors pay lip service to the problem of causality in the introduction, but then go on to assume it in the conclusions. In fact the problem of causality isn’t even metnioned anywhere in either the 2012 study, or the new 2013 EPIC trial.
So is the risk of processed meat still real? Of course I can’t answer that. All that can be said is that it’s quite small, and as sample sizes get bigger, estimates of the risk are getting smaller. It wouldn’t be surprising if the risk from processed meat were eventually found not to exist, just as has happened for red (unprocessed) meat
The Japanese study
Last year there was another cohort study, with 51,683 Japanese. The results were even more (non-) dramatic [Nagao et al, 2012] than in the EPIC trial. This is how they summarise the results for the relative risks (with 95% confidence intervals).
"…for the highest versus lowest quintiles of meat consumption (77.6 versus 10.4 g/day) among men were 0.66 (0.45 — 0.97) for ischemic heart disease, 1.10 (0.84 — 1.43) for stroke and 1.00 (0.84 — 1.20) for total cardiovascular disease. The corresponding HRs (59.9 versus 7.5 g/day) among women were 1.22 (0.81 — 1.83), 0.91 (0.70 — 1.19) and 1.07 (0.90 — 1.28). The associations were similar when the consumptions of red meat, poultry, processed meat and liver were examined separately.
CONCLUSION: Moderate meat consumption, up to about 100 g/day, was not associated with increased mortality from ischemic heart disease, stroke or total cardiovascular disease among either gender."
In this study, the more meat (red or processed) you eat, the lower your risk of ischaemic heart disease (with the possible exception of overweight women). The risk of dying from any cardiovascular disease was unrelated to the amount of meat eaten (relative risk 1.0) whether processed meat or not.
Of course it’s possible that things which risky for Japanese people differ from those that are risky for Europeans. It’s also possible that even processed meat isn’t bad for you.
The carnitine study
The latest meat study to hit the headlines didn’t actually look at the effects of meat at all, though you wouldn’t guess that from the pictures of sausages in the headlines (not just in newspapers, but also in NHS Choices). The paper [reprint] was about carnitine, a substance that occurs particularly in beef, with lower amounts in pork and bacon, and in many other foods. The paper showed that bacteria in the gut can convert carnitine to a potentially toxic substance, trimethylamine oxide (TMAO). That harms blood vessels (at least in mice). But to show an effect in human subjects they were given an amount of carnitine equivalent to over 1 lb of steak, hardly normal, even in the USA.
The summary of the paper says it is an attempt to explain "the well-established link between high levels of red meat consumption and CVD [cardiovascular disease] risk". As we have just seen, it seems likely that this risk is far from being “well-established”. There is little or no such risk to explain.
It would be useful to have a diagnostic marker for heart disease, but this paper doesn’t show that carnitine or TMAO) is useful for that. It might also be noted that the authors have a maze of financial interests.
Competing financial interests Z.W. and B.S.L. are named as co-inventors on pending patents held by the Cleveland Clinic relating to cardiovascular diagnostics and have the right to receive royalty payments for inventions or discoveries related to cardiovascular diagnostics from Liposciences. W.H.W.T. received research grant support from Abbott Laboratories and served as a consultant for Medtronic and St. Jude Medical. S.L.H. and J.D.S. are named as co-inventors on pending and issued patents held by the Cleveland Clinic relating to cardiovascular diagnostics and therapeutics patents. S.L.H. has been paid as a consultant or speaker by the following companies: Cleveland Heart Lab., Esperion, Liposciences, Merck & Co. and Pfizer. He has received research funds from Abbott, Cleveland Heart Lab., Esperion and Liposciences and has the right to receive royalty payments for inventions or discoveries related to cardiovascular diagnostics from Abbott Laboratories, Cleveland Heart Lab., Frantz Biomarkers, Liposciences and Siemens.
The practical significance of this work was summed up the dietitian par excellence, Catherine Collins, on the BBC’s Inside Health programme.
Listen to Catherine Collins on carnitine.
She points out that the paper didn’t mean that we should change what we already think is a sensible diet.
At most, it suggests that it’s not a good idea to eat 1 lb steaks very day.
And the paper does suggest that it’s not sensible to take the carnitine supplements that are pushed by every gym. According to NIH
"twenty years of research finds no consistent evidence that carnitine supplements can improve exercise or physical performance in healthy subjects".
Carnitine supplements are a scam. And they could be dangerous.
Follow-up
Another blog on this topic, one from Cancer Research UK also fails to discuss the problem of causality. Neither does it go into the nature (and fallibility) of the corrections for counfounders like smoking and alcohol,. Nevertheless that, and an earlier post on Food and cancer: why media reports are often misleading, are a good deal more realistic than most newspaper reports.
The time when I lose patience with quacks is when they make unjustified claims about serious diseases. Giving false hope to the desperate (often at a high price) is plain wicked. If the patient stops more effective treatment, it’s homicide. Homeopaths have been jailed for that. Sometimes it’s a result of wishful thinking. Sometimes it’s to make money. The latter is morally more despicable. Both are culpable.
|
One example was the Totnes (aka Narnia) to “offer real alternatives to the conventional approach to cancer health care“. Another case, the Dove Clinic, was investigated in the Sunday Times, by Jon Ungoed-Thomas and Justin Stoneman: Clinics mislead patients over cancer ‘cure‘. |
|
There is yet another cancer conference, Back2Health, coming up in April (remember that "integrative", in this context, is a euphemism for quackery).

The speakers are listed on the left, as they were when I first noticed the conference in December 2012. On the right are the speakers as of February 2013,
Spot the difference
|
18 December 2012
 |
28 February 2013
 |
Yes, the one respectable oncologist on the programme, Robert Thomas, has withdrawn from the meeting.
I came across Robert Thomas because it was pointed out to me that he spoke at a meeting of YesToLife, an organisation that advocates all sorts of treatments that are unsupported by evidence. That seemed like an odd thing for a respectable oncologist to be doing, so I wrote to him, to point out some of the bizarre beliefs of his fellow speakers. Most are familiar names in made-up medicine, but probably not widely known among real oncologists.
Professor Thomas seemed unaware of this because he told me
"Thank you for your email and pointing out the vitamin C issues which of course, as you say has no scientific basis and should be outlawed along with many other practices."
Nevertheless he thought it was too late to pull out of the YesToLife meeting, so went ahead.
After this Robert Thomas wrote to me again (18 December 2012) to ask for advice about another conference he’d been invited to speak at, the Back2health event. Again he seemed unaware of the reputations of his fellow speakers, just about all of whom have a track record of advocating treatments for which there is no good evidence. Many of them are purveyors of false hope, often at a high price. I’ll deal with only three of them.
Dr Rosy Daniel is there. She’s featured several times on this blog. I met her, with Karol Sikora,here. Her course in quackery was ditched by the University of Buckingham after a year..
Chris Woollams of CancerActive is also there. As readers of this blog will know, I accept he is an honest man and I do feel a great deal of sympathy for him having lost his daughter. This doesn’t mean I am any closer to accepting his views on cancer treatment.
Next to Thomas’s picture is Barbara Wren. She was secretly filmed by the BBC claiming "to have cured thyroid cancer by applying external compresses, half an hour with castor oil and half an hour with your own urine". You can’t get much barmier than that.
Then there is a nurse, Patricia Peat, who runs a private "integrative" cancer consultancy, Cancer Options. She’s a prominent supporter of YesToLife which, since at least February 8th 2013, has been promoting a video, "Cancer is Curable Now", which makes totally irresponsible claims (and is illegal in the UK under the Cancer Act, 1939). Among other baseless treatments she has advocated high dose Vitamin C.
“The first of these people is the proprietor of Cancer Options. Cancer Options is a private consultancy offering advice to cancer patients. It is run by Patricia Peat who is a qualified nurse. My dad went to see her and she told him the good news, if he followed her advice he could be tumour free in 3 to 4 years. She advised him to have intravenous vitamin C, to have oxygen therapy, heat therapy and to take a myriad of supplements.”
I have heard that the cost of these useless recommendations over a three months would have been £4,640, plus the considerable cost of moving to Brighton, to the Vision of Hope hospital. That includes, for example, a telephone consultation (£175), supplement pills (£400) and intravenous vitamin C (£3000). There is no good evidence that any of these would help the patient. Not only would this have destituted his family and taken the patient away from them: it would also have made his last days an unnecessary misery. For Christmas he would have been condemned to a vegan diet, no wheat, sugar or alcohol, and to live on five glasses of raw juice and two jars of sprouts a day (see "Would you kick a dying man" for a real life experience).
Patricia Peat appears prominently on another web site too, Self Help Cancer. There she’s partnered by Dr Chris Etheridge (an ex biochemist, turned herbalist, with no medical qualifications). On that site you’ll find every kind of barminess endorsed. It even takes seriously the notorious Burzynski clinic about which so much has been written, both here and in the USA.
Recommending a bit of foot massage or reiki as a way to relax distraught patients is harmless enough if you like that sort of thing. Recommending you to ignore real doctors is quite another. Patricia Peat is on record as saying (my emphasis).
"Also detoxification is as important as what goes in – the rapid removal of toxins from the body would be massively beneficial in reducing the side effects. If someone is on chemotherapy, its very important to get any herbal preparations checked out by a qualified practitioner, to make sure there are no interactions, with the chemotherapy. A lot of nutritional and herbal supplements are very strong, and it is dangerous to suppose that because they are natural, they can do no harm. Probably the worst person to ask about this is your oncologist "
There is, of course, no reason to think that "detoxification" is anything other than a figment of the imagination. There is no reason to think that (never-named) toxins are important, and no reason to think that the procedures get rid of anything.
If you want sound advice about diet, go to somewhere like the American Cancer Society. There you will find that most of the things that quack nutritionists love to sell you just don’t work. The ACS asks "Will a vitamin a day keep cancer away?". Their answer is
"Can popping vitamin pills prevent cancer? The simple answer is no, based on what we know so far. In fact, some vitamin supplements have even shown harm."
The journalist, John Diamond, described movingly the way that the alternative industry moved in on him when it became known that he had cancer. His book, Snake Oil and Other Preoccupations was never finished before he died. These extracts from the foreword to the book, by Richard Dawkins, sum it up.
"When the pathologist has read the runes; when the oracles of X-ray, CT scan and biopsy have spoken and hope is guttering low; when the surgeon enters the room accompanied by ‘a tallish man … looking embarrassed … in hood and gown with a scythe over his shoulder’, it is then that the ‘alternative’ or ‘complementary’ vultures start circling. This is their moment. This is where they come into their own, for there’s money in hope: the more desperate the hope, the richer the pickings. And. to be fair, many pushers of dishonest remedies are motivated by an honest desire to help. Their persistent importunings of the gravely ill, their intrusively urgent offers of pills and potions, have a sincerity that rises above the financial greed of the quacks they promote. "
"They are targets that deserve to be hit hard, targets whose neutralisation would leave the world a better place: cynical charlatans (or honest foolish dreamers) who prey on gullible unfortunates. And the best part is that although this gallant man is dead, his guns are not silenced"
Shortly before he died, John Diamond said something that I think is one of the most perceptive comments that I’ve ever read. Some of the blame for the rise of the profitable alternative industry lies with the hype of real medicine. It’s worth quoting at length.
|
"But we expected more. Hell, we’d been promised more. Just as we’d learned, rightly, to expect that the political system could be arranged to provide a roof over the head and food in the stomach of all of us, so, we believed, could the medical system be arranged to give us all health and happiness. It was our right, dammit. And the medical establishment, flattered by all those pieces in the popular press describing the latest miracle cure which was just about —always just about — to arrive at the local surgery, joined in with the celebrations and connived with the scam. Indeed, if the boom in alternative medicine is anybody’s fault it’s that of orthodox medicine. It was the orthodoxy -helped by the media and our own vanity – which allowed us to believe that we could all be healthy and happy, that there was a pill for every problem and that if we died too early or too painfully it was an act of some agency other than capricious old God. The orthodoxy allowed us to expect And the elsewhere we looked to was the alternative practitioners. They were only too willing to take our custom . . ." |
I have no way of knowing whether the people at this conference are "cynical charlatans" or "honest foolish dreamers". I impute no motives. But I can say that their treatments are very expensive and for the most part they don’t work.
There is an interesting question about the extent to which charities like YesToLife function as charities, and the extent to which they act as agencies that channel desperate patients into the hands of private hucksters. I don’t pretend to know tha answer. I’d like to.
|
“It is difficult to get a man to understand something, when his salary depends upon his not understanding it.” |
Follow-up
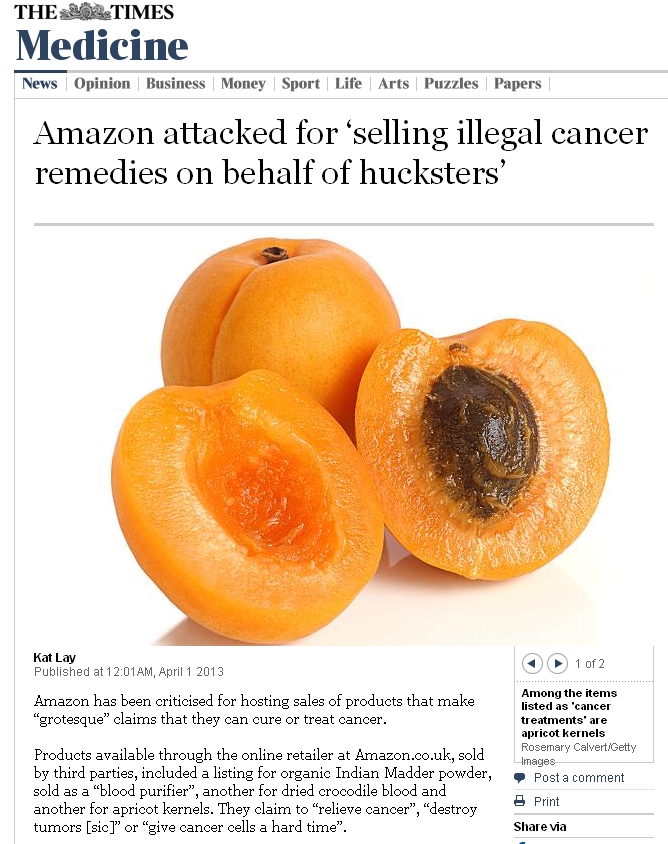
1 April 2013. The Times contacted me shortly after this came out, about some of the (illegal) nonsense to be found on sale at Amazon. One of their journalists, Kat Lay, did a good write-up, and they contacted the MHRA and stirred it into action. [download pdf].
5 April 2013. I quoted some of Patricia Peat’s views on diet from a page on Woollams’ blog. I notice that the copyright conditions on that page changed
![]()
" This content may be copied, in full or in part", has been changed to " No content may be reproduced, in whole or in part".
It’s curious that there should be an attempt to ban the reproduction of content, of which he authors are presumably proud, and which appears on a public web site. Of course it is also baseless in law, because copyright law has always allowed reproduction of parts of any document for the purposes of fair comment or in the public interest.
20 May 2012
In the USA, the first amendment allows the most outrageous claims to be made. But when they do decide the law has been broken, they do something about it. Their law enforcement is not as pathetically impotent as in the UK.
A Dr Christine Donald treated patients with cancer with an expensive herbal concoction, from her Wellness Clinic in San Fernando Valley. She promised 60 – 80% success rate. she was trusted because she was also a Pentecostal minister.
She was convicted of four counts of mail and wire fraud, six counts of tax evasion and one count of witness tampering she was found guilty of in September 2011
She was sentenced to 14 years in jail and a fine of $1.2 million.
One wonders why that never happens in the UK
26 May 2013 I noticed another incredible assertion by Patricia Peat.
“One could be forgiven for thinking how does anyone manage to die from cancer when the answers to curing it are actually so simplistic and one dimensional.”
So that’s solved, then.
10 June 2013.
I have just come across a good source of information about all sorts of alternative cancer treatments. "CAM-Cancer" was originally funded by the European Commission (EC) within the Framework 5 Programme, it is now hosted by the National Information Center for Complementary and Alternative Medicine (NIFAB) at the University of Tromsø, Norway.
The bulletin of the British Pharmacological Society, Pharmacology Matters, declined to publish the following article. Sadly the Society seems to be more interested in "reputation management" than in truth. Luckily, it is not easy to suppress criticism these days. A version of the article has appeared in Research Fortnight where it will be seen by far more people than it would have been in Pharmacology Matters. This is the original version that I submitted to them. They would not allow me to quote Lewis’s comment (apropos of the sale of homeopathic meningitis vaccine)
“Children will be harmed by this inaction. Children will die. And the fault must lie with Professor Sir Kent Woods, chairman of the regulator [MHRA].”
If a child were to die of whooping cough or meningitis as a result of buying the fraudulent "vaccines", that would be true. It’s a sad reflection on the state of defamation law that journals are not willing to say so. Blogs are fast becoming the best source of reliable information.
|
|
|
Stop press. The BPS has now signed up to Alltrials (too late for the printed version)
Pharmacology society does little to defend its subject
David Colquhoun
Over the past few years a courageous group of writers, researchers and activists has worked to expose the truth about the medicines we are sold, be they conventional or alternative.
Thanks, above all, to Ben Goldacre (1), more people than ever know that the big pharma companies have been concealing evidence of the harm that their products do, or the good they fail to do. Thanks to a small army of bloggers the preposterous claims made by peddlers of homeopathic remedies and other quackery are less likely to go unchallenged.
And yet, the organization charged with safeguarding the good name of pharmacology in this country, the British Pharmacological Society (BPS), has remained silent throughout.
The pharmaceutical industry
The BPS, rather than helping, became actively complicit when, along with much of the medical establishment, it signed an agreement with the ABPI (2). This document, developed under the aegis of the Ethical Standards in Health & Life Sciences Group (ESHLSG), contained two objectionable clauses:
“Industry plays a valid and important role in the provision of medical education”
And
“Medical representatives can be a useful resource for healthcare professionals”
Given that clinical “education” has long been part of Pharma’s marketing strategy, this seems disgraceful. And most of the doctors I know and respect refuse to see reps altogether. It is hopelessly optimistic to think that can an industry person can teach clinical pharmacology without bias in favour of his own company’s products. The BPS has many members who teach pharmacology. Can they really cope so badly that we need to have industry to educate clinicians?
It’s fine, and sometimes desirable, for academics and industry to work together on drug development. But only as long as the industry partner has no say in how, or whether, the results are published. Without that proviso we can expect more corruption of the sort that’s been seen at the University of Sheffield (3).
This is very sad, because I have great reason to like the drug industry. I’ve benefitted from several of their products myself. But the industry is in trouble. Many of its products provide only marginal benefits. Furthermore, some of the things that seemed to be useful, like SSRI antidepressants, have turned out to be next to useless once hidden trials were revealed (4). The MHRA’s learning module on SSRIs doesn’t seem to have caught up with this yet.
Sadly, the reaction of industry has been to resort to dishonesty, to hide unfavourable data and to increase yet more what it spends on marketing. Between 2009 and 2012, fines of at least 10 billion dollars (5) have been imposed on some of the most eminent companies. They include Lilly, Pfizer, AstraZeneca, Merck, Abbott and GlaxoSmithKline (GSK). The biggest fine of all ($3 bn, in July 2012) went to a British company, GSK. This succession of large fines seems to be regarded by the companies as mere marketing expenses.
All these fines were levied in the USA. Where, one might ask, are the regulators in the UK? Why have there been no fines here? Why, indeed, are some of the senior managers of these companies not in jail? Why has the BPS remained silent about the prostitution of its subject? And why have the MHRA done so little to stop it?
I suggest that you support the petition for release of the results of all trials (6). It’s been supported by many individuals and a lot of organisations, including the BMJ and the Royal Statistical Society. But, disgracefully, not by the BPS.
Quackery
At least in the case of the pharmaceutical industry some of its products work. But pharmacologists should also be concerned about the quackery industry, worth about 60 billion dollars per year (as opposed to $600 bn for the pharmaceutical industry). Virtually none of their products work (7). Why has the BPS said so little about it? It has, along with most of the medical and university establishment, shrugged its shoulders about the fact that students at Westminster University have been shown dowsing with a pendulum as a method for selection of herbal “remedies”, as part of a Bachelor or “Science” degree. It is an area in which every regulatory agency has failed to ensure even minimal levels of honesty (8). And the BPS has just shrugged.
The MHRA has been worse than useless in this area: it has been actively unhelpful (9). The senior staff of the MHRA are members of the BPS which has, as usual, said next to nothing. The MHRA’s herbal medicine committee has allowed misleading labels that give indications to be put on herbal potions, and these labels fail to make it clear that no evidence whatsoever of efficacy is required to get the MHRA kitemark. The wording was suggested (not required) by European law, but that law does not prevent the MHRA from saying, as it should, “there is no reason to think that this product is effective for any of the indications on the label” (10). Arguably, the MHRA is in breach of Consumer Protection law (11, 12).
At the time, the BPS did make some objection to the labelling (13), but only under great pressure from me (indeed I wrote it) . That has not been followed up, and I can no longer find it on the BPS web site. Indeed Philip Routledge, one of the people who is responsible for the misinformation in his capacity as chair of the MHRA Herbal Medicines Advisory Committee, is, at present the president of the BPS.
The MHRA has also been responsible for misleading labelling of the products of the most obviously fraudulent products of the lot: homeopathic pills, the medicines that contain no medicine. Most of the pills (anything beyond 12x dilution) contain not a single molecule of the substance on the label. Yet they have been given a get-out clause that enables them to evade prosecution by Trading Standards (an organisation that consistently fails to apply consumer protection laws. Rose et al (2011) (12) concluded
"EU directive 200s5/29/EC is largely ineffective in preventing misleading health claims for consumer products in the UK".
It is simply bizarre that the people at the MHRA, many of who are BPS members, have sat round a table and approved the following label. This example is for Arnica 30C pills, which, of course, contain no trace of arnica (14, 8). The outcome of their deliberations is simply surreal (see the actual labels here).
"Used within the homeopathic tradition for the symptomatic relief of sprains, muscular ache; and bruising or swelling after contusions."
This will deceive the naïve into thinking that it will have some effect on sprains etc. It won’t. And the MHRA have declined to test how the label is perceived by the public, though it took some effort to get them to admit it.
"If you are allergic to any of the ingredients in this medicine, consult your doctor before taking this medicine."
The ingredients aren’t stated apart from “contains lactose and sucrose”. That’s all they contain. No arnica.
"If pregnant or breastfeeding consult your doctor before use."
Why should a few mg of lactose and sucrose have the slightest effect on a pregnant or breast-feeding mother. This is pure make-believe
"If you forget to take this product, continue to take your usual dose at the usual time, it does not matter if you have missed a dose. Do not take a double dose to make up for a missed dose."
This statement is even more bizarre. There is nothing in the pills.
"If you take too much of this product (overdose) speak to a doctor or pharmacist and take this label with you."
And this is the ultimate in nonsense. The 1023 campaign regularly swallows whole bottles, and of course nothing happens. You can’t overdose on nothing. The fact that the MHRA can insist on this label, with a straight face, is the ultimate betrayal of science and reason.
"When asked to comment, as part of the consultation on these rules, this was the response from the BPS."
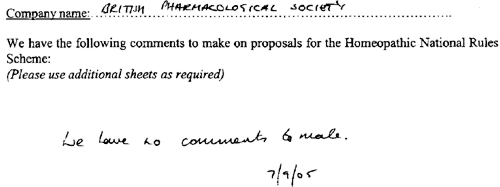
This is extracted from page 16 of the “selected response” provided by the MHRA under a Freedom of Information Act request [download all]
Things have changed little since A.J. Clark wrote his book on Patent Medicines in 1938 (15). And the BPS has done next to nothing to help. Neither has the MHRA. In fact both have colluded in the failures of both honesty and reason.
A BBC South West program recently revealed that a pharmacist was selling “homeopathic vaccines” for whooping cough and meningitis (16). The MHRA have know about his homicidal practice for years, but have done nothing. The General Pharmaceutical Council let him off with a rap on the knuckles. It has been left to bloggers and TV reporters to focus attention on these scoundrels. The well-respected blogger, Andy Lewis, wrote (17)
“Children will be harmed by this inaction. Children will die. And the fault must lie with Professor Sir Kent Woods, chairman of the regulator [MHRA].”
And the full clinical data for Tamiflu are still being concealed by Roche (18).
I think that is rather shameful.
I have been a member of the BPS for all my working life. I was happy when they made me an honorary fellow. But I now find myself asking if I can remain a member of an organisation that has done so little to defend honest scientific behaviour.
References
(1) Ben Goldacre’s Bad Pharma. Buy it now. Then do something. https://www.dcscience.net/?p=5538
(2) ABPI 2012 Guidance on collaboration between healthcare professionals and the pharmaceutical industry. http://www.abpi.org.uk/our-work/library/guidelines/Pages/collaboration-guidance.aspx
(3) Colquhoun, D. (2007) The Corporate Corruption of Higher Education: part 2 https://www.dcscience.net/?p=193
(4) Kirsch,I., B.J.Deacon, T.B.Huedo-Medina, A.Scoboria, T.J.Moore, and B.T.Johnson. 2008. Initial severity and antidepressant benefits: a meta-analysis of data submitted to the Food and Drug Administration. PLoS. Med. 5:e45. http://www.plosmedicine.org/article/info:doi/10.1371/journal.pmed.0050045
(5) Groeger, L. (2012) Big Pharma’s Big Fines http://www.propublica.org/special/big-pharmas-big-fines
(6) All trials registered. All results reported, http://www.alltrials.net/supporters/
(7) Singh,S. and E.Ernst. 2009. Trick or Treatment. Corgi. http://en.wikipedia.org/wiki/Trick_or_Treatment
(8) Colquhoun, D. (2012) Regulation of alternative medicine: why it doesn’t work, and never can. https://www.dcscience.net/?p=5562
(9) Colquhoun, D, (2006) The MHRA breaks its founding principle: it is an intellectual disgrace. https://www.dcscience.net/?p=32
(10) Colquhoun, D. (2011). Why does the MHRA refuse to label herbal products honestly? Kent Woods and Richard Woodfield tell me. https://www.dcscience.net/?p=4269
(11) Colquhoun, D. (2009) Most alternative medicine is illegal. https://www.dcscience.net/?p=30
(12) Rose,L.B., P.Posadzki, and E.Ernst. 2012. Spurious claims for health-care products: an experimental approach to evaluating current UK legislation and its implementation. Med. Leg. J. 80:13-18. https://www.dcscience.net/Rose-medico-legal-2012.pdf
(13) Colquhoun, D. (2006) Learned Societies speak out against CAM, and the MHRA. https://www.dcscience.net/?p=30
(14) MHRA Arnicare Arnica 30c pillules NR 01175/0181 http://www.mhra.gov.uk/home/groups/par/documents/websiteresources/con049307.pdf
(15) Colquhoun, D. (2008) Patent medicines in 1938 and now: A.J.Clark’s book. https://www.dcscience.net/?p=257
(16) BBC South West on the evils of homeopathic "vaccines" http://www.youtube.com/watch?v=TZf9mUzI4RI
(17) Why Does the MHRA Not Close Down these Homeopaths? The regulators have known of serious problems for years, Nothing is done. http://www.quackometer.net/blog/2013/01/why-does-the-mhra-not-close-down-these-homeopaths.html
(18) Payne, D. (2012). Tamiflu: the battle for secret drug data http://www.bmj.com/content/345/bmj.e7303
Follow-up
25 February 2013 This post has some follow-up even before it appeared on Research Research. I noticed on the BPS web site a press release “BPS announces intention to sign All Trials Petition“. It was dated 20th February, but I didn’t notice it until after the printed edition went to press. It was expressed as a future intention to sign, though in fact they signed almost straight away (though over 100 organisations had already done so). That’s good. I suspect that when my old friend, Humphrey Rang, who is president elect of the BPS, takes charge, the Society may start to take its responsibilities to the public more seriously than it has in the past.
|
The MHRA, on the other hand, is still evading its self-declared job of ensuring the public that drugs work. |
|
13 March 2013. A reply to this piece appeared in red on Research Research, The British Pharmacological Society champions its science. It was written by Humphrey Rang who, as president elect of the BPS naturally felt obliged to defend its record. He defends the BPS membership of ESHLSG, but fails to mention that first the Lancet and then the BMA withdrew their support. Nor does he mention that medical students and doctors launched a campaign, BadGuidelines.org, against the agreement. The Medical Schools Council, which also signed the agreement, said "the scrutiny of the guidance has ‘identified deficiencies in the current statement". Didn’t they read it before signing? Rang says that the BPS is also working to improve the joint statement with the ABPI. That’s good, but one must wonder why the BPS signed up to the original form.
On the points about quackery, Rang sites the BPS statement on homeopathy (now vanished) but fails to mention that that statement was written by me in an attempt to wake the BPS from it’s slumbers on the matter of medicines that don’t work. But he doesn’t mention at all the matter of mislabelling of both homeopathic and herbal preparations.
Of course, the BPS does many good things. But like most organisations, it is too reluctant to speak out when it sees wrongdoing, and too reluctant to say "sorry we made a cock-up that time".
|
“In causing NHS Choices to publish content that is less than completely frank about the evidence on homeopathy, the DH have compromised the editorial standards of a website that they themselves established”. . . “. . . they have failed the general public, by putting special interests, politics, and the path of least resistance (as they saw it) before the truth about health and healthcare.” David Mattin, lately of NHS Choices |
NHS Choices is usually a good source of information for the public. But there is one exception: the information they provide about alternative medicine is poor. A Freedom of Information Act request has revealed that the attempt of NHS Choices to rewrite their pages more accurately was censored by the Department of Health in conjunction with the late Prince’s Foundation for Integrated Health. The Department of Health (DH) has misled the public.
The earliest version of the homeopathy information page recorded by the Wayback Machine was November 12 2007. It was still there on December 5 2010. The comments were mostly critical. One said, quite correctly,
|
I find it most regrettable that the way NHS has covered this subject is to give uncritical voice to the claims of homoeopathy without giving readers the information they need to evaluate those claims. To refer readers to the websites of the British Homeopathy Association is like settling the question of the shape of planet by a reference to the website of the Flat Earth Society |
There were a lot of complaints, and to the credit of NHS Choices, the page vanished. Throughout 2011, and up to October 2012 the information page on homeopathy read
|
Introduction Content on homeopathy has been removed from the website pending a review by the Department of Health policy team responsible for complementary and alternative medicines. Homeopathy is not part of mainstream medicine. Instead it is defined as a complementary or alternative medicine. If you are considering using homeopathy, talk to your GP first. For more information about homeopathy see the House of Commons Science and Technology Committee report on homeopathy published on 8 February 2010 and the Department of Health response to that report published in July 2010 (PDF, 69KB). |
Then, at the end of 2012, the page reappeared. It was a bit better than the original, but not much. Many of the comments criticise the misleading nature of the information (as well as the usual “it worked for me” comments). The “useful links” still has six links to flat-earth organisations like the Society of Homeopaths, and only one to a sensible source, the excellent pamphlet from Sense about Science. They do link at the end to the 2010 Science and Technology Committee Report: Evidence Check 2: Homeopathy (PDF, 1.61Mb), and to the Government Response to the Science and Technology Committee Report, Evidence Check 2: Homeopathy (PDF, 69kb) but no comment is made on the findings.
Policy-based evidence
I wondered why the NHS Choices page, after an absence of almost two years, had returned in such an unsatisfactory form. So I asked them. After a reminder, I was told that my queries were being dealt with not by NHS Choices, but had been referred to Dr Sunjai Gupta “the DH official with responsibility for this area”. Dr Sunjai Gupta OBE is Deputy Director of Public Health Strategy and Social Marketing, Department of Health.
Dr Gupta is not obviously sympathetic to woo. It’s hard to tell since he doesn’t seem to have published much. But one is not reassured by an article that he wrote for the Journal of Holistic Healthcare. It appears straight after an article by fantasy herbalist, Simon Mills.
Despite assurances that I’d hear from Dr Gupta shortly, nothing happened. So I sent a request for the correspondence under the Freedom of Information Act (2000). Although the request was addressed to NHS Choices, a public body, strenuous efforts were made to divert it to the Department of Health. These were resisted. Nevertheless when, after a long delay, the material arrived, it came not from NHS Choices, but from DH, who had evidently vetted it,. The emails were rather shocking [download all].
A mail dated 1 December 2009 said

This is the most direct statement I’ve seen that, in the Department of Health, policy dictates evidence. NHS Choices is meant to provide evidence, but what they say has to be checked by DH to make sure they “don’t clash with any policy messages”.
The re-written page
The original version of the re-written page was sent to me by David Mattin, who worked for NHS Choices until September 2012. You can download the whole draft here. It is an enormous improvement on the original page. For example, it says
|
“Does it work?
Many independent experts would respond to this question ‘no, homeopathy does not work’ There is no good quality clinical evidence to show that homeopathy is more successful than placebo in the treatment of any type of condition. Furthermore, if the principles of homeopath were true it would violate all the existing theories of science that we make use of today; not just our theory of medicine, but also chemistry, biology and physics. |
This original draft was sent to Mattin on 29 January 2010. After editing it for length Mattin sent it to DH for approval. Over the next two years, DH removed much of the accurate content. Mattin’s own comments on this evisceration are reproduced below.
The DH emails
All the names have been redacted. Needless to say, nobody is willing to take responsibility. But the number of people who support magic medicine is really quite small so the main players were easy to identify.
During the nearly 2 year absence of the homeopathy page, dozens of changes were made by DH. It seems that the policy message with which the NHS Choices draft failed to comply were those of the Prince’s Foundation for Integrated Health, and its successor (after April 2010), the College of Integrated Health, now known as the College of Medicine.
NHS Choices sought advice about their redrafted pages from the right person, Sir Iain Chalmers, one of the founders of the Cochrane Collaboration. On 3 Nov 2009, Chalmers advised
The most reliable source in the country - and one of the most reliable in the world - is Professor Edzard Ernst, professor of Complementary Medicine at the Peninsular Medical School, |
Ernst returned his suggestions in July 2010, but it seems that few of them survived the subsequent 18 months of revisions by DH.
On 2 December 2009, a mail from the NHS headquarters (Quarry House, Leeds) was sent to NHS Choices
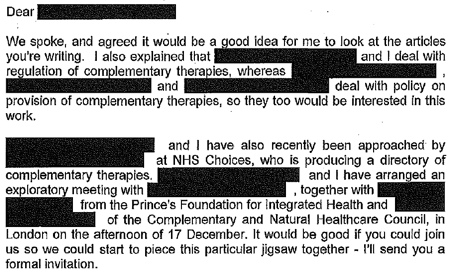
This makes it perfectly clear that DH regards the Prince’s Foundation, and the equally flaky Complementary and Natural Healthcare Council (CNHC: known on the web as Ofquack) as appropriate guides for public health policy. The fact of the matter is that regulation of magic medicine by the government has been a total disaster, because, it seems, DH regards the Prince of Wales as a reliable source.
On 29 December 2009, the Prince’s Foundation went on the attack.
On 10th January 2010, two more letters were sent to DH by the Prince’s Foundation. At 13.48 they wrote
And at 22.14 on the same day, it was followed up with
The references to Devon and to Thought Field Therapy, make it very obvious that these letters were written by Dr Michael Dixon OBE, who was medical director of the Prince’s Foundation, and who is now a director of the “College of Medicine”. And the object of Dixon’s bile is obviously Edzard Ernst (the quotation is from his book, Trick or Treatment).
I find it fascinating to see just how venomous quacks become when the evidence contradicts their views. The cuddly “holistic” veneer quickly vanishes.
It gets worse. On 21 January 2010, a mail from NHS Choices to DH said
The only person in the country who fits this description is the (in)famous George Lewith. It is simply mind-boggling that DH regards him as an appropriate person to advise on anything.
After that, NHS Choices kept asking DH to sign off the documents, and changes continued to be made. Almost two years later, DH were still stalling.
The admission that “We are a bit short of doctors within DH these days” is interesting.
A bit short of anyone capable of critical thinking would be more accurate.
The most interesting document that I got from DH was an intermediate draft of the rewritten page on homeopathy (undated). Download the document. Here are a couple of extracts.
It’s a story of two years of meddling and procrastination. The end result misinforms the public.

Right at the start, the NHS Choices draft says, reasonably enough
A House of Commons Science and Technology Committee report said that homeopathic remedies perform no better than placebos and that the principles on which homeopathv is based are “scientifically implausible”.
But a comment, added apparently by DH, says
Can we remove this statement? This report is really quite contentious and we may well be subject to quite a lot of challenge from the Homeopathic community if published.
What on earth? The DH seems to think that that its job is not to present the evidence, but to avoid challenges from the homeopathic community! And true enough, this piece is missing from the final version.
A bit later, the NHS Choices draft was censored again

“A 2010 Science and Technology Committee report said that scientific tests had shown that homeopathic treatments don’t work”
But again this doesn’t appear in the final version. The comment, apparently from DH, says
“The DH response to this report (point 24) doesn’t support this statement though”
That’s a gross distortion of point 24, which actually concludes
“The Government Chief Scientific Adviser cannot envisage scientifically credible proposals for funding for research into homeopathy in the future”
NHS Choices was not happy with the result
Shortly before the revised page was published, Paul Nuki, Editor in Chief of NHS Choicea, sent an email to DH.
|
Date: 7th September 2011 Time: 3:33:42 pm Hi I’ve been through the CAM articles and asked that we publish them asap as requested. For the record, we will be publishing these pieces outside of the normal editorial process. Although originally signed off by a suitably qualified clinician, the time lapse and policy changes have been so substantial as to render that null and void. We also don’t have a formal |
It doesn’t need much reading between the lines to see that he was unhappy with the result. It will be interesting to see whether the Information Standard people at the Royal Society for Public Health do anything about it.
The Department of Health has not just ignored evidence but actively opposed it.
That’s the only possible conclusion from the documents that I was sent. And it’s pretty shocking that the DH has preferred advice from the Prince’s Foundation and its handful of acolytes (in particular Michael Dixon and George Lewith) to the findings of the Science and Technology Select Committee and the views of the Chief Scientific Advisor.
In January this year, the Chief medical Officer, Dame Sally Davies, said, in a rare outburst of candour
|
‘I’m very concerned when homeopathic practitioners try to peddle this way of life to prevent malaria or other infectious disease,” she said. “I am perpetually surprised that homeopathy is available on the NHS.” Dame Sally, who is England’s most senior doctor, concluded by remarking that homeopathy “is rubbish”. |
 |
So one part of DH is working to contradict another part. the Chief Medical Officer. Perhaps Sally Davies should have a word with Dr Gupta.
This all predates the advent of Jeremy Hunt (and known defender of homeopathy) as health minister. But the sympathies of some DH people are made obvious by the presence on the DH web site of an article “Personal health budgets: A new way of accessing complementary therapies?”. This astonishing piece confirms the worst fears that quacks will see personal health budgets as a commercial opportunity to peddle their wares. The article is by Jim Rogers of Lincoln University. What his paper does not mention is Rogers’ conflict of interest. He’s a homeopath, and he has a paper in the International Journal of High Dilution Research (yes, there is a journal for every form of make-believe). You can download a reprint of this paper. It advocates more research into homeopathic provings, something that even George Lewith seems to have given up on.
It’s about time that the DH started to listen to the Chief Medical Officer. As it is, some people at DH seem to prefer the advice of the Prince’s Foundation, and to actively suppress employees who prefer evidence to anecdote.
One thing is clear. The DH is an unholy mess. Parts of it are intent on producing policy-based evidence.
Comment by David Mattin, who edited the first draft for NHS Choices
David Mattin left NHS Choices in September, 2012. He edited the new version and lived through the two years of wrangling with DH during which much of the best content was eviscerated. He sent me this statement about the affair.
|
As an editor at NHS Choices, I viewed it as my job to present evidence-based information to the public. The article we prepared on homeopathy stayed true to that central purpose: it made clear to readers that there is no good quality evidence that homeopathy is an effective treatment for any health condition, and also presented the broad scientific consensus that the supposed method of action of homeopathy is implausible.
What followed was a two year story of delay, and eventual suppression, of that article. My strong impression was of DH civil servants who lacked the courage, and, frankly, the energy to stand up to the criticism from special interest groups that they anticipated would arise because of the article; and that did indeed arise when a draft of the article and other draft content on complementary and alternative medicines fell into the hands of the Prince’s Foundation and other CAM groups.
The attitude of DH civil servants, broadly, was simply to tell us ‘we can’t say this about homeopathy, people will complain’. They seemed to have no interest in making an appraisal of the evidence on homeopathy themselves to see if what we were saying was actually true or not. We repeatedly pushed back with the message: ‘some people may very well complain, but if what we are saying about the evidence base is true – and it is – then we must simply weather those complaints, and stand by our content. Our duty is to supply our readers with the best information, not to please the homeopathy community.’ But these arguments were disregarded. The DH civil servants were almost entirely concerned with the politics of the situation – that is, the politics as they saw them – and the possibility that this article may create new work for them, and very little concerned with the evidence itself, or the presentation of this evidence to the public.
The whole episode is an insight into the way special interest groups can influence the workings of government and the public sector simply by making a lot of noise, and having a few powerful friends. In causing NHS Choices to publish content that is less than completely frank about the evidence on homeopathy, the DH have compromised the editorial standards of a website that they themselves established, and that they fund. They have sold out the NHS Choices editorial team, who work tirelessly to fulfil their remit. And, most seriously, they have failed the general public, by putting special interests, politics, and the path of least resistance (as they saw it) before the truth about health and healthcare.
|
Follow-up
13 February 2013 The Guardian version of this story, written by Sarah Boseley, is Prince’s charity lobbied government to water down homeopathy criticism. It’s fine as far as it goes but it doesn’t name any names. There are some good comments though.
14 February 2013. The printed Guardian gave the story full 5 column-width coverage. [download print version]

And news has reached the USA: there’s an account of the affair on the Neurologica blog: Politics trumping science at the NHS.
On 14 February, the Guardian version was Editor’s Choice by lunchtime, and the Guardian web version already had 414 comments, mostly sensible (though this blog got far more referrals from twitter than from the Guardian)

And news has reached the USA: there’s an account of the affair on the Neurologica blog: Politics trumping science at the NHS.
15 February 2013. The Daily Mail had very fair coverage of the story.

The Guardian closed the comments on the story when it had got 642 comments, most of them very sensible. And this page got almost 6000 hits in 24 hours. The majority of the referrals came from Twitter rather than from the Guardian, despite the direct link to the page from the Guardian.
18 February 2013. The affair featured in BMJ News [download the reprint]. The item featured prominently on the BMJ news page.
![]()

19 February 2013 Only six days of this post, the NHS Choices page has been re-written again, in a much improved form. That looks like bloggers 1, DH 0. It is baffling that it’s left to bloggers, working for nothing, to extract a bit of sense from the highly-paid civil servants at the Department of Health. But at least they listened this time, which is a lot more than happens often. Paul Nuki, who runs NHS Choices, deserves congratulations. Of course the revised page still doesn’t call a spade a spade, but it gets close at times. I like the way it starts "Homeopathy is a ‘treatment’ based". Notice the quotation marks.
Reputation management?
Incidentally, NHS Choices is outsourced to the (in)famous company, Capita. And the moderation of the comments on their site is outsourced again to Tempero, which describes itself as a "reputation management" company. Each of them creams off money meant of patient care. This discovery might explain why I and others have had comments rejected by NHS Choices several times. "Reputation management" is the antithesis of evidence. It is public relations, i.e. paid lying. That is quite wrong for a site that is meant to provide dispassionate information.
21 February 2013. Sadly a step backwards. Part of the improved page was removed. This bit.
The Chief Medical Officer, Professor Dame Sally Davies, has said there is no scientifically plausible way that homeopathy can prevent or cure diseases. She has made it clear she is particularly concerned about the use of homeopathy in developing countries as a so-called cure for malaria.
We can only speculate why this was removed, because it was true. In fact she accurately described homeopathy as "rubbish". Why she should not be quoted beats me.
It must be admitted that the human genome has yet to live up to its potential. The hype that greeted the first complete genome sequence has, ten years on, proved to be a bit exaggerated. It’s going to take longer to make sense of it than was thought at first. That’s pretty normal in science. Commerce, though, can’t wait. Big business has taken over and is trying to sell you all sorts of sequencing, with vastly exaggerated claims about what you can infer from the results.
There are two main areas that are being exploited commercially, health and ancestry. Let’s look at an example of each of them.
Private health screening is wildly oversold
There has been a long-running controversy about the value of screening for things like breast cancer. For a superb account, read Dr Margaret McCartney’s book, "The Patient Paradox: Why sexed-up medicine is bad for your health", “Our obsession with screening swallows up the time of NHS staff and the money of healthy people who pay thousands to private companies for tests they don’t need. Meanwhile, the truly sick are left to wrestle with disjointed services and confusing options”.
Many companies now offer DNA sequencing. It’s become so bad that a website, http://privatehealthscreen.org/ has been set up to monitor the dubious claims made by these companies. It’s run by Dr Peter Deveson, Dr Margaret McCartney, Dr Jon Tomlinson and others. They are on twitter as @PeteDeveson, @MgtMcCartney, @mellojonny. They explain clearly what’s wrong. They show examples of advertisements and explain the problems.
Genetic screening for ancestry is wildly-oversold
Many companies are now offering to tell you about your ancestors on the basis of your DNA. I’ll deal with only one example here because it is a case where legal threats were used to try to suppress legitimate criticism. The problem arose initially in an interview on BBC Radio 4’s morning news programme. Play the interview.
Today. I should make it clear that I’m a huge fan of Today. I listen every morning. I’m especially enthusiastic when the presenters include John Humphrys and James Naughtie. The quality of the interviews with politicians is generally superb. Humphrys’ interview with his own boss, George Entwhistle, was widely credited with sealing Entwhistle’s resignation. But I have often thought that is not always as good on science as it is on politics. It has suffered from the "false balance" problem, and from the fact that you don’t get to debate directly with your opponent. Everything goes through the presenter who, only too often, doesn’t ask the right questions.
These problems featured in Steve Jones’ report on the quality of BBC Science reporting, which was commissioned by the BBC Trust, and reported in August 2011. The programmes produced by science departments are generally superb. Just think of the Natural History Unit and David Attenborough’s programmes. But the news departments are more variable. One of Jones’ recommendations was that there should be an overall science editor. In January 2012, David Shukman was appointed to this job. But it seems that neither Shukman, nor Today‘s own science editor, Tom Feilden, was consulted about the offending interview.
My knowledge of genetics is not good enough to provide a critical commentary. But UCL has world-class experts in the area. The account that follows is based mainly on a draft written by two colleagues, Mark Thomas and David Balding.
Vincent Plagnol has posted on Genomes Unzipped a blog that explains in more detail the abuse of science, and the resort to legal threats by a public figure to try to cover up his errors and exaggerations.
|
The interview was with the Rector of St Andrews University, Alastair Moffat, who also runs several businesses, including Britains DNA, Scotlands DNA, Irelands DNA, and Yorkshires DNA.
|
 “Inside all of us lies a hidden history, the story of an immense journey told by our DNA.” |
All four sites are essentially identical (including lack of apostrophes. These companies will, for a fee, type some genetic markers in either the maternally-inherited mtDNA (mitochondrial DNA), or the male-only Y chromosome, and provide the customer with a report on their ancestry.
We’ll come back to the accuracy of these reports below, but as a preliminary guide, consider some of the claims made by Moffat on the BBC Radio 4 Today programme on July 9, 2012:
- there is scientific evidence for the existence of Adam and Eve
- nine people in the UK have the same DNA as the Queen of Sheba
- there is a man in Caithness who is “Eve’s grandson” because he differs by only two mutations from her DNA
- 33% of all men are extremely closely associated with the founding lineages of Britain
- we found people that have got Berber and Tuareg ancestry from the Saharan nomads
There was a persistent theme in the interview that DNA testing by Moffat’s company was “bringing the Bible to life” — of course their activities neither support nor detract from anything in the Bible. If you want to either laugh or cry at the shocking range of errors and exaggerations in the interview, listen to it yourself and then read the Genomes Unzipped blog. For example, Piagnol points out that::
"A bit of clarification on chromosome Y and mtDNA: these data represent only a small portion of the human genome and only provide information about the male (fathers of fathers of fathers…) and female (mother of mothers of mothers…) lineages. As an illustration, going back 12 generations (so 300 years approximately) we each have around 4,000 ancestors. mtDNA and chromosome Y DNA only provide information about 2 of them. So these markers provide a very limited window into our ancient ancestry."
Of most concern is that Moffat’s for-profit business was presented as a scientific study in which listeners were twice invited to participate. He admitted that they have to pay but “we subsidise it massively”. This phrase is important because it suggests that this is a genetic history project of such importance and public interest that it has been subsidised by the government or a charitable body. This doesn’t seem plausible – Britains DNA charges £170 for either mtDNA or Y typing, which is comparable with their competitors. There is nothing on the Britain’s DNA website to indicate that it is subsidised by anybody.
Instead of producing evidence, Moffat paid a lawyer to suppress criticism
When challenged by my two academic colleagues, Mark Thomas and David Balding, on this and other problems arising from the interview, Moffat failed to either clarify or withdraw the "massively subsidised" claim. Instead, his two challengers received letters from solicitors threatening legal action for defamation unless they fulfil conditions such as that they will not state that Mr Moffat’s science is wrong or untrue. In the face of so many obvious dubious claims in the Today interview, it would be a dereliction of the duty of an academic not to point out what is wrong.
The interview certainly sounded exaggerated to me. Luckily, a colleague of Thomas and Balding, Vincent Plagnol (lecturer in statistical genetics), has written a detailed refutation of many of Moffat’s claims on his post Exaggerations and errors in the promotion of genetic ancestry testing, on the Genomes Unzipped blog.
Thomas and Balding maintain that oversimpliifed and incorrect statements appear also on the web site of Britains DNA.
The interview sounded more like advertising than science
It is clearly unacceptable for a person in high public office to make a claim on national radio that appears to be untrue and intended to support his business interests, yet to refuse to withdraw or clarify it when challenged.
Complaints were made both by Thomas and Balding to the BBC, but they met with the usual defensive reply. The BBC seemed to be more interested in entertainment value than in science, in this case.
A few more aspects of this story are interesting. One of them is the role of Moffat’s business partners, Dr Jim Wilson of Edinburgh University and Dr Gianpiero Cavalleri of the Royal College of Surgeons in Ireland. It was these two academics to whom both Thomas and Balding sent emails about their concerns. And it was these emails that elicited the legal threat. They refused to clarify the “massively subsidised” claim, and they have not publicly disassociated themselves from the many misleading statements made by Moffat, from which as business partners they stand to benefit financially (they are both listed as directors and shareholders of The Moffat Partnership Ltd at Companies House). They have both responded to Thomas and Balding, misrepresenting their statements in a way that would support legal action.
Did James Naughtie think his interview was entertainment, not science?
Another interesting but depressing aspect to the story is the role of the BBC’s interviewer Jim Naughtie. In the face of the most outrageous claims about Eve, the Queen of Sheba and "bringing the Bible to life”, that a moment’s thought would have suggested can’t be true, Naughtie asked no sceptical, challenging or probing question. He even commented twice on individuals having "pure" DNA, which is appalling: nobody’s DNA is any purer than another’s; has he not heard of eugenics? Naughtie gave Moffat two opportunities to promote his business, even with details of the web address.
It turns out that Naughtie and Moffat are old friends: as Chancellor of the University of Stirling, Naughtie invited Moffat to sit on its Court, and he posted on YouTube a short video of him supporting Moffat’s campaign for Rector of St Andrews. No such connection was mentioned during the interview.
This interview is not the first. Naughtie also interviewed Moffat (broadcast on 1st June 2011) about a rather silly exercise in claiming – on the basis of Y-chromosome data – that Jim Naughtie is an Englishman . Again Naughtie gave Moffat ample opportunity to promote his business and as far as I am aware none of Moffat’s commercial rivals has been given any comparable opportunity for free business promotion on the BBC.
No suggestion is being made that there is anything corrupt about this. Naughtie is not a scientist, and couldn’t be expected to challenge scientific claims. The most likely interpretation of events is that Naughtie thought the subject was interesting (it is) and invited a friend to talk about it. But it was a mistake to do this without involving Today‘s science editor, Tom Feilden, or the new BBC science editor, David Shukman, and especially to fail to invite a real expert in the area to challenge the claims. There are lots of such experts close to the BBC in London.
Many other companies cash in on the ancestry industry.
Britains DNA is only one of many genetic ancestry companies that make scientifically unsupported claims about what can be inferred from Y chromosome or from mtDNA variants about an individual’s ancestry. This is a big industry, and arouses much public interest, yet in truth what can reliably be inferred from such tests is limited.
Our number of ancestors roughly doubles every generation in the past, so the maternal-only and paternal-only lineages rapidly become negligible among the large numbers of ancestors that each of us had even just 10 or 20 generations ago. Because migration is ubiquitous in human history, those ancestors are likely to have had diverse origins and the origins of just two of them (paternal-only and maternal-only lineages) may not give a good guide to your overall ancestry. Moreover if you have a DNA type that is today common in a particular part of the world, it doesn’t follow that your ancestors came from that location: such genetic tests can say little about where your ancestors were at different times in the past.
Faced with these limitations, but desiring to sell genetic tests, many companies succumb to the temptation to exaggerate and mislead potential clients about the implications of their tests, in some cases leading to disappointed clients who feel betrayed by the scientists in whom they placed trust.
If you have a few hundred pounds to spare, by all means get yourself sequenced for fun. But don’t imagine that the results will tell you much.
Follow-up
25 February 2013, Mark Thomas follwed up this post in the Guardian
“To claim someone has ‘Viking ancestors’ is no better than astrology. Exaggerated claims from genetic ancestry testing companies undermine serious research into human genetic history”
10 March 2014
After more than a year of struggling, the BBC did eventually uphold a complaint about this affair. Full accuonts can be found on the web site of UCL’s Molecular and Cultural Evolution Lab and on Debbie Kennett’s site
Which? Magazine (the UK equivalent of Consumer Reports in the USA) has done it again. They published an excellent article, Health products you don’t need. It’s a worthy successor to their recent debunking of “nutritional therapists”. Most of the products in question, apart from Bach Rescue Remedy Spray, were not outright quackery like homeopathy or "detox" products. Rather they were old-fashioned pharmaceutical products that were quite respectable in the 1950s but which have subsequently been found not to work.

These are the things that were looked at.
- Benylin Chesty Coughs (Non-Drowsy)
- Benylin Tickly Coughs (Non-Drowsy)
- Covonia Herbal Mucus
Cough Syrup - Boots Cold and Flu Relief
Tablets - Adios Slimming Tablets
- Bio-Oil
- Seven Seas Jointcare Be Active
- Bach Rescue Remedy
Spray
It’s an interesting and large category, and its one that I grew up with. My first job, in the 1950s was as an apprentice in Timothy Whites & Taylors Homeopathic Chemists in Grange Road, Birkenhead (you can’t have a much humbler start than that). Don’t worry about he homeopathic bit. We had one homeopathic prescription in two years, which was made up with great hilarity. These were the days before the endarkenment.
We did, however, sell a lot of "tonics" and "cough medicines". Two popular brands were Metatone Tonic and Minadex Tonic. I was quite surprised to discover that they are still on sale. Even in the 1950s I was a bit sceptical about what a "tonic" was supposed to achieve. The term soon became extinct as it was slowly realised that no examples existed.
Here is the bad news. It is scarcely an exaggeration to assert the following.
- Nothing is known that alters the time course of a cold.
- There is nothing that you can buy that will suppress a cough*.
- There is no such thing as a "demulcent" or an "expectorant"
- There is no such thing as a "tonic".
- It would be nice if these things existed, but they are figments of the imagination. Nonetheless they sell by the truckload and vast amounts of money are made by selling them.
[*morphine may have a modest effect, but you can’t buy it]
How can this happen? We have the Medicines and Healthcare products Regulatory Agency (MHRA) is the government agency which is responsible for ensuring that medicines and medical devices work, and are acceptably safe.
Demulcents
In the 1950s this was a more or less respectable term. If you google it now, almost all the references come from herbalists, It is, almost entirely, part of the world of quackery. Apart, that is, from the MHRA. And NHS Evidence. It was surprising to find, in a 2009 document from the MHRA
"Simple cough mixtures containing a demulcent, for example glycerin, and syrup can have a soothing effect by coating the throat and relieving the irritation which causes the cough"
No reference is given, and I’m not aware of the slightest reason to think that there is any such effect. Syrup in your respiratory tract is a bit of a disaster.
But the same document says
There are severe limitations to the efficacy studies given that many of the products were first introduced decades ago. There has been no co-ordinated development program to establish efficacy. What trials there are have not been carried out to current standards.
There isn’t much detail about these old ‘remedies’ on the MHRA site. I did find a Publiic Assessment Report for Benylin Mucus Cough Menthol Flavour Oral Solution. The main ingredient is Guaifenesin
The assessment says this.
And the approved label says this.
The Public Assessment Report also says
Efficacy
Guaifenesin . . . is a well-established medicinal product with well-known efficacy and safety profiles
This appears to be pure make-believe. There is no credible evidence for any such effect. The report may be dated 2012, but it is a carry-over from a previous age.
In 1976, it was pointed out that none of these things worked (Ziment, 1976), and the situation hasn’t changed. Ziment’s review concludes
"Perhaps this is the one disease that could truly benefit from that oft-touted panacea of therapeutics, the overworked nostrum of materia medica—namely, chicken soup"
A 2012 Cochrane review agrees: "Over-the-counter (OTC) medications for acute cough". This review concludes
"We found no good evidence for or against the effectiveness of over-the-counter (OTC) medications in acute cough, which confirms the findings of two previous reviews (Anonymous 1999; Smith 1993)."
What the MHRA tell me
I was puzzled by the apparently unjustified statements on the MHRA site so I asked them about the eight products that were investigated by Which? magazine (see above). I asked them also about Metatone and Minadex "tonics"
The questions, and the responses can be downloaded here. (I merely asked some reasonable questions, but the MHRA chose to treat them as a request under the Freedom of Information Act).
The first five items all have full marketing authorisation, as do Metatone and Minadex "tonics".
"Metatone (PL-02855/0017), Covonia Herbal Mucus Cough Syrup, Cold and Flu Relief Tablets and Adios Tablets originally held Product Licences of Right. These products were on the market before the Medicines Act 1968 came into force in 1971. These licences were reviewed in the 1980s to ensure that the products were safe, of suitable quality and have evidence of efficacy. Because of the length of time that the products had been on the market they were considered to have well established use and original clinical data to today’s standards was not necessarily available."
The MHRA tell me that they have no copies of the reviews conducted in the 1980s, apart from one. They sent a scanned copy of the August 1988 expert review of Covania syrup (the ingredients have changed since than).
The document is like an antique. It simply repeats the old myths. The names of the "expert reviewers" have been hidden. Given the quality of the review, perhaps that isn’t surprising, but the MHRA should not be so secretive.
There is no such thing as a "tonic", so I asked the MHRA about that too.
Q.5 Can you tell me what criteria the MHRA uses when allowing a product to be advertised as a "tonic"?
R.5 The MHRA assesses proposed product names on a case by case basis. On the basis of the well established use of Minadex Tonic it was decided that the use of the word tonic in the product name was acceptable. For the same reason, it was accepted that Metatone could be referred to as a tonic in the Product Information Leaflet and product labels
In other words, we let them get away with it because it’s old.
I had always understood that when the MHRA grants "Marketing authorisation", that meant there was some guarantee that the product worked. You’d infer that from the MHRA’s own definition.(my emphasis)
"Medicines which meet the standards of safety, quality and efficacy are granted a marketing authorisation (previously a product licence),"
Sadly, it seems that this isn’t true, at least for old-established products, those that were on the market before the Medicines Act (1968) came into force in 1971.
Conclusion
Although old products which were on the market before 1971 were supposed to be reviewed for efficacy and safety. This hasn’t been done efficiently. The make-believe has simply been perpetuated. I have no objection to people buying benylin etc, but they should not have full marketing authorisation and they should be labelled accurately so that it is clear that there is very little evidence that they’ll do you much good. The MHRA has let down the public, just as it did when it allowed misleading labels on homeopathic and herbal potions.
Postscript
After writing this, I discovered a very recent paper about guaifenesin (Seagrave et al, 2012), This paper shows some effects on mucus secretion in cultured human cells (not in humans) with prolonged exposure to concentrations of 30 and 100 µM. This is an order of magnitude greater than the peak blood concentration (7 µM. = 1.4 µg/ml) that is achieved (transiently) in man (Maynard & Bruce, 1970). This is not mentioned in the paper. I’m sure that has nothing to do with what we read at the end of the paper.
Competing interest
JS has received research funds from Reckitt Benckiser. HHA is a consultant to Reckitt Benckiser and is the co-author of a Mucinex sustained-release guaifenesin) patent. DBH has received research funds and consultancy payments from Reckitt Benckiser. DFR has received consultancy payments from Reckitt Benckiser. GS is an employee of Reckitt Benckiser and is also a co-author of a Mucinex (sustained-release guaifenfesin) patent.Acknowledgements
This study was funded by Reckitt Benckiser Healthcare International Ltd. Assistance with manuscript submission was provided by Elements Communications Ltd, supported by Reckitt Benckiser Healthcare International Ltd.
On 15 October 2010, Reckitt Benckiser was fined £10.2 m by the Office of Fair Trading after the company admitted anti-competitive behaviour.
Follow-up
Shortly after this post went up. I was attacked on twitter by @iHealthP. That’s a company, http://www.ihealthpartnership.com (the tweeter declined to reveal their identity). It started thus.
Your article asserts that “There is nothing that will suppress a cough.” This is bollocks, pure & simple.
The interchange was one of those less pleasant Twitter moments (I’ve Storifed some of it in case anyone is interested). The discussion did throw up a few useful references though. @LeCanardNoir pointed out a 2007 paper which concludes
"Clearly the widespread notion that codeine is an effective cough suppressant is not supported by the available evidence."
One of the papers cited by @iHealthP in support of his/her contention that pholcodine and codeine work was Recommendations for the management of cough in adults (from the British Thoracic Society Cough Guideline Group). This paper actually concludes
“There are no effective treatments controlling the cough response per se with an acceptable therapeutic ratio.”
That, of course, is exactly what I said.
There was, however, one reference produced by @iHealthP for which I’m grateful. It doesn’t concern over-the-counter cough treatments (which is what this post is about), but morphine. It does, though, produce some evidence that morphine does work to some extent as a cough suppressant. Amazingly this "well-known truth" was not demonstrated until 2006. The paper, Opiate Therapy in Chronic Cough, by Morice et al., 2006. shows a convincing effect of morphine (5 or 10 mg twice a day) on chronic cough. The main caveat lies in the reported side effects: constipation (40%) and drowsiness (25%). Obvious side-effects can make the trial non-blind. In any case, none of this is relevant to the present post (though I altered the blog to refer to it).
|
Synexus is "The world’s largest multi-national company entirely focused on the recruitment and running of clinical trials company that runs clinical trials and screening programmes". |
|
I should say at the outset that I’m deeply impressed by our local GP practice. I can’t imagine a better GP than mine; he has the ideal mix of knowledge and empathy. I do, however, worry about the fragmentisation of the NHS and its creeping privatisation.
I came across Synexus because my wife had a letter (on our GP practice letterhead) inviting her to go for osteoporosis screening, and possibly to "take part in a study". Download the letter.
Notice that the form gives no idea of what the "study" might be. Notice also, more seriously, the small print on the second page of the form. Here it is in normal size print.
"If you contact Synexus and/or return the attached tear-off slip Synexus may, with your consent, use the data you provide for the purposes of informing you of the study, of medical products and processes that might be of interest to you. Your information will be held by, and access to it limited to, Synexus Ltd and/or companies within the Synexus group of companies and/or third parties acting on their behalf"
You are invited, in near-illegible small print, to allow all your medical data to be handed over to Synexus [see comment, below], and an unspecified number of other companies and third parties. It also gives the company permission to "use the data you provide for the purposes of informing you. . . of medical products and processes that might be of interest to you". This appears to mean that in the future you’ll be pestered with mailings that bypass your GP and advertise (private?) screening etc. For the purposes of screening there should be no need to hand over any data whatsoever (and the practice manager ensures me that they don’t).
My wife asked my advice about whether she should sign up for "the study" if invited to do so, so I asked the GP practice what the trial was about. Rather to my surprise, they didn’t know. Neither did Hertfordshire NHS. So I asked the National Osteoporosis Society, and they didn’t know either. After several emails and a phone call, I eventually got the details from Synexus.
I have two concerns about this. One is the argument that’s been raging about the value of indiscrimate screening, The case against it has been put perfectly in Margaret McCartney’s recent book, The Patient Paradox. There’s a good case that too much money is spent on people who are well, and not enough on those who are ill. Of course prevention is better than cure. The problem is that in many cases the screening tests aren’t accurate enough, so many people get diagnosed and treated when they are not actually ill.
On top of that, there is now a serious worry about screening tests promoted by private companies, for profit. Lifeline has been criticised, for good reasons. The men’s health charity, Movember, promotes PSA screening for prostate cancer, one of the most unreliable tests in existence. There is now a web site that collates evidence about private health screening. Many of the tests are available on the NHS, and the NHS advice about them is being re-written so that it gives information about risks as well as benefits.
The NHS advice on screening for osteoporosis is still ambiguous. The evidence for benefit of screening at age 60 is not clear.
The main question, though, is this. If my wife were offered an opportunity to "take part in a study", should she say yes, or no? My first inclination was to say yes. Clinical trials are the only way to find out whether treatments work or not. If people don’t volunteer for trials, we’ll never know. But before saying yes, one would want to know that the trial was organised properly, so that it could answer a relevant question. That’s why I was surprised when I found it so hard to discover the details. Nobody seemed to know even where the trial was registered. It’s no use searching trial registers for "Synexus": you need to know who is paying for it.
Eventually Dr John Robinson of Synexus turned out to be very helpful. The protocol number is 20070337 with a EudraCT number 2011-001456-11. The trial is registered at ClinicalTrails.gov and it has ethical approval. It’s a trial of a new osteoporosis treatment made by Amgen, AMG 785. It’s a monoclonal antibody against sclerostin, a protein that inhibits bone formation. It sounds like a good idea, but we won’t know how well it works until it’s been tested. The allocation of patients to AMG 785 or placebo is randomised and double blind. The patient Information sheet for participants looks pretty good to me.
Nevertheless, I have some reservations about the trial. First, its organisation is odd. “After taking AMG 785 or placebo for one year, all study participants will be taking denosumab for the following year”. Denusomab is another product of the same company, Amgen. It has already been approved by NICE. When I asked Dr Robinson why this arrangement had been chosen, this is what he said.
"Previous studies have shown that the maximal benefit on bone density is seen after 12 months and that treatment after this period shows a lower increase, it is for this reason treatment with AMG 785 is for 12 months in this study.
Other studies have also shown benefit in further improving and maintaining the increase in bone density and reducing fracture risk by subsequently treating patients with Alendronate after 12 months of AMG 785. This study is investigating whether similar or better findings occur with denosumab."
This does not make any sense to me. If the object is to compare AMG 785 with denusomab, they should be compared side by side, not sequentially. That brings us straight to the main problem with the trial design. It asks the wrong question. What the doctor needs to know is whether AMG 785 is more effective than existing treatments, not whether it is better than placebo. When I asked Dr Robinson about this, he said
"To quote from the protocol: A placebo-controlled study was chosen because it permits a minimally confounded demonstration of efficacy and safety of AMG 785 in the treatment of PMO. Using an active control such as a bisphosphonate means that more patients have to be enrolled to show benefit from AMG 785. The study already plans to enrol 6000 women. Increasing this number would add to the time required to complete the study. In addition the use of a placebo control is also within regulatory guidelines. "
What this means, in plain English, is that they are expecting a rather small difference between AMG 785 and existing treatments. It would take a very large number of patients to show this difference. If the difference is indeed small, it would be hard to justify the (doubtless eye-watering) cost of AMG 795 (denusomab costs £185.00 per dose). Testing a new drug against placebo, or against a low dose of something not very effective, is one of the stratagems listed in Chapter 4, Bad trials, in Ben Goldacre’s Bad Pharma. It makes the new drug look good, but it asks the wrong question.
The National Osteoporosis Society should be an organisation to which patients could turn to for advice in cases like this. In this case they were not helpful. They didn’t know much about the trial. I hope that this is not related to the fact that they get a lot of funding from Synexus. I noticed too that one of their advisors is the infamous Professor Richard Eastell, who admitted in print to lying in a paper, about a drug for osteoporosis made by Proctor & Gamble. It’s getting quite hard to find a medical charity that isn’t in the pocket of Big Pharma. or quacks (or even occasionally, both).
Conclusion. The trial asks the wrong question. On those grounds alone, I think that my advice would be not to volunteer for the trial.
Follow-up
I should have mentioned an interesting and relevant Cochrane review, New treatments compared to established treatments in randomized trials (2012), The authors’ conclusions are as follows.
“Society can expect that slightly more than half of new experimental treatments will prove to be better than established treatments when tested in RCTs, but few will be substantially better. This is an important finding for patients (as they contemplate participation in RCTs), researchers (as they plan design of the new trials), and funders (as they assess the ’return on investment’).”
15 May 2013. As noted in the comments, Synexus has been censured by the Advertising Standards Authority, because the ASA judged that they did not give sufficient prominence to the fact that there advertising of free screening was actually a way to recruit people into clinical trials.
Nobody could have been more surprised than I when I found myself nominated as an academic role model at UCL. I had to answer a few questions. It is not obvious to me what the object of the stunt is, but the person who asked me to do it seemed to find the answers amusing, so I’ll reproduce here what I said. I apologise for the temporary lapse into narcissism.
The final version has now been printed [download a copy]. Sadly the printed edition was “corrected” by someone who replaced “whom I asked to submit the first theoretical paper by Hawkes and me to the Royal Society” (as written below), with “paper by Hawkes and I”. Aaargh.
Your nomination – Why you were nominated as an Academic Role Model?
"David Colquhoun has made major contributions to our understanding of how ion channels (proteins which allow charged ions to pass across cell membranes) function to mediate electrical signalling in nerve and muscle cells. This work elegantly combines experimental and theoretical aspects, and resulted in David being made a Fellow of the Royal Society. David Colquhoun played a key role in resisting the notion that UCL should merge with Imperial College in 2002, by running a website opposed to the merger. He thus facilitated the continued existence of an independent UCL. He is also well-known for his principled opposition to therapies that are not based on scientific evidence, and for his blog which comments on this issue as well as on university bureaucracy and politics."
Role models’ questions
1. What is your response to being nominated?
Astounded.
We are interested in giving people a very brief ‘snapshot’ description of their career trajectory, to help a broad range of people see how you got to where you are:
2. What has your career path been?
|
My first job (in 1950s) was as an apprentice pharmacist in Timothy Whites & Taylors (Homeopathic Chemists) in Grange Road, Birkenhead. You can’t get a more humble start than that. But it got me interested in drugs, and thanks to my schoolmaster father, I got to the University of Leeds. |
 My father (1907 – 2001), in 1955 |
|
One of the courses involved some statistics, and that interested me. I think I made a semi-conscious decision that it would be sensible to be good at something that others were bad at, so I learned quite a lot of statistics and mathematics. I recall buying a Methuen’s Monograph on Determinants and Matrices in my final year, and, with the help of an Argentinian PhD student in physical chemistry (not my lecturers) I began to make sense of it. |

|
I purposely went into my final viva with it sticking out of my pocket. The examiner was Walter Perry, then professor of Pharmacology in Edinburgh (he later did a great job setting up the Open University). That’s how I came to be a PhD student in Edinburgh.
Although Perry was one of my supervisors, the only time I saw him was when he came into my lab between committee meetings for a cigarette. But he did make me an honorary lecturer so I could join the Staff Club, where I made many friends, including a young physics lecturer called Peter Higgs. The staff club exists no longer, having been destroyed in one of those acts of short-sighted academic vandalism that vice-chancellors seem so fond of.
The great university expansion in the 1960s made it easy to get a job. The most famous pharmacology department in the world was at UCL so I asked someone to introduce me to its then head, Heinz Schild, and asked him if he had a job. While interned during WW2 he had written a paper on the statistics of biological assay and wanted someone to teach it to students, so I got a job (in 1964), and have been at UCL ever since apart from 9 years. Between 1964 and 1970 I published little, but learned a great deal by writing a textbook on statistics.
That sort of statistics is now thought too difficult for undergraduates, and the famous department that attracted me was itself destroyed in another act of academic vandalism, in 2007.
I have spent my life doing things that I enjoy. Such success as I’ve had, I attribute to a liking for spending time with people cleverer than I am, and wasting time drinking coffee. I found a very clever statistician, Alan Hawkes, in the Housman Room in the late 1960s, and we began to collaborate on the theory of single ion channel analysis in a series of papers that still isn’t quite finished. He did the hard mathematics, but I knew enough about it to write it up in a more or less comprehensible form and to write computer programs to evaluate the algebra. When I got stuck, I would often ask Hyman Kestelman (co-author of the famous mathematics textbook, Massie & Kestelman) to explain, usually in what was then the Joint Staff Common Room at lunch time (it is now the Haldane room, the common room having been confiscated by unenlightened management). Before leaving for the USA in 1970, I, in league with the then professor of French, Brian Woledge, eventually got through a motion that allowed women into the Housman room.
I’d also talk as much as I could to Bernard Katz, whom I asked to submit the first theoretical paper by Hawkes and me to the Royal Society. His comments on the first draft led to the published version making a prediction about single ion channel behaviour before channels could be observed.
The next step was sheer luck. As this was going on, two young Germans, Neher & Sakmann, succeeded in observing the tiny currents that flow through single ion channel molecules, so it became possible to test the theory. In series of visits to Göttingen, Sakmann and I did experiments late into the night. Neher & Sakmann got a well-deserved Nobel Prize in 1991, and I expect I benefitted from a bit of reflected glory
The work that I have done is nothing if not basic. It doesn’t fit in with the current vogue for translational research (most of which will fail), although I would regard it as laying the basis for rational drug design. My only regret is that rational drug design has proved to be so difficult that it won’t be achieved in my lifetime (please don’t believe the hype).
We’d also like you to take a slightly more personal view:
3. What have been the highs (and the lows?) of your career so far?
The highs have been the chance to work with brilliant people and write a handful of papers that have a chance of having a lasting influence. Because I have been able to take my time on those projects there haven’t been too many lows, apart from observing the continuous loss of academic integrity caused by the intense pressure to publish or perish, and the progressive decline in collegiality in universities caused by that pressure combined with the rise in power of managerialism. Luckily the advent of blogs has allowed me to do a little about that.
I’m saddened by the fact that the innumeracy of biologists that I noticed as an undergraduate has not really improved at all (though I don’t believe it is worse). Most biologists still have difficulty with even the simplest equations. Worse still, they don’t know enough maths to communicate their problem to a mathematician, so only too often one sees collaborations with mathematicians produce useless results.
The only real failure I’ve had was when, in a fit of vanity, I applied for the chair of Pharmacology in Oxford, in 1984, and failed to get it. But in retrospect that was really a success too. I would have hated the flummery of Oxford, and as head of department (an increasingly unattractive job) I would have spent my time on pushing paper, not ion channels. In retrospect, it was a lucky escape. UCL is my sort of place (most of the time).
We would like to hear what our role models have to say about the next generation:
4. What advice would you give to people finishing off their PhD?
My career course would be almost impossible now. In fact it is very likely that I would have been fired before I got going in the present climate. There were quite long periods when I didn’t publish much. I was learning the tools of my trade, both mathematical and experimental. Now there is no time to do that. You are under pressure to publish a paper a week (for the glory of your PI and your university) and probably rarely find time to leave the lab to talk to inspiring people. If you are given any courses they’ll probably be in some inane HR nonsense, not in algebra. That is one reason we started our summer workshop, though bizarrely that has now been dropped by the graduate school in favour of Advanced Powerpoint.
The plight of recent PhDs is dire. Too many are taken on (for the benefit of the university, not of the student) and there aren’t many academic jobs. If you want to stay in academia, all I can suggest is that you get good at doing something that other people can’t do, and to resist the pressure to publish dozens of trivial papers.
Try to maintain some academic integrity despite the many pressures to do the opposite that are imposed on you by your elders (but not always betters). That may or may not be enough to get you the job that you want, but at least you’ll be able to hold your head high.
Finally, we want to give a balanced impression of our role models because many were nominated for their ability to motivate others, and to balance life and work:
5. How do you keep motivated?
Work-life balance is much talked about by HR, though they are one of the reasons why it is now almost impossible, In the past it wasn’t a great problem. I’m fascinated by the problems that I’m trying to puzzle out. I’ve had periods of a year or two when things haven’t gone well and I’ve felt as though I was a failure, but luckily they haven’t lasted too long, and they occurred in a time before some idiotic performance manager would harass you for failing to publish for a year or two. The climate of “performance management” is doing a lot to kill innovation and creativity.
6. What do you do when are not working in SLMS?
I’ve had various phases. For a while I carried on boxing (which had been compulsory at school). When I was first at UCL in 1964 I bought a 21 foot sloop (and as a consequence could barely afford to eat), and in 1970 (at Yale) I learned to fly. I had a lot of fun sailing right up to the early 1980s, when I found I could not afford a son as well as a boat. That was when running came into fashion and that could be done for the price of a pair of shoes. I did marathons and half marathons for fun (the London in 1988 was great fun). And that was supplanted by walking country trails in the early 2000s.
There is never a clear division between work and play, especially with algebra. You can continue to struggle with a derivation on a boat, or even get a new angle on it while running. That, of course, is why the transparency review is such total nonsense.
The main cause of stress has never been work for me. Stress comes mainly from the imposition of dim-witted managerialism and incompetent HR policies. And that has become progressively worse. I doubt that if I were a young academic now I’d have the time to spend the weekend sailing.
I’m not sure whether the blogging that has taken up something like half my time since my nominal retirement in 2004 counts as work or not. It certainly depends on things that I have learned in my academic work. And it’s fun to have effects in the real world after a life spent on problems that many would regard as esoteric.
If you want a hobby that costs very little, and allows you to say what you want, start a blog.
Follow-up
The Scottish Universities Medical Journal asked me to write about the regulation of alternative medicine. It’s an interesting topic and not easy to follow because of the veritable maze of more than twenty overlapping regulators and quangos which fail utterly to protect the public against health fraud. In fact they mostly promote health fraud. The paper is now published, and here is a version with embedded links (and some small updates).
We are witnessing an increasing commercialisation of medicine. It’s really taken off since the passage of the Health and Social Security Bill into law. Not only does that mean having NHS hospitals run by private companies, but it means that “any qualified provider” can bid for just about any service. The problem lies, of course, in what you consider “qualified” to mean. Any qualified homeopath or herbalist will, no doubt, be eligible. University College London Hospital advertised for a spiritual healer. The "person specification" specified a "quallfication", but only HR people think that a paper qualification means that spiritual healing is anything but a delusion.
The vocabulary of bait and switch
First, a bit of vocabulary. Alternative medicine is a term that is used for medical treatments that don’t work (or at least haven’t been shown to work). If they worked, they’d be called “medicine”. The anti-malarial, artemesinin, came originally from a Chinese herb, but once it had been purified and properly tested, it was no longer alternative. But the word alternative is not favoured by quacks. They prefer their nostrums to be described as “complementary” –it sounds more respectable. So CAM (complementary and alternative medicine became the politically-correct euphemism. Now it has gone a stage further, and the euphemism in vogue with quacks at the moment is “integrated” or “integrative” medicine. That means, very often, integrating things that don’t work with things that do. But it sounds fashionable. In reality it is designed to confuse politicians who ask for, say, integrated services for old people.
Put another way, the salespeople of quackery have become rather good at bait and switch. The wikepedia definition is as good as any.
Bait-and-switch is a form of fraud, most commonly used in retail sales but also applicable to other contexts. First, customers are “baited” by advertising for a product or service at a low price; second, the customers discover that the advertised good is not available and are “switched” to a costlier product.
As applied to the alternative medicine industry, the bait is usually in the form of some nice touchy-feely stuff which barely mentions the mystical nonsense. But when you’ve bought into it you get the whole panoply of nonsense. Steven Novella has written eloquently about the use of bait and switch in the USA to sell chiropractic, acupuncture, homeopathy and herbal medicine: "The bait is that CAM offers legitimate alternatives, the switch is that it primarily promotes treatments that don’t work or are at best untested and highly implausible.".
The "College of Medicine" provides a near-perfect example of bait and switch. It is the direct successor of the Prince of Wales’ Foundation for Integrated Health. The Prince’s Foundation was a consistent purveyor of dangerous medical myths. When it collapsed in 2010 because of a financial scandal, a company was formed called "The College for Integrated Health". A slide show, not meant for public consumption, said "The College represents a new strategy to take forward the vision of HRH Prince Charles". But it seems that too many people have now tumbled to the idea that "integrated", in this context, means barmpottery. Within less than a month, the new institution was renamed "The College of Medicine". That might be a deceptive name, but it’s a much better bait. That’s why I described the College as a fraud and delusion.
Not only did the directors, all of them quacks, devise a respectable sounding name, but they also succeeded in recruiting some respectable-sounding people to act as figureheads for the new organisation. The president of the College is Professor Sir Graham Catto, emeritus professor of medicine at the University of Aberdeen. Names like his make the bait sound even more plausible. He claims not to believe that homeopathy works, but seems quite happy to have a homeopathic pharmacist, Christine Glover, on the governing council of his college. At least half of the governing Council can safely be classified as quacks.
So the bait is clear. What about the switch? The first thing to notice is that the whole outfit is skewed towards private medicine: see The College of Medicine is in the pocket of Crapita Capita. The founder, and presumably the main provider of funds (they won’t say how much) is the huge outsourcing company, Capita. This is company known in Private Eye as Crapita. Their inefficiency is legendary. They are the folks who messed up the NHS computer system and the courts computer system. After swallowing large amounts of taxpayers’ money, they failed to deliver anything that worked. Their latest failure is the court translation service.. The president (Catto), the vice president (Harry Brunjes) and the CEO (Mark Ratnarajah) are all employees of Capita.
The second thing to notice is that their conferences and courses are a bizarre mixture of real medicine and pure quackery. Their 2012 conference had some very good speakers, but then it had a "herbal workshop" with Simon Mills (see a video) and David Peters (the man who tolerates dowsing as a way to diagnose which herb to give you). The other speaker was Dick Middleton, who represents the huge herbal company, Schwabe (I debated with him on BBC Breakfast), In fact the College’s Faculty of Self-care appears to resemble a marketing device for Schwabe.
Why regulation isn’t working, and can’t work
There are various levels of regulation. The "highest" level is the statutory regulation of osteopathy and chiropractic. The General Chiropractic Council (GCC) has exactly the same legal status as the General Medical Council (GMC). This ludicrous state of affairs arose because nobody in John Major’s government had enough scientific knowledge to realise that chiropractic, and some parts of osteopathy, are pure quackery,
The problem is that organisations like the GCC function more to promote chiropractic than to regulate them. This became very obvious when the British Chiropractic Association (BCA) decided to sue Simon Singh for defamation, after he described some of their treatments as “bogus”, “without a jot of evidence”.
In order to support Singh, several bloggers assessed the "plethora of evidence" which the BCA said could be used to justify their claims. When, 15 months later, the BCA produced its "plethora" it was shown within 24 hours that the evidence was pathetic. The demolition was summarised by lawyer, David Allen Green, in The BCA’s Worst Day.
In the wake of this, over 600 complaints were made to the GCC about unjustified claims made by chiropractors, thanks in large part to heroic work by two people, Simon Perry and Allan Henness. Simon Perry’s Fishbarrel (browser plugin) allows complaints to be made quickly and easily -try it). The majority of these complaints were rejected by the GCC, apparently on the grounds that chiropractors could not be blamed because the false claims had been endorsed by the GCC itself.
My own complaint was based on phone calls to two chiropractors, I was told such nonsense as "colic is down to, er um, faulty movement patterns in the spine". But my complaint never reached the Conduct and Competence committee because it had been judged by a preliminary investigating committee that there was no case to answer. The impression one got from this (very costly) exercise was that the GCC was there to protect chiropractors, not to protect the public.
The outcome was a disaster for chiropractors, wno emerged totally discredited. It was also a disaster for the GCC which was forced to admit that it hadn’t properly advised chiropractors about what they could and couldn’t claim. The recantation culminated in the GCC declaring, in August 2010, that the mythical "subluxation" is a "historical concept " "It is not supported by any clinical research evidence that would allow claims to be made that it is the cause of disease.". Subluxation was a product of the fevered imagination of the founder of the chiropractic cult, D.D. Palmer. It referred to an imaginary spinal lesion that he claimed to be the cause of most diseases. .Since ‘subluxation’ is the only thing that’s distinguished chiropractic from any other sort of manipulation, the admission by the GCC that it does not exist, after a century of pretending that it does, is quite an admission.
The President of the BCA himself admitted in November 2011
“The BCA sued Simon Singh personally for libel. In doing so, the BCA began one of the darkest periods in its history; one that was ultimately to cost it financially,”
As a result of all this, the deficiencies of chiropractic, and the deficiencies of its regulator were revealed, and advertisements for chiropractic are somewhat less misleading. But this change for the better was brought about entirely by the unpaid efforts of bloggers and a few journalists, and not at all by the official regulator, the GCC. which was part of the problem. not the solution. And it was certainly not helped by the organisation that is meant to regulate the GCC, the Council for Health Regulatory Excellence (CHRE) which did nothing whatsoever to stop the farce.
At the other end of the regulatory spectrum, voluntary self-regulation, is an even worse farce than the GCC. They all have grand sounding "Codes of Practice" which, in practice, the ignore totally.
The Society of Homeopaths is just a joke. When homeopaths were caught out recommending sugar pills for prevention of malaria, they did nothing (arguably such homicidal advice deserves a jail sentence).
The Complementary and Natural Healthcare Council (CNHC) is widely know in the blogosphere as Ofquack. I know about them from the inside, having been a member of their Conduct and Competence Committee, It was set up with the help of a £900,000 grant from the Department of Health to the Prince of Wales, to oversee voluntary self-regulation. It fails utterly to do anything useful.. The CNHC code of practice, paragraph 15 , states
“Any advertising you undertake in relation to your professional activities must be accurate. Advertisements must not be misleading, false, unfair or exaggerated”.
When Simon Perry made a complaint to the CNHC about claims being made by a CNHC-registered reflexologist, the Investigating Committee upheld all 15 complaints. But it then went on to say that there was no case to answer because the unjustified claims were what the person had been taught, and were made in good faith.
This is precisely the ludicrous situation which will occur again and again if reflexologists (and many other alternative therapies) are “accredited”. The CNHC said, correctly, that the reflexologist had been taught things that were not true, but then did nothing whatsoever about it apart from toning down the advertisements a bit. They still register reflexologists who make outrageously false claims.
Once again we see that no sensible regulation is possible for subjects that are pure make-believe.
The first two examples deal (or rather, fail to deal) with regulation of outright quackery. But there are dozens of other quangos that sound a lot more respectable.
European Food Standards Agency (EFSA). One of the common scams is to have have your favourite quack treatment classified as a food not as a medicine. The laws about what you can claim have been a lot laxer for foods. But the EFSA has done a pretty good job in stopping unjustified claims for health benefits from foods. Dozens of claims made by makers of probiotics have been banned. The food industry, needless to say, objects very strongly to be being forced to tell the truth. In my view, the ESFA has not gone far enough. They recently issued a directive about claims that could legally be made. Some of these betray the previously high standards of the EFSA. For example you are allowed to say that "Vitamin C contributes to the reduction of tiredness and fatigue" (as long as the product contains above a specified amount of Vitamin C. I’m not aware of any trials that show vitamin C has the slightest effect on tiredness or fatigue, Although these laws do not come into effect until December 2012, they have already been invoked by the ASA has a reason not to uphold a complaint about a multivitamin pill which claimed that it “Includes 8 nutrients that can contribute to the reduction in tiredness and fatigue”
The Advertising Standards Authority (ASA). This is almost the only organisation that has done a good job on false health claims. Their Guidance on Health Therapies & Evidence says
"Whether you use the words ‘treatment’, ‘treat’ or ‘cure’, all are likely to be seen by members of the public as claims to alleviate effectively a condition or symptom. We would advise that they are not used"
"Before and after’ studies with little or no control, studies without human subjects, self-assessment studies and anecdotal evidence are unlikely to be considered acceptable"
"Before and after’ studies with little or no control, studies without human subjects, self-assessment studies and anecdotal evidence are unlikely to be considered acceptable"
They are spot on.
The ASA’s Guidance for Advertisers of Homeopathic Services is wonderful.
"In the simplest terms, you should avoid using efficacy claims, whether implied or direct,"
"To date, the ASA has have not seen persuasive evidence to support claims that homeopathy can treat, cure or relieve specific conditions or symptoms."
That seems to condemn the (mis)labelling allowed by the MHRA as breaking the rules.. Sadly, though, the ASA has no powers to enforce its decisions and only too often they are ignored. The Nightingale collaboration has produced an excellent letter that you can hand to any pharmacist who breaks the rules
The ASA has also judged against claims made by "Craniosacral therapists" (that’s the lunatic fringe of osteopathy). They will presumably uphold complaints about similar claims made (I’m ashamed to say) by UCLH Hospitals.
The private examination company Edexcel sets exams in antiscientific subjects, so miseducating children. The teaching of quackery to 16 year-olds has been approved by a maze of quangos, none of which will take responsibility, or justify their actions. So far I’ve located no fewer than eight of them. The Office of the Qualifications and Examinations Regulator (OfQual), Edexcel, the Qualifications and Curriculum Authority (QCA), Skills for Health, Skills for Care, National Occupational Standards (NOS), private exam company VTCT and the schools inspectorate, Ofsted.. Asking any of these people why they approve of examinations in imaginary subjects meets with blank incomprehension. They fail totally to protect tha public from utter nonsense.
The Department of Education has failed to do anything about the miseducation of children in quackery. In fact it has encouraged it by, for the first time, giving taxpayers’ money to a Steiner (Waldorf) school (at Frome, in Somerset). Steiner schools are run by a secretive and cult-like body of people (read about it). They teach about reincarnation, karma, gnomes, and all manner of nonsense, sometimes with unpleasant racial overtones. The teachers are trained in Steiner’s Anthroposophy, so if your child gets ill at school they’ll probably get homeopathic sugar pills. They might well get measles or mumps too, since Steiner people don’t believe in vaccination.
Incredibly, the University of Aberdeen came perilously close to appointing a chair in anthroposophical medicine. This disaster was aborted by bloggers, and a last minute intervention from journalists. Neither the university’s regulatory mechanisms. nor any others, seemed to realise that a chair in mystical barmpottery was a bad idea.
Trading Standards offices and the Office of Fair Trading.
It is the statutory duty of Trading Standards to enforce the Consumer Protection Regulations (2008) This European legislation is pretty good. it caused a lawyer to write " Has The UK Quietly Outlawed “Alternative” Medicine?". Unfortunately Trading Standards people have consistently refused to enforce these laws. The whole organisation is a mess. Its local office arrangement fails totally to deal with the age of the internet. The situation is so bad that a group of us decided to put them to the test. The results were published in the Medico-Legal Journal, Rose et al., 2012. "Spurious Claims for Health-care Products: An Experimental Approach to Evaluating Current UK Legislation and its Implementation". They concluded "EU directive 2005/29/EC is
largely ineffective in preventing misleading health claims for consumer products in
the UK"
Skills for Health is an enormous quango which produces HR style "competences" for everything under the son. They are mostly quite useless. But those concerned with alternative medicine are not just useless. They are positively harmful. Totally barmy. There are competences and National Occupational Standards for every lunatic made-up therapy under the sun. When I phoned them to discover who’d written them, I learned that the had been drafted by the Prince of Wales’ Foundation for Magic Medicine. And when I joked by asking if they had a competence for talking to trees, I was told, perfectly seriously, “You’d have to talk to LANTRA, the land-based organisation for that.”
That was in January 2008. A lot of correspondence with the head of Skills for Health got nowhere at all. She understood nothing and it hasn’t improved a jot.
This organisation costs a lot of taxpayers’ money and it should have been consigned to the "bonfire of the quangos" (but of course there was no such bonfire in reality). It is a disgrace.
The Quality Assurance Agency (QAA) is supposed to ensure the quality of university courses. In fact it endorses courses in nonsense alternative medicine and so does more harm than good. The worst recent failure of the QAA was in the case of the University of Wales: see Scandal of the University of Wales and the Quality Assurance Agency. The university was making money by validating thousands of external degrees in everything from fundamentalist theology to Chinese Medicine. These validations were revealed as utterly incompetent by bloggers, and later by BBC Wales journalist Ciaran Jenkins (now working for Channel 4).
The mainstream media eventually caught up with bloggers. In 2010, BBC1 TV (Wales) produced an excellent TV programme that exposed the enormous degree validation scam run by the University of Wales. The programme can be seen on YouTube (Part 1, and Part 2). The programme also exposed, incidentally, the uselessness of the Quality Assurance Agency (QAA) which did nothing until the scam was exposed by TV and blogs. Eventually the QAA sent nine people to Malaysia to investigate a dodgy college that had been revealed by the BBC. The trip cost £91,000. It could have been done for nothing if anyone at the QAA knew how to use Google.
The outcome was that the University of Wales stopped endorsing external courses, and it was soon shut down altogether (though bafflingly, its vice-chancellor, Marc Clement was promoted). The credit for this lies entirely with bloggers and the BBC. The QAA did nothing to help until the very last moment.
Throughout this saga Universities UK (UUK), has maintained its usual total passivity. They have done nothing whatsoever about their members who give BSc degrees in anti-scientific subjects. (UUK used to known as the Committee of Vice-Chancellors and Principals).
Council for Health Regulatory Excellence (CHRE), soon to become the PSAHSC,
Back now to the CHRE, the people who failed so signally to sort out the GCC. They are being reorganised. Their consultation document says
"The Health and Social Care Act 20122 confers a new function on the Professional Standards Authority for Health and Social Care (the renamed Council for Healthcare Regulatory Excellence). From November 2012 we will set standards for organisations that hold voluntary registers for people working in health and social care occupations and we will accredit the register if they meet those standards. It will then be known as an ‘Accredited Register’. "
They are trying to decide what the criteria should be for "accreditation" of a regulatory body. The list of those interested has some perfectly respectable organisations, like the British Psychological Society. It also contains a large number of crackpot organisations, like Crystal and Healing International, as well as joke regulators like the CNHC.
They already oversee the Health Professions Council (HPC) which is due to take over Herbal medicine and Traditional Chinese Medicine, with predictably disastrous consequences.
Two of the proposed criteria for "accreditation" appear to be directly contradictory.
Para 2.5 makes the whole accreditation pointless from the point of view of patients
2.5 It will not be an endorsement of the therapeutic validity or effectiveness of any particular discipline or treatment.
Since the only thing that matters to the patient is whether the therapy works (and is safe), accrediting of organisations that ignore this will merely give the appearance of official approval of crystal healing etc etc. This appears to contradict directly
A.7 The organisation can demonstrate that there either is a sound knowledge base underpinning the profession or it is developing one and makes that explicit to the public.
A "sound knowledge base", if it is to mean anything useful at all, means knowledge that the treatment is effective. If it doesn’t mean that, what does it mean?
It seems that the official mind has still not grasped the obvious fact that there can be no sensible regulation of subjects that are untrue nonsense. If it is nonsense, the only form of regulation that makes any sense is the law.
Please fill in the consultation. My completed return can be downloaded as an example, if you wish.
Medicines and Healthcare products Regulatory Agency (MHRA) should be a top level defender of truth. Its strapline is
"We enhance and safeguard the health of the public by ensuring that medicines and medical devices work and are acceptably safe."
The MHRA did something (they won’t tell me exactly what) about one of the most cruel scams that I’ve ever encountered, Esperanza Homeopathic Neuropeptide, peddled for multiple sclerosis, at an outrageous price ( £6,759 for 12 month’s supply). Needless to say there was not a jot of evidence that it worked (and it wasn’t actually homeopathic).
Astoundingly, Trading Standards officers refused to do anything about it.
The MHRA admit (when pushed really hard) that there is precious little evidence that any of the herbs work, and that homeopathy is nothing more than sugar pills. Their answer to that is to forget that bit about "ensuring that medicines … work"
Here’s the MHRA’s Traditional Herbal Registration Certificate for devils claw tablets.

The wording "based on traditional use only" has to be included because of European legislation. Shockingly, the MHRA have allowed them to relegate that to small print, with all the emphasis on the alleged indications. The pro-CAM agency NCCAM rates devil’s claw as "possibly effective" or "insufficient evidence" for all these indications, but that doesn’t matter because the MHRA requires no evidence whatsoever that the tablets do anything. They should, of course, added a statement to this effect to the label. They have failed in their duty to protect and inform the public by allowing this labelling.
But it gets worse. Here is the MHRA’s homeopathic marketing authorisation for the homeopathic medicinal product Arnicare Arnica 30c pillules
It is nothing short of surreal.
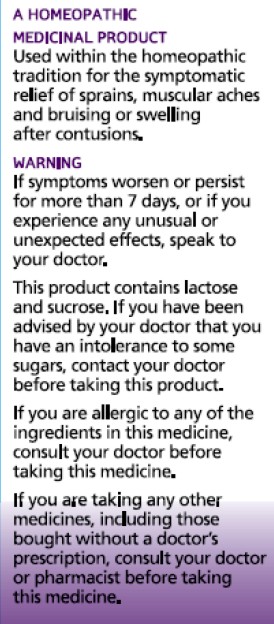
|
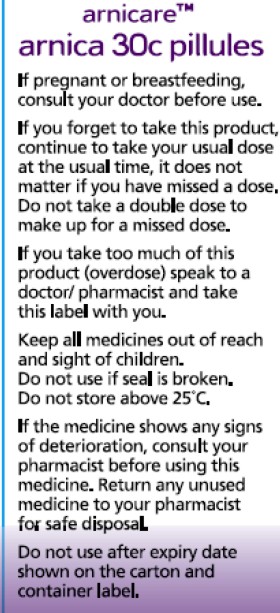
|
Since the pills contain nothing at all, they don’t have the slightest effect on sprains, muscular aches or bruising. The wording on the label is exceedingly misleading.
If you "pregnant or breastfeeding" there is no need to waste you doctor’s time before swallowing a few sugar pills.
"Do not take a double dose to make up for a missed one". Since the pills contain nothing, it doesn’t matter a damn.
"If you overdose . . " it won’t have the slightest effect because there is nothing in them
And it gets worse. The MHRA-approved label specifies ACTIVE INGREDIENT. Each pillule contains 30c Arnica Montana
No, they contain no arnica whatsoever.
|
|
It truly boggles the mind that men with dark suits and lots of letters after their names have sat for hours only to produce dishonest and misleading labels like these.
When this mislabeling was first allowed, it was condemned by just about every scientific society, but the MHRA did nothing.
The Nightingale Collaboration.
This is an excellent organisation, set up by two very smart skeptics, Alan Henness and Maria MacLachlan. Visit their site regularly, sign up for their newsletter Help with their campaigns. Make a difference.
Conclusions
The regulation of alternative medicine in the UK is a farce. It is utterly ineffective in preventing deception of patients.
Such improvements as have occurred have resulted from the activity of bloggers, and sometime the mainstream media. All the official regulators have, to varying extents, made things worse.
The CHRE proposals promise to make matters still worse by offering "accreditation" to organisations that promote nonsensical quackery. None of the official regulators seem to be able to grasp the obvious fact that is impossible to have any sensible regulation of people who promote nonsensical untruths. One gets the impression that politicians are more concerned to protect the homeopathic (etc, etc) industry than they are to protect patients.
Deception by advocates of alternative medicine harms patients. There are adequate laws that make such deception illegal, but they are not being enforced. The CHRE and its successor should restrict themselves to real medicine. The money that they spend on pseudo-regulation of quacks should be transferred to the MHRA or a reformed Trading Standards organisation so they can afford to investigate and prosecute breaches of the law. That is the only form of regulation that makes sense.
Follow-up
The shocking case of the continuing sale of “homeopathic vaccines” for meningitis, rubella, pertussis etc was highlighted in an excellent TV programme by BBC South West. The failure of the MHRA and the GPC do take any effective action is a yet another illustration of the failure of regulators to do their job. I have to agree with Andy Lewis when he concludes
“Children will die. And the fault must lie with Professor Sir Kent Woods, chairman of the regulator.”
|
This is a very important book. Buy it now (that link is to Waterstone’s Amazon don’t pay tax in the UK, so don’t use them). When you’ve read it, do something about it. The book has lots of suggestions about what to do. |

Stolen from badscience.net |
Peter Medawar, the eminent biologist, in his classic book Advice to a Young Scientist, said this.
“Exaggerated claims for the efficacy of a medicament are very seldom the consequence of any intention to deceive; they are usually the outcome of a kindly conspiracy in which everybody has the very best intentions. The patient wants to get well, his physician wants to have made him better, and the pharmaceutical company would have liked to have put it into the physician’s power to have made him so. The controlled clinical trial is an attempt to avoid being taken in by this conspiracy of good will.”
There was a lot of truth in that 1979, towards the end of the heyday of small molecule pharmacology. Since then, one can argue, things have gone downhill.
First, though, think of life without general anaesthetics, local anaesthetics, antibiotics, anticoagulants and many others. They work well and have done incalculable good. And they were developed by the drug industry.
But remember also that remarkably little is known about medicine. There are huge areas in which neither causes nor cures are known. Treatments for chronic pain, back problems, many sorts of cancer and almost all mental problems are a mess. It just isn’t known what to do. Nobody is to blame for this. Serious medical research has been going on for little more than 60 years, and it turns out to be very complicated. We are doing our best, but are still ignorant about whole huge areas. That leads to a temptation to make things up. Clutching at straws is very evident when it comes to depression, pain and Alzheimer’s disease, among others.
In order to improve matters, one essential is to do fair tests on treatments that we have. Ben Goldacre’s book is a superb account of how this could be done, and how the process of testing has been subverted for commercial gain and to satisfy the vanities of academics.
Of course there is nothing new in criticisms of Big Pharma. The huge fines levied on them for false advertising are well known. The difference is that Goldacre’s book explains clearly what’s gone wrong in great detail, documents it thoroughly, and makes concrete suggestions for improving matters.
Big Pharma has undoubtedly sometimes behaved appallingly in recent years. Someone should be in jail for crimes against patients. They have behaved in much the same way that bankers have. In any huge globalised industry it is always possible to blame someone in another department for the dishonesty. But they aren’t the only people to blame. None of the problems could have arisen with the complicity of academics, universities, and a plethora of regulatory agencies and professional bodies.
The biggest scandal of all is missing data (chapter 1). Companies, and sometmes academics, have suppressed of trials that don’t favour the drugs that they are trying to sell. The antidepressant drug, reboxetine, appeared at first to be good. It had been approved by the Medicines and Healthcare products Regulatory Agency (MHRA) and there was at least one good randomized placebo-controlled trial (RCT) showing it worked. But it didn’t. The manufacturer didn’t provide a complete list of unpublished trials when asked for them. After much work it was found in 2010 that, as well as the published, favourable trial, there were six more trials which had not been published and all six showed reboxetine to be no better than placebo . In comparisons with other antidepressant drugs three small studies (507 patients) showed reboxetine to be as good as its competitors. These were published. But it came to light that data on 1657 patients had never been published and these showed reboxetine to be worse than its rivals.
When all the data for the SSRI antidepressants were unearthed (Kirsch et al., 2008) it turned out that they were no better than placebo for mild or moderate depression. This selective suppression of negative data has happened time and time again. It harms patients and deceives doctors, but, incredibly, it’s not illegal.
Disgracefully, Kirsch et al. had to use a Freedom of Information Act request to get the data from the FDA.
“The output of a regulator is often simply a crude, brief summary: almost a ‘yes’ or ‘no’ about side effects. This is the opposite of science, which is only reliable because everyone shows their working, explains how they know that something is effective or safe, shares their methods and their results, and allows others to decide if they agree with the way they processed and analysed the data.”
|
“the NICE document discussing whether it’s a good idea to have Lucentis, an extremely expensive drug, costing well over £ 1,000 per treatment, that is injected into the eye for a condition called acute macular degeneration. As you can see, the NICE document on whether this treatment is a good idea is censored. Not only is the data on the effectiveness of the treatment blanked out by thick black rectangles, in case any doctor or patient should see it, but absurdly, even the names of some trials are missing, preventing the reader from even knowing of their existence, or cross referencing information about them.Most disturbing of all, as you can see in the last bullet point, the data on adverse events is also censored.”
|
 |
The book lists all the tricks that are used by both industry and academics. Here are some of them.
- Regulatory agencies like the MHRA, the European Medicines Agency (EMA) and the US Food and Drugs Administration (FDA) set a low bar for approval of drugs.
- Companies make universities sign gagging agreements which allow unfavourable results to be suppressed, and their existence hidden.
- Accelerated approval schemes are abused to get quick approval of ineffective drugs and the promised proper tests often don’t materialise
- Disgracefully, even when all the results have been given to the regulatory agencies (which isn’t always). The MHRA, EMA and FDA don’t make them public. We are expected to take their word.
- Although all clinical trials are meant to be registered before they start, the EMA register, unbelievably, is not public. Furthermore there is no check that the results if trials ever get published. Despite mandates that results must be published within a year of finishing the trial, many aren’t. Journals promise to check this sort of thing, but they don’t.
- When the results are published, it is not uncommon for the primary outcome, specified before it started, to have been changed to one that looks like a more favourable result. Journals are meant to check, but mostly don’t.
- Companies use scientific conferences, phony journals, make-believe “seed trials” and “continuing medical education” for surreptitious advertising.
- Companies invent new diseases, plant papers to make you think you’re abnormal, and try to sell you a “cure”. For example, female sexual dysfunction , restless legs syndrome and social anxiety disorder (i.e. shyness). This is called disease-mongering, medicalisation or over-diagnosis. It’s bad.
- Spin is rife. Companies, and authors, want to talk up their results. University PR departments want to exaggerate benefits. Journal editors want sensational papers. Read the results, not the summary. This is universal (but particularly bad in alternative medicine).
- Companies fund patient groups to lobby for pills even when the pills are known to be ineffective. The lobby that demanded that Herceptin should be available to all on the breast cancer patients on the NHS was organised by a PR company working for the manufacturer, Roche. But Herceptin doesn’t work at all in 80% of patients and gives you at best a few extra months of life in advanced cases.
- Ghostwriting of papers is serious corruption. A company writes the paper and senior academics appear as the authors, though they may never have seen the original data. Even in cases where academics have admitted to lying about whether they have seen the data, they go unpunished by their universities. See for example, the case of Professor Eastell.
- By encouraging the funding of “continuing medical education” by companies, the great and the good of academic medicine have let us down badly.
This last point is where the book ends, and it’s worth amplification.
“So what have the great and good of British medicine done to help patients, in the face of this endemic corruption, and these systematic flaws? In 2012, a collaborative document was produced by senior figures in medicine from across the board, called ‘Guidance on Collaboration Between Healthcare Professionals and the Pharmaceutical Industry’. This document was jointly approved by the ABPI, the Department of Health, the Royal Colleges of Physicians, Nursing, Psychiatrists, GPs, the Lancet, the British Medical Association, the NHS Confederation, and so on. ”
“It contains no recognition of the serious problems we have seen in this book. In fact, quite the opposite: it makes a series of assertions about them that are factually incorrect.”
“It states that drug reps ‘can be a useful resource for healthcare professionals’. Again, I’m not sure why the Royal Colleges, the BMA, the Department of Health and the NHS Confederation felt the need to reassert this to the doctors of the UK, on behalf of industry, when the evidence shows that drug reps actively distort prescribing practices. But that is the battle you face, trying to get these issues taken seriously by the pinnacle of the medical establishment.”
This is perhaps the most shameful betrayal of all. The organisations that should protect patients have sold them out.
You may have been sold out by your “elders and betters”, but you can do something. The “What to do” sections of the book should be produced as a set of flash cards, as a reminder that matters can be improved.
It is shameful that this book was not written by a clinical pharmacologist, or a senior doctor, or a Royal College, or a senior academic. Why has the British Pharmacological Society said nothing?
It is shameful too that this book was not written by one of the quacks who are keen to defend the $60 billion alternative medicine industry (which has cured virtually nothing) and who are strident in their criticism of the 600 billion dollar Pharma industry. They haven’t done the work that Goldacre has to analyse the real problems. All they have done is to advocate unfair tests, because that is the only sort their treatments can pass.
It’s weird that medicine, the most caring profession, is more corrupt than any other branch of science. The reason, needless to say, is money. Well, money and vanity. The publish or perish mentality of senior academics encourages dishonesty. It is a threat to honest science.
Goldacre’s book shows the consequences: harm to patients and huge wastage of public money.
Read it.
Do something.
Follow-up
7 October, 2012, The Observer
Goldacre wrote
"I think it’s really disappointing that nobody, not the Royal Colleges, the Academy of Medical Sciences, the British Pharmacological Society, the British Medical Association, none of these organisations have stood up and said: selective non-publication of unflattering trial data is research misconduct, and if you do it you will be booted out. And I think they really urgently should."
Exactly.
The row about redundancies firings at Queen Mary rumbles on.
|
I’ve already written about it twice in Is Queen Mary University of London trying to commit scientific suicide?, and in Queen Mary, University of London in The Times. Does Simon Gaskell care?. But wait, there is more to come. The harm done to teaching at Queen Mary was outlined in a report written at the request of Simon Gaskell. He appears to have ignored it entirely. So let’s concentrate on research. |

Some explanation of the bizarre behaviour of the Queen Mary management can be gleaned from Queen Mary’s Frequently Asked Questions:
Restructures and Reviews in Academic Departments 2011-12. This says
“research-related metrics” used in the School of Biological and Chemical Sciences are the result of “extensive consultation with staff and include both the Australian [Research Council] journal classification system as well as impact factor”.
Let’s skip over the fact that the "extensive consultation" was largely sham. That’s standard procedure (and not only in universities).
Australian journal classification
The reference to the Australian journal classification is revealing. Australia has been noted in the past for being one of the worst places for abuse of publication metrics. Its 2010 Journal classification was utterly bizarre [download Excel]. It ranks 20,712 journals as being A*, A, B, or C (did the rankers really look at all of them?).
I’ll take one example from my own area: the Journal of General Physiology is probably one of the most-respected journals for electrophysiology with emphasis on mechanisms. Many of its papers are quite mathematical. In its niche, it is hugely respected for the quality of papers and for its high integrity [declaration of interest, I’m an editor, and was hugely flattered by that honour]. But the Australian 2010 list ranks the Journal of General Physiology as B, the same as Brain Research, British Journal of Religious Education and Chinese Medicine (a journal of quack medicine).
In contrast, the Nature journals all get A*, as do many review journals which don’t publish original research at all. But if you can’t get a paper into Nature, there are other A* journals that might help you keep your job, for example Television and New Media, or Tourism Management as well as some joke journals like the Journal of Alternative and Complementary Medicine and Complementary Therapies in Medicine.
No doubt you’ll find similar ludicrous anomalies in your own field.
Simon Gaskell has not answered emails from me, and he hasn’t answered those from his own staff either, but he did emerge briefly from his shell last week, in The Times and at greater length in today’s Times Higher Education. The latter, though longer, consists almost entirely of the vapid self-congratulation which all vice-chancellors feel compelled to spout. Only one short paragraph is devoted to answering his critics.
“Where academic performance has been assessed, it has been important to do so on the basis of objective criteria including metrics – any subjective assessment would be quite unacceptable. These objective criteria were based on generally recognised academic expectations . . . “
I find it almost impossible to believe that a vice-chancellor should be so out of touch as to believe that counting papers, and using impact factors to judge people are “generally recognised”. The extent of the misunderstanding of metrics is illustrated by two statements for Matthew Evans, head of the School of Biological and Chemical Sciences. is quoted as saying:
“Impact factor reflects the number of times an average paper is cited, [so] is a good indication of how many citations a particular paper is likely to achieve,”
Anyone who understands the difference between mode, median and mean of the highly skewed distribution of citations would not make an elementary mistake like that. It is simply statistical illiteracy.
Evans also
"…described metrics as a “vital tool” in assessing academics’ contributions to research and “the only empirical way of measuring success in science”."
Is Matthew Evans not aware that there isn’t the slightest evidence that any metric predicts the future success of a scientist? It’s an evidence-free zone Perhaps he should read about how to test social interventions.
It’s certainly evident that Gaskell’s management team can’t use Google. After getting the hint about the use of Australian rankings, it took five minutes to discover this statement.
"On 30 May 2011, the decision not to use ranked outlets for ERA 2012 was announced".
It’s more than a year since Kim Carr, at that time the Australian minister for innovation, industry, science and research, announced the result of a review of the way the next ce of Research in Australia (ERA) exercise would be conducted by the Australian Research Council (ARC).
“There is clear and consistent evidence that the rankings were being deployed inappropriately within some quarters of the sector, in ways that could produce harmful outcomes, and based on a poor understanding of the actual role of the rankings. One common example was the setting of targets for publication in A and A* journals by institutional research managers.
“their existence was focussing ill-informed, undesirable behaviour in the management of research – I have made the decision to remove the rankings, based on the ARC’s expert advice”.
It seems that Professor Gaskell is unaware of this, since he is enforcing the very “ill-informed, undesirable behaviour in the management of research” that Australia has dropped.
That is what I’d call a major cock-up.
HEFCE also reviewed the role of metrics. Their pilot tests were, almost needless to say, not properly randomised, but the conclusion was much the same as in Australia. Is Gaskell not aware that REF instructions say
“No sub-panel will make any use of journal impact factors, rankings, lists or the perceived standing of publishers in assessing the quality of research outputs”
The very people Gaskell seeks to please have condemned strongly his methods.
If that is not “bringing your university into disrepute”, I don’t know what is.
The responses to Simon Gaskell
This week’s Times Higher Education published three letters in response to Gaskell’s article.
The lead letter was signed by thirteen Queen Mary academics. This gives the flavour.
“Here we point to the unintended consequences of restructuring already in evidence. These include undermining morale in the schools and departments concerned; the flight of talented colleagues to other institutions; the consignment of teaching to lecturers in casual employment or those deemed unfit for research; scandalous gender disparity; and the lopsided, counterproductive allocation of resources. When staff are dismissed, replacements can come only from other institutions that have been willing to invest in people, research and scholarship. As a part of normal academic life, mobility is acceptable, even desirable, but when enforced on the scale envisaged at Queen Mary, it is random slaughter offset by poaching.”
My letter described the cock-up over the ARC Journal classification.
The third letter was from Fanis Missirlis, who was co-authot of the Lancet letter, Queen Mary: nobody expects the Spanish Inquisition. As a result he was fired at one day’s notice. He is one of the academics whose “careers are destroyed by decimal points in spurious calculations”
The Queen Mary process was summed up rather well when the University of Sydney went through a similar convulsion. An Australian academic referred to
"retrenchment exercises driven by “crass, bureaucratic, quantifiable simulacra of genuine research”.
Follow-up
August 23 2012.
|
I see it is now official. One of the great stars of Queen Mary, Lisa Jardine, is leaving Queen Mary (and, as it happens, coming to UCL). Learn more about her in an interview with Laurie Taylor. She discovered lost papers by the great renaissance scientist, Robert Hooke –watch the video. |

20 December 2012
It seems that the predicted bad effects are coming true. Times Higher Education carries a letter from a biology undergraduate, Matthew James Erickson, which is highly critical of the effect of Gaskell’s policies on teaching at Queen Mary.
“From my perspective as a first-year undergraduate, the aggressive restructuring has had a profoundly negative effect on my opinion of my university.”
It is rather wonderful when a first year undergraduate dares to speak truth to power. Well done Matthew James Erickson.
A lot of people from around the world ready my last post, Is Queen Mary University of London trying to commit scientific suicide?. Nonetheless, the mainstream media reach a different audience. They are still needed. Oddly enough, the Guardian Higher Education section didn’t seem very interested. For a paper that publishes Polly Toynbee and George Monbiot, the education section is surprisingly establishment-orientated. So is Times Higher Education, especially now the excellent Zoe Corbyn has left.
The Times, however, welcomed it. On Monday 30 July, the following much shortened version of the blog appeared. And in the Thunderer column, no less (again). Two of the most irritating things about writing for papers are the lack of links, and the often silly titles chosen by sub-editors not the author. [download pdf].
|
There are moments when the way a university runs its affairs is so boneheaded that it deserves scorn far beyond the world of academia. Queen Mary University of London is selecting which staff to sack from its science departments in a way that I can describe only as insane. The firings, it seems, are nothing to do with hard financial times, but are a ham-fisted attempt to raise Queen Mary’s ranking in the league tables. A university’s position is directly related to its government research funding. So Queen Mary’s managers hope to do well in the 2014 “Research Excellence Framework” by firing staff who don’t publish a paper every ten minutes. To survive as a professor there you need to have published 11 papers during 2008 to 2011, of which at least two are “high quality”. For lecturers, the target for keeping your job is five papers, of which one is “high quality”. You must also have had at least one PhD student complete their thesis. What Queen Mary defines as “high quality” is publication in “high-impact journals” (periodicals that get lots of citations). Journals such as Nature and Science get most of their citations from very few articles, so it is utterly brainless to base decisions about the quality of research from such a skewed distribution of citations. But talk of skewed distribution is, no doubt, a bit too technical for innumerate HR people to understand. Which is precisely why they should have nothing to do with assessing scientists. I have been lucky to know well three Nobel prizewinners. None would have passed the criteria laid down for a professor by QMUL. They would have been fired and so would Peter Higgs. More offensive still is that you can buy immunity if you have had 26 papers published in 2008-11, with six being “high quality”. The encouragement to publish reams is daft. If you are publishing a paper every few weeks, you certainly are not writing them, and possibly not even reading them. Most likely you are appending your name to somebody else’s work with little or no checking of the data, let alone contributing real research. It is also deeply unethical for Queen Mary to require all staff to have a PhD student with the aim of raising the university’s ranking rather than of benefitting the student. Like so much managerialism, the rules are an active encouragement to dishonesty. The dimwitted assessment methods of Queen Mary will guarantee the creation of a generation of second-rate spiv scientists. Who in their right mind would want to work there, now that the way it treats its scientists is public knowledge? David Colquhoun is Professor of Pharmacology at University College London
|
Follow-up
August 3 2012 A response from Simon Gaskell appeared in the letter column of The Times.
|
Publication of research findings is only one criterion in a range of expectations within the realm of academia Sir, Professor Colquhoun is entitled to question the value of publishing in academic journals and the role this plays in academia (Thunderer, July 30). However, some will wish to understand more of the background of the criticism he levelled at Queen Mary, University of London. QM is ranked in the top dozen or so research universities in the UK, as judged by the last Research Assessment Exercise. To continue making this contribution and to ensure that our students receive the finest research-led education, we’ve had to address a small number of academic areas where performance doesn’t match expectations. And in a challenging environment for higher education, we need to safeguard QM’s financial stability. We have applied objective criteria to the assessment of individual academic performance. These criteria are based on generally recognised academic expectations that take account of differences between disciplines and have been applied in a manner that acknowledges the imprecision of any such measures. Publication of research findings was only one criterion. We are now investing in those areas that have been restructured with a focus on establishing strengths in the medium to long term that will continue to benefit not only our students but broader society and will make best use of our resources, both public and private. Professor Simon J. Gaskell |
I fear that Gaskell has just dug himself deeper in the pit of his own making. Here is the letter I have submitted for publication. I left a similar online comment, which has already appeared.
|
Sir. Professor Gaskell (Letters, August 3) tries to defend his actions at Queen Mary, University of London by saying "We have applied objective criteria to the assessment of individual academic performance. These criteria are based on generally recognised academic expectations". Nothing could be further from the truth. It is most certainly not "generally recognised" that you can measure the worth of a scientist by simply counting the number of papers they produce, or by looking at the impact factor of the journal in which they appear. I’m afraid Professor Gaskell appears to be totally out of touch with the literature about such matters. The Research Excellence Framework says explicitly "No sub-panel will make any use of journal impact factors, rankings, lists or the perceived standing of publishers in assessing the quality of research outputs". Furthermore the REF allows submission of only four papers, and tries to assess their quality. Production of a large number of salami-sliced papers would hinder, not help. His actions appear to harm rather than help his university’s chances in the REF. Gaskell’s says also that he wants to "ensure that our students receive the finest research-led education". But we all know that someone who produces the large number of publications that he demands is unlikely to have either the time or the inclination to teach students too. Then, of course, there is the dubious legality of declaring a person "redundant" while advertising an essentially identical job. The word for his process is firing, not redundancy. I see no reason to change my view (Thunderer July 30) that Professor Gaskell is bringing his university into disrepute. David Colquhoun |
August 3 2012 A correspondent write to me to point out an article that described the management methods that led to a lost decade by Microsoft. They are remarkably similar to those being imposed at Queen Mary.
"It leads to employees focusing on competing with each other rather than competing with other companies.”
It’s unfortunate that university managers so often seem to latch on to ideas that have already been discredited in industry.
August 6 2012. The Times hasn’t published my response, but they did publish today a letter from Professor Gavin Vinson, of Queen Mary. I was too kind to mention the obvious absurdity of Gaskell’s first sentence. Now it has been done..
|
Published at 12:01AM, August 6 2012
Judging scientists No one disputes the value of publishing in science and academia. However, all opinions need to havea basis in fact to support them Sir, Professor Simon Gaskell (letter, Aug 3) says, “Professor Colquhoun is entitled to question the value of publishing in academic journals and the role this plays in academia” (Thunderer, July 30). Try as I might, I have failed to find the basis for this statement in Professor Colquhoun’s article, or indeed anywhere else come to that. No one disputes the value of publishing in science and academia. What is in dispute is the use of spurious metrics in evaluating scientists. Professor Gavin P. Vinson |
Academic staff are going to be fired at Queen Mary University of London (QMUL). It’s possible that universities may have to contract a bit in hard times, so what’s wrong?
What’s wrong is that the victims are being selected in a way that I can describe only as insane. The criteria they use are guaranteed to produce a generation of second-rate spiv scientists, with a consequent progressive decline in QMUL’s reputation.
The firings, it seems, are nothing to do with hard financial times, but are a result of QMUL’s aim to raise its ranking in university league tables.
In the UK university league table, a university’s position is directly related to its government research funding. So they need to do well in the 2014 ‘Research Excellence Framework’ (REF). To achieve that they plan to recruit new staff with high research profiles, take on more PhD students and post-docs, obtain more research funding from grants, and get rid of staff who are not doing ‘good’ enough research.
So far, that’s exactly what every other university is trying to do. This sort of distortion is one of the harmful side-effects of the REF. But what’s particularly stupid about QMUL’s behaviour is the way they are going about it. You can assess your own chances of survival at QMUL’s School of Biological and Chemical Sciences from the following table, which is taken from an article by Jeremy Garwood (Lab Times Online. July 4, 2012). The numbers refer to the four year period from 2008 to 2011.
|
Category of staff |
Research Output Quantity |
Research Output |
Research Income (£) |
Research Income (£) |
|
Professor |
11 |
2 |
400,000 |
at least 200,000 |
|
Reader |
9 |
2 |
320,000 |
at least 150,000 |
|
Senior Lecturer |
7 |
1 |
260,000 |
at least 120,000 |
|
Lecturer |
5 |
1 |
200,000 |
at least 100,000 |
|
In addition to the three criteria, ‘Research Output ‐ quality’, ‘Research Output – quantity’, and ‘Research Income’, there is a minimum threshold of 1 PhD completion for staff at each academic level. All this data is “evidenced by objective metrics; publications cited in Web of Science, plus official QMUL metrics on grant income and PhD completion.” To survive, staff must meet the minimum threshold in three out of the four categories, except as follows: Demonstration of activity at an exceptional level in either ‘research outputs’ or ‘research income’, termed an ‘enhanced threshold’, is “sufficient” to justify selection regardless of levels of activity in the other two categories. And what are these enhanced thresholds? |
|
The university notes that the above criteria “are useful as entry standards into the new school, but they fall short of the levels of activity that will be expected from staff in the future. These metrics should not, therefore, be regarded as targets for future performance.” This means that those who survived the redundancy criteria will simply have to do better. But what is to reassure them that it won’t be their turn next time should they fail to match the numbers? To help them, Queen Mary is proposing to introduce ‘D3’ performance management (www.unions.qmul.ac.uk/ucu/docs/d3-part-one.doc). Based on more ‘administrative physics’, D3 is shorthand for ‘Direction × Delivery × Development.’ Apparently “all three are essential to a successful team or organisation. The multiplication indicates that where one is absent/zero, then the sum is zero!” D3 is based on principles of accountability: “A sign of a mature organisation is where its members acknowledge that they face choices, they make commitments and are ready to be held to account for discharging these commitments, accepting the consequences rather than seeking to pass responsibility.” Inspired? |
I presume the D3 document must have been written by an HR person. It has all the incoherent use of buzzwords so typical of HR. And it says "sum" when it means "product" (oh dear, innumeracy is rife).
The criteria are utterly brainless. The use of impact factors for assessing people has been discredited at least since Seglen (1997) showed that the number of citations that a paper gets is not perceptibly correlated with the impact factor of the journal in which it’s published. The reason for this is the distribution of the number of citations for papers in a particular journal is enormously skewed. This means that high-impact journals get most of their citations from a few articles.
|
The distribution for Nature is shown in Fig. 1. Far from being gaussian, it is even more skewed than a geometric distribution; the mean number of citations is 114, but 69% of papers have fewer than the mean, and 24% have fewer than 30 citations. One paper has 2,364 citations but 35 have 10 or fewer. ISI data for citations in 2001 of the 858 papers published in Nature in 1999 show that the 80 most-cited papers (16% of all papers) account for half of all the citations (from Colquhoun, 2003)
|
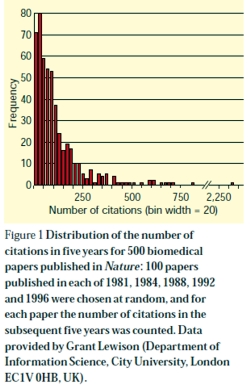
|
The Institute of Scientific Information, ISI, is guilty of the unsound statistical practice of characterizing a distribution by its mean only, with no indication of its shape or even its spread. School of Biological and Chemical Sciences-QMUL is expecting everyone has to be above average in the new regime. Anomalously, the thresholds for psychologists are lower because it is said that it’s more difficult for them to get grants. This undermines even the twisted logic applied at the outset.
All this stuff about skewed distributions is, no doubt, a bit too technical for HR people to understand. Which, of course, is precisely why they should have nothing to do with assessing people.
At a time when so may PhDs fail to get academic jobs we should be limiting the numbers. But QMUL requires everyone to have a PhD student, not for the benefit of the student, but to increase its standing in league tables. That is deeply unethical.
The demand to have two papers in journals with impact factor greater than seven is nonsense. In physiology, for example, there are only four journals with an impact factor greater that seven and three of them are review journals that don’t publish original research. The two best journals for electrophysiology are Journal of Physiology (impact factor 4.98, in 2010) and Journal of General Physiology (IF 4.71). These are the journals that publish papers that get you into the Royal Society or even Nobel prizes. But for QMUL, they don’t count.
I have been lucky to know well three Nobel prize winners. Andrew Huxley. Bernard Katz, and Bert Sakmann. I doubt that any of them would pass the criteria laid down for a professor by QMUL. They would have been fired.
The case of Sakmann is analysed in How to Get Good Science, [pdf version]. In the 10 years from 1976 to 1985, when Sakmann rose to fame, he published an average of 2.6 papers per year (range 0 to 6). In two of these 10 years he had no publications at all. In the 4 year period (1976 – 1979 ) that started with the paper that brought him to fame (Neher & Sakmann, 1976) he published 9 papers, just enough for the Reader grade, but in the four years from 1979 – 1982 he had 6 papers, in 2 of which he was neither first nor last author. His job would have been in danger if he’d worked at QMUL. In 1991 Sakmann, with Erwin Neher, got the Nobel Prize for Physiology or Medicine.
The most offensive thing of the lot is the way you can buy yourself out if you publish 26 papers in the 4 year period. Sakmann came nowhere near this. And my own total, for the entire time from my first paper (1963) until I was elected to the Royal Society (May 1985) was 27 papers (and 7 book chapters). I would have been fired.
Peter Higgs had no papers at all from the time he moved to Edinburgh in 1960, until 1964 when his two paper’s on what’s now called the Higgs’ Boson were published in Physics Letters. That journal now has an impact factor less than 7 so Queen Mary would not have counted them as “high quality” papers, and he would not have been returnable for the REF. He too would have been fired.
The encouragement to publish large numbers of papers is daft. I have seen people rejected from the Royal Society for publishing too much. If you are publishing a paper every six weeks, you certainly aren’t writing them, and possibly not even reading them. Most likely you are appending your name to somebody else’s work with little or no checking of the data. Such numbers can be reached only by unethical behaviour, as described by Peter Lawrence in The Mismeasurement of Science. Like so much managerialism, the rules provide an active encouragement to dishonesty.
In the face of such a boneheaded approach to assessment of your worth, it’s the duty of any responsible academic to point out the harm that’s being done to the College. Richard Horton, in the Lancet, did so in Bullying at Barts. There followed quickly letters from Stuart McDonald and Nick Wright, who used the Nuremburg defence, pointing out that the Dean (Tom Macdonald) was just obeying orders from above. That has never been as acceptable defence. If Macdonald agreed with the procedure, he should be fired for incompetence. If he did not agree with it he should have resigned.
It’s a pity, because Tom Macdonald was one of the people with whom I corresponded in support of Barts’ students who, very reasonably, objected to having course work marked by homeopaths (see St Bartholomew’s teaches antiscience, but students revolt, and, later, Bad medicine. Barts sinks further into the endarkenment). In that case he was not unreasonable, and, a mere two years later I heard that he’d taken action.
To cap it all, two academics did their job by applying a critical eye to what’s going on at Queen Mary. They wrote to the Lancet under the title Queen Mary: nobody expects the Spanish Inquisition
"For example, one of the “metrics” for research output at professorial level is to have published at least two papers in journals with impact factors of 7 or more. This is ludicrous, of course—a triumph of vanity as sensible as selecting athletes on the basis of their brand of track suit. But let us follow this “metric” for a moment. How does the Head of School fair? Zero, actually. He fails. Just consult Web of Science. Take care though, the result is classified information. HR’s “data” are marked Private and Confidential. Some things must be believed. To question them is heresy."
Astoundingly, the people who wrote this piece are now under investigation for “gross misconduct”. This is behaviour worthy of the University of Poppleton, as pointed out by the inimitable Laurie Taylor, in Times Higher Education (June 7)
|
The rustle of censorship It appears that last week’s edition of our sister paper, The Poppleton Evening News, carried a letter from Dr Gene Ohm of our Biology Department criticising this university’s metrics-based redundancy programme. We now learn that, following the precedent set by Queen Mary, University of London, Dr Ohm could be found guilty of “gross misconduct” and face “disciplinary proceedings leading to dismissal” for having the effrontery to raise such issues in a public place. Louise Bimpson, the corporate director of our ever-expanding human resources team, admitted that this response might appear “severe” but pointed out that Poppleton was eager to follow the disciplinary practices set by such soon-to-be members of the prestigious Russell Group as Queen Mary. Thus it was only to be expected that we would seek to emulate its espousal of draconian censorship. She hoped this clarified the situation. |
David Bignell, emeritus professor of zoology at Queen Mary hit the nail on the head.
"These managers worry me. Too many are modest achievers, retired from their own studies, intoxicated with jargon, delusional about corporate status and forever banging the metrics gong. Crucially, they don’t lead by example."
What the managers at Queen Mary have failed to notice is that the best academics can choose where to go.
People are being told to pack their bags and move out with one day’s notice. Access to journals stopped, email address removed, and you may need to be accompanied to your (ex)-office. Good scientists are being treated like criminals.
What scientist in their right mind would want to work at QMUL, now that their dimwitted assessment methods, and their bullying tactics, are public knowledge?
The responsibility must lie with the principal, Simon Gaskell. And we know what the punishment is for bringing your university into disrepute.
Follow-up
Send an email. You may want to join the many people who have already written to QMUL’s principal, Simon Gaskell (principal@qmul.ac.uk), and/or to Sir Nicholas Montagu, Chairman of Council, n.montagu@qmul.ac.uk.
Sunday 1 July 2012. Since this blog was posted after lunch on Friday 29th June, it has had around 9000 visits from 72 countries. Here is one of 17 maps showing the origins of 200 of the hits in the last two days

The tweets about QMUL are collected in a Storify timeline.
I’m reminded of a 2008 comment, on a post about the problems imposed by HR, In-human resources, science and pizza.
Thanks for that – I LOVED IT. It’s fantastic that the truth of HR (I truly hate that phrase) has been so ruthlessly exposed. Should be part of the School Handbook. Any VC who stripped out all the BS would immediately retain and attract good people and see their productivity soar.
That’s advice that Queen Mary should heed.
Part of the reason for that popularity was Ben Goldacre’s tweet, to his 201,000 followers
“destructive, unethical and crude metric incentives in academia (spotlight QMUL) bit.ly/MFHk2H by @david_colquhoun”
3 July 2012. I have come by a copy of this email, which was sent to Queen Mary by a senior professor from the USA (word travels fast on the web). It shows just how easy it is to destroy the reputation of an institution.
|
Sir Nicholas Montagu, Chairman of Council, and Principal Gaskell, I was appalled to read the criteria devised by your University to evaluate its faculty. There are so flawed it is hard to know where to begin. Your criteria are antithetical to good scientific research. The journals are littered with weak publications, which are generated mainly by scientists who feel the pressure to publish, no matter whether the results are interesting, valid, or meaningful. The literature is flooded by sheer volume of these publications. Your attempt to require “quality” research is provided by the requirement for publications in “high Impact Factor” journals. IF has been discredited among scientists for many reasons: it is inaccurate in not actually reflecting the merit of the specific paper, it is biased toward fields with lots of scientists, etc. The demand for publications in absurdly high IF journals encourages, and practically enforces scientific fraud. I have personally experienced those reviews from Nature demanding one or two more “final” experiments that will clinch the publication. The authors KNOW how these experiments MUST turn out. If they want their Nature paper (and their very academic survival if they are at a brutal, anti-scientific university like QMUL), they must get the “right” answer. The temptation to fudge the data to get this answer is extreme. Some scientists may even be able to convince themselves that each contrary piece of data that they discard to ensure the “correct” answer is being discarded for a valid reason. But the result is that scientific misconduct occurs. I did not see in your criteria for “success” at QMUL whether you discount retracted papers from the tally of high IF publications, or perhaps the retraction itself counts as yet another high IF publication! Your requirement for each faculty to have one or more postdocs or students promotes the abusive exploitation of these individuals for their cheap labor, and ignores the fact that they are being “trained” for jobs that do not exist. The “standards” you set are fantastically unrealistic. For example, funding is not graded, but a sharp step function – we have 1 or 2 or 0 grants and even if the average is above your limits, no one could sustain this continuously. Once you have fired every one of your faculty, which will almost certainly happen within 1-2 rounds of pogroms, where will you find legitimate scientists who are willing to join such a ludicrous University? |
4 July 2012.
Professor John F. Allen is Professor of Biochemistry at Queen Mary, University of London, and distinguished in the fields of Photosynthesis, Chloroplasts, Mitochondria, Genome function and evolution and Redox signalling. He, with a younger colleague, wrote a letter to the Lancet, Queen Mary: nobody expects the Spanish Inquisition. It is an admirable letter, the sort of thing any self-respecting academic should write. But not according to HR. On 14 May, Allen got a letter from HR, which starts thus.
|
14th May 2012 Dear Professor Allen I am writing to inform you that the College had decided to commence a factfinding investigation into the below allegation: That in writing and/or signing your name to a letter entitled "Queen Mary: nobody expects the Spanish Inquisition," (enclosed) which was published in the Lancet online on 4th May 2012, you sought to bring the Head of School of Biological and Chemical Sciences and the Dean for Research in the School of Medicine and Dentistry into disrepute. . . . . Sam Holborn |
Download the entire letter. It is utterly disgraceful bullying. If anyone is bringing Queen Mary into disrepute, it is Sam Holborn and the principal, Simon Gaskell.
Here’s another letter, from the many that have been sent. This is from a researcher in the Netherlands.
|
Dear Sir Nicholas,
I am addressing this to you in the hope that you were not directly involved in creating this extremely stupid set of measures that have been thought up, not to improve the conduct of science at QMUL, but to cheat QMUL’s way up the league tables over the heads of the existing academic staff. Others have written more succinctly about the crass stupidity of your Human Resources department than I could, and their apparent ignorance of how science actually works. As your principal must bear full responsibility for the introduction of these measures, I am not sending him a copy of this mail. I am pretty sure that his “principal” mail address will no longer be operative. We have had a recent scandal in the Netherlands where a social psychology professor, who even won a national “Man of the Year” award, as well as as a very large amount of research money, was recently exposed as having faked all the data that went into a total number of articles running into three figures. This is not the sort of thing one wants to happen to one’s own university. He would have done well according to your REF .. before he was found out. Human Resources departments have gained too much power, and are completely incompetent when it comes to judging academic standards. Let them get on with the old dull, and gobbledigook-free, tasks that personnel departments should be carrying out. |
5 July 2012.
Here’s another letter. It’s from a member of academic staff at QMUL, someone who is not himself threatened with being fired. It certainly shows that I’m not making a fuss about nothing. Rather, I’m the only person old enough to say what needs to be said without fear of losing my job and my house.
|
Dear Prof. Colquhoun,
I am an academic staff member in SBCS, QMUL. I am writing from my personal email account because the risks of using my work account to send this email are too great. I would like to thank you for highlighting our problems and how we have been treated by our employer (Queen Mary University of London), in your blog. I would please urge you to continue to tweet and blog about our plight, and staff in other universities experiencing similarly horrific working conditions. I am not threatened with redundancy by QMUL, and in fact my research is quite successful. Nevertheless, the last nine months have been the most stressful of all my years of academic life. The best of my colleagues in SBCS, QMUL are leaving already and I hope to leave, if I can find another job in London. Staff do indeed feel very unfairly treated, intimidated and bullied. I never thought a job at a university could come to this.
Thank you again for your support. It really does matter to the many of us who cannot really speak out openly at present.
Best regards,
|
In a later letter, the same person pointed out
"There are many of us who would like to speak more openly, but we simply cannot."
"I have mortgage . . . . Losing my job would probably mean losing my home too at this point."
"The plight of our female staff has not even been mentioned. We already had very few female staff. And with restructuring, female staff are more likely to be forced into teaching-only contracts or indeed fired"."
"total madness in the current climate – who would want to join us unless desperate for a job!"
“fuss about nothing” – absolutely not. It is potentially a perfect storm leading to teaching and research disaster for a university! Already the reputation of our university has been greatly damaged. And senior staff keep blaming and targeting the “messengers"."
6 July 2012.
Througn the miracle of WiFi, this is coming from Newton, MA. The Lancet today has another editorial on the Queen Mary scandal.
"As hopeful scientists prepare their applications to QMUL, they should be aware that, behind the glossy advertising, a sometimes harsh, at times repressive, and disturbingly unforgiving culture awaits them."
That sums it up nicely.
24 July 2012. I’m reminded by Nature writer, Richard van Noorden (@Richvn) that Nature itself has wriiten at least twice about the iniquity of judging people by impact factors. In 2005 Not-so-deep impact said
"Only 50 out of the roughly 1,800 citable items published in those two years received more than 100 citations in 2004. The great majority of our papers received fewer than 20 citations."
"None of this would really matter very much, were it not for the unhealthy reliance on impact factors by administrators and researchers’ employers worldwide to assess the scientific quality of nations and institutions, and often even to judge individuals."
And, more recently, in Assessing assessment” (2010).
29 July 2012. Jonathan L Rees. of the University of Edinburgh, ends his blog:
"I wonder what career advice I should offer to a young doctor circa 2012. Apart from not taking a job at Queen Mary of course. "
How to select candidates
I have, at various times, been asked how I would select candidates for a job, if not by counting papers and impact factors. This is a slightly modified version of a comment that I left on a blog, which describes roughly what I’d advocate
After a pilot study the entire Research Excellence Framework (which attempts to assess the quality of research in every UK university) made the following statement.
“No sub-panel will make any use of journal impact factors, rankings, lists or the perceived standing of publishers in assessing the quality of research outputs”
It seems that the REF is paying attention to the science not to bibliometricians.
It has been the practice at UCL to ask people to nominate their best papers (2 -4 papers depending on age). We then read the papers and asked candidates hard questions about them (not least about the methods section). It’s a method that I learned a long time ago from Stephen Heinemann, a senior scientist at the Salk Institute. It’s often been surprising to learn how little some candidates know about the contents of papers which they themselves select as their best. One aim of this is to find out how much the candidate understands the principles of what they are doing, as opposed to following a recipe.
Of course we also seek the opinions of people who know the work, and preferably know the person. Written references have suffered so much from ‘grade inflation’ that they are often worthless, but a talk on the telephone to someone that knows both the work, and the candidate, can be useful, That, however, is now banned by HR who seem to feel that any knowledge of the candidate’s ability would lead to bias.
It is not true that use of metrics is universal and thank heavens for that. There are alternatives and we use them.
Incidentally, the reason that I have described the Queen Mary procedures as insane, brainless and dimwitted is because their aim to increase their ratings is likely to be frustrated. No person in their right mind would want to work for a place that treats its employees like that, if they had any other option. And it is very odd that their attempt to improve their REF rating uses criteria that have been explicitly ruled out by the REF. You can’t get more brainless than that.
This discussion has been interesting to me, if only because it shows how little bibliometricians understand how to get good science.